Primary Xanthoma of Ulnar Bone in a Normolipemic Patient
Prachi Nayak1, Nidhi Shukla2, Raj Narain Srivastava3, Premala Anthony Singh4, Kapil Kulshreshta5
1 Consultant Pathologist, Department of Pathology, Anoop Labs Pvt Ltd, Allahabad, Uttar Pradesh, India.
2 Consultant Pathologist, Department of Pathology, Anoop Labs Pvt Ltd, Allahabad, Uttar Pradesh, India.
3 Consultant Pathologist, Department of Pathology, Anoop Labs Pvt Ltd, Allahabad, Uttar Pradesh, India.
4 Consultant Pathologist, Department of Pathology, Anoop Labs Pvt Ltd, Allahabad, Uttar Pradesh, India.
5 Orthopaedic Surgeon, Department of Orthopaedic Surgery, Yashlok Hospital and Research Centre, Allahabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prachi Nayak, 55-B, Lowther Road, Near Medical College, Allahabad-211001, Uttar Pradesh, India.
E-mail: dr.prachinayak87@gmail.com
Xanthoma of bone is an exceedingly rare primary bone lesion. It is generally known that bone xanthomas are associated with hyperlipidemia. Non-hyperlipidemic xanthomas are very rare. Radiologically it presents as well-defined osteolytic lesion thus mimicking benign bone tumours. Definitive diagnosis is based mainly on histopathology. Histologically, presence of sheets of foamy macrophages with multinucleated giant cells and cholesterol clefts at places confirms the diagnosis of xanthoma. Surgical curettage followed by bone grafting is curative. We report a case of skeletal xanthoma in ulnar bone of a non-hyperlipidemic patient.
Foamy macrophages, Non-hyperlipidemia, Osteolytic
Case Report
A 28-year-old female presented with a clicking sensation followed by pain in the right forearm after mild physical activity. On examination, there was a diffuse swelling and tenderness in the right forearm but no local warmth or redness was apparent. The range of motion of the elbow joint was not restricted. No neurological abnormalities were noted. Routine haematological parameters were within normal limits except for Erythrocyte Sedimentation Rate (ESR) which was mildly raised (22mm). Liver function test, kidney function test and blood sugar of the patient were requested but did not present any alteration.
