Monteggia Type 1 Fracture Equivalent with Concomitant Ipsilateral Distal Radius and Ulna Fracture in an Adult: A Rare Case Report
Shankarlinga S Sajjan1, Atmananda S Hegde2, Rajendra Annappa3, Sharan Mallya4
1 Junior Resident, Department of Orthopaedics, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
2 Associate Professor, Department of Orthopaedics, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
3 Assistant Professor, Department of Orthopaedics, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
4 Senior Resident, Department of Orthopaedics, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajendra Annappa, 602, Shakti Palace, Kodialguttu East Road, Kodialbail, Mangaluru-575003, Karnataka, India.
E-mail: rajendra.orthopaedics@gmail.com
Monteggia fracture comprises of 5% to 10% of all forearm fractures. It represents severe forearm injuries which require operative intervention. We report a unique case of Monteggia variant in female patient aged 67-year-old presenting a fracture of proximal ulna and radial neck along with ipsilateral fracture of distal ulna and radius at its metaphyseal end, which cannot be classified under Monteggia fracture and its equivalents occurring in adults. We managed this case using dorsal approach surgically and patient had good functional result at the end of six months.
Monteggia variants, Proximal ulna fracture, Radial head dislocation
Case Report
A 67-year-old female patient presented to the Emergency Department with alleged history of slip and fall at her residence three days back. She sustained trauma when she had a fall on outstretched hand to her right forearm, following which she developed severe pain, swelling and restriction of movement at the right elbow and wrist joint.
On examination, there was varus deformity at the right elbow along with swelling, tenderness and bony crepitus at the elbow and the wrist joint. There was no distal neurovascular deficit.
Radiographs of right elbow, forearm and wrist revealed fractures of proximal ulna and radial neck along with distal ulna and radius fractures at metaphyseal end [Table/Fig-1]. Radial neck fracture was undisplaced. Proximal ulna fracture was laterally displaced and angulated. Distal radius fracture was dorsally displaced; dorsally angulated and proximal shift was present with comminuted fracture of ulnar head.
Preoperative radiograph showing: fracture of proximal ulna with fracture of radial head