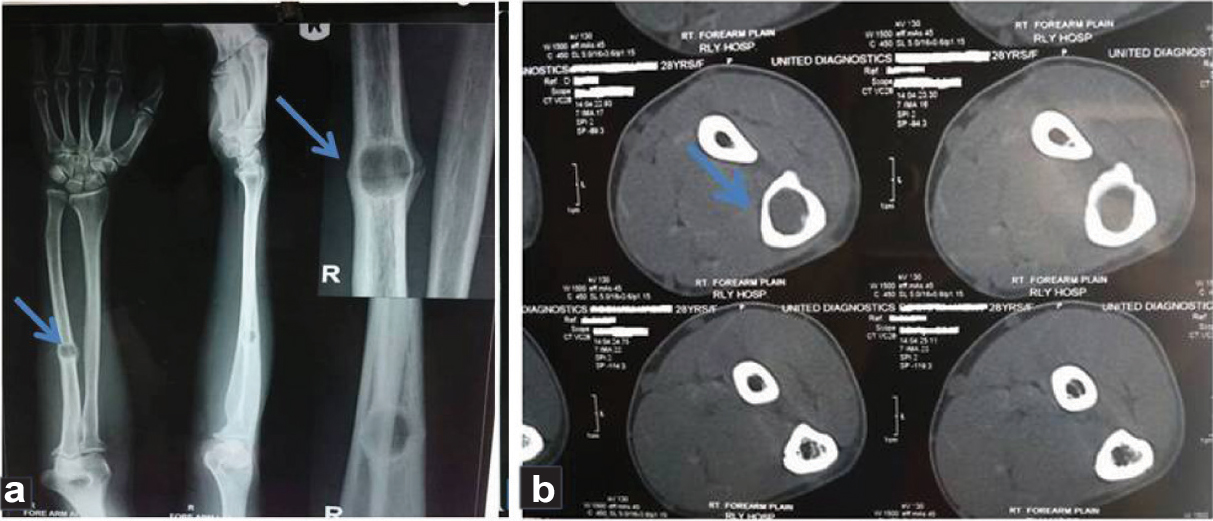
X-Ray imaging of the right forearm showed a clearly demarcated well defined osteolytic lesion with sclerotic margins involving the cortex and medullary region of mid diaphysis of ulna with cortical breach and solid type periosteal reaction. Findings suggested benign bone disease [Table/Fig-1a]. Computed tomography of the right forearm showed a well circumscribed expansile hypodense lesion of size 10 x 14 x 16 mm in mid diaphysis of right ulna. Sharply defined scalloped margins causing mild endosteal scalloping, expansion of overlying cortex without any cortical erosion was seen. No intralesional calcification or periosteal reaction was seen. No paracortical soft tissue was noted. A transverse thin fracture was seen at the same site. Rest of the visualized bones were normal with intact cortical outlines. Bone density was normal [Table/Fig-1b]. Possibility of enchondroma with pathological fracture was suggested.
a) X-ray forearm (preoperative): showing a clearly demarcated osteolytic lesion with sclerotic margins involving the cortex and medulla of mid diaphysis of right ulna; b) CT forearm– showing a well circumscribed expansile hypodense lesion in mid diaphysis of right ulna.
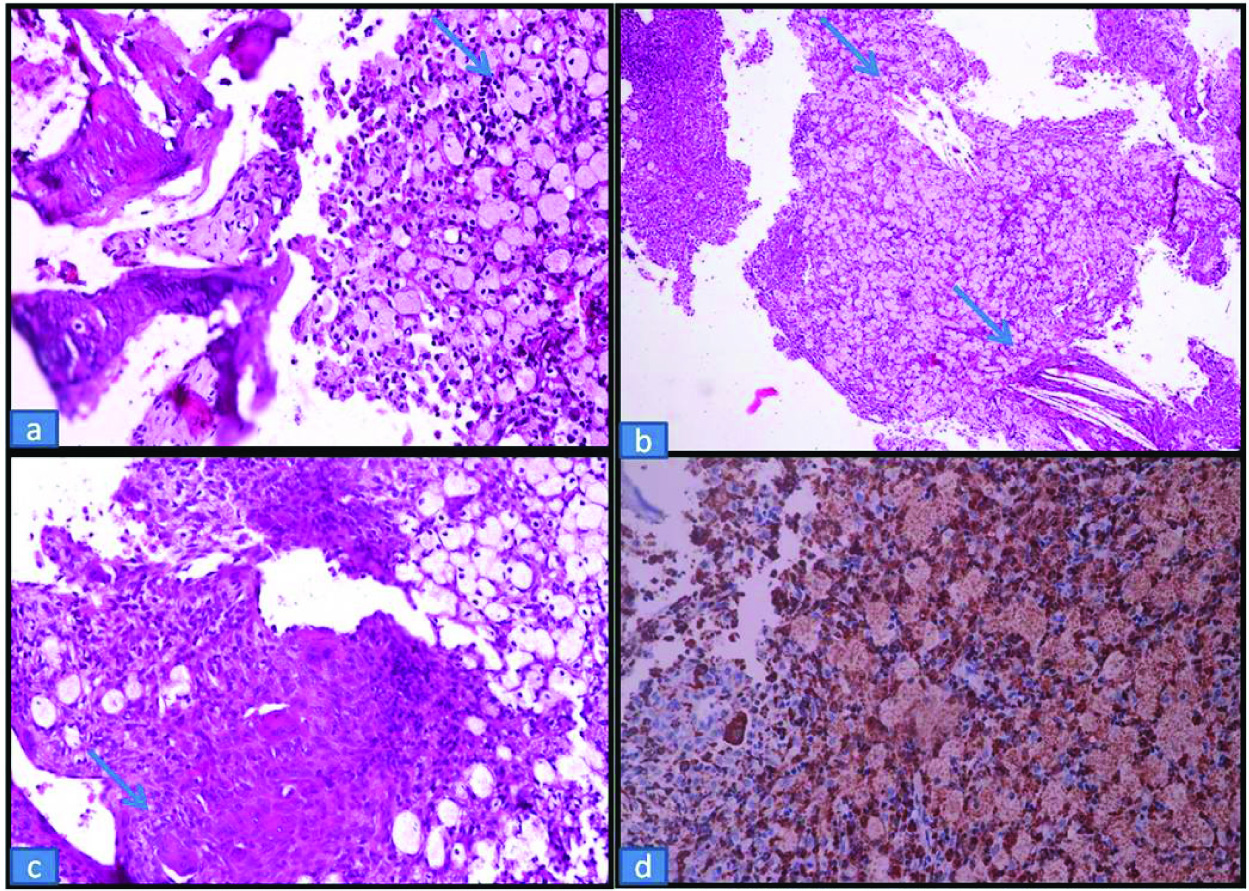
Based on radiological findings, bone curettage was done and specimen was sent for histopathological examination. A few small irregular yellowish white pieces of tissue were received. The tissue was processed and on microscopic examination biopsy material showed sheets of large histiocytic cells with central to eccentric nuclei, pink granular cytoplasm in a background of mixed inflammatory cells, fibrous tissue and spicules of bone [Table/Fig-2a]. At places few cholesterol clefts [Table/Fig-2b] and foreign body giant cells were also seen [Table/Fig-2c]. Histopathological findings suggested xanthoma of ulnar bone. Considering the histology of the sample received, the patient serum was submitted for lipid profile which was completely within the normal limits. There was no sign of hyperlipidemia or lipid disorder. On immunohistochemical staining, these histocytic cells were strongly positive for CD68 [Table/Fig-2d]. At the same time cytokeratin, CD1a, Langerin and S-100 were negative. Thus, we confirmed the diagnosis of primary bone xanthoma without hyperlipidemia.
a) Histological findings (H&E, 40X); histiocytic cells with central to eccentric nuclei, pink granular cytoplasm along with bone spicules; b) Histological findings, (H&E, 10X), histiocytic cells with cholesterol clefts; c) Histological findings, (H&E, 10X); histiocytic cells with multinucleated giant cells; d) Immunohistochemistry, 40X, histiocytic cells showing strong positivity for CD68.
The patient subsequently underwent bone curettage followed by bone grafting and stabilization of fracture site by internal fixator [Table/Fig-3]. Bone graft was taken from iliac bone. The patient is under clinical and radiographic follow up for six months with no signs or symptoms of recurrence.
X-ray forearm (postoperative): showing fracture fixation by internal fixator.

Discussion
Xanthoma is a reactive proliferation and localized collection of lipid laden tissue histiocytes. Most common site of xanthoma is skin and subcutaneous tissue but occasionally it involves deeper soft tissues like tendons and synovium [1]. Bone involvement in xanthoma is extremely rare [1,2]. Most common location of skeletal xanthoma is ilium and femur followed by ribs, skull, vertebral bodies, humerus, tibia and small bones of hand [3]. Only two cases of ulnar xanthoma have been reported so far in the literature [2].
Xanthomas usually occur in hyperlipidemic state which could be primary (essential or familial) or secondary to primary biliary cirrhosis, diabetes mellitus, nephrotic syndrome, hypothyroidism, alcohol abuse or medications like oestrogen, corticosteroid and retiniods [1,4]. Only few cases of xanthoma are reported in normolipemic patients [2]. Skeletal xanthoma in ulnar bone with no cutaneous or soft tissue involvement in a normolipemic patient makes our case unique and rare entity.
Xanthoma of bone is a benign bone disorder which occurs due to abnormal deposition of cholesterol in bone [5]. Usual age of presentation is around 20 years with male preponderance [6]. Xanthoma typically occurs in hyperlipidemic patients due to dysregulated macrophage sterol flux or disturbed macrophage sterol reflux. Normolipemic xanthomas are either idiopathic or associated with abnormal apoprotein, lymphoproliferative disorders or they are post-traumatic [4]. On x-ray imaging, skeletal xanthomas appear as osteolytic lesion with cortical expansion or disruption and thus mimic primary bone tumours and metastatic deposits [7]. So, final diagnosis depends mainly on histopathology. Histologically, xanthomas are characterized by abundant foamy macrophages and focal cholesterol clefts and multinucleated giant cells. Scattered polymorphs and fibrous connective tissue is also observed [6,7]. Microscopic differentials of the case included langerhans cell histiocytosis, Erdheim-Chester disease, Rosai-Dorfman disease [6,7].
Langerhans cell histiocytosis is a clonal disorder characterized by histiocytes with coffee bean nucleus (unlike xanthomas) in a background of inflammatory cells. On immunophenotyping cells are CD1a and langerin positive which is negative in xanthoma [6].
Erdheim-Chester disease is a multifocal disease with xanthogranulomatous histiocytosis. Lesion is characterized by histiocytosis, touton giant cells, reactive fibrosis and chronic inflammatory cells. It is not found in xanthomas [8].
Rosai-Dorfman disease is a polyclonal histiocytic disorder with characteristic feature of emperipolesis which is not seen in xanthomas. Secondly bone involvement is very rare in Rosai-dorfman disease. On immunophenotyping, histiocytes are strongly positive for CD68 and S-100. However, macrophages in xanthomas are S-100 negative [6].
Treatment of choice in skeletal xanthoma is bone curettage with bone grafting with very good prognosis [7]. Medical treatment in the form of statins can be given in hyperlipidemic patients [5].
Conclusion
Skeletal xanthoma is an extremely rare cause of pathological fracture. We report a case of primary xanthoma of ulnar bone because of its rare site of occurrence with rare presentation in normolipidemic patient. Imaging shows osteolytic lesion mimicking primary bone tumour. Histopathology plays a key role in diagnosis. It is very important to evaluate whole specimen carefully to rule out primary bone tumour with xanthomatous degeneration and to confirm primary xanthoma in bone. Skeletal xanthomas are important because its clinicoradiological features mimic bone tumours and it is very difficult to reach definitive diagnosis before surgery.
[1]. Weiss SW, Goldblum JR, Enzinger and Weiss’s Soft Tissue Tumours 2008 5th edChinaMosby Elsevier [Google Scholar]
[2]. Yaligod V, Mahesh S, Rudrappa GH, Choudhary L, Xanthoma of ulnaJournal of evolution of medical and dental sciences 2013 2(35):6691-95. [Google Scholar]
[3]. Forest M, Tomeno B, Vanel D, Orthopedic surgical pathology: Diagnosis of tumours and pseudotumoural lesions of bone and joints 1998 EdinburghChurchill Livingstone [Google Scholar]
[4]. Elder DE, Lever’s histopathology of the skin 2008 10th edPhiladelphiaLippincott Williams and Wilkins [Google Scholar]
[5]. Guerrouj H, Mouaden A, BenRais N, Xanthoma of Bone: A case reportCase reports in endocrinology 2012 2012:1-3. [Google Scholar]
[6]. Wang Z, Lin ZW, Huang LL, Ke ZF, Luo CJ, Xie WL, Primary non-hyperlipidemia xanthoma of bone: A case report with review of the literatureInt J Clin Exp Med 2014 7(11):4503-08. [Google Scholar]
[7]. Chakravarthi VK, Aruna E, Rao DNC, Rao DR, Bilateral tibial xanthoma in a normolipidemic patient - report a rare case with review of literatureInt. J of Clin Med 2012 3:234-37. [Google Scholar]
[8]. Abdelfattah AM, Arnaout K, Tabbara IA, Erdheim-chester disease: A comprehensive reviewAnticancer Res 2014 34:3257-61. [Google Scholar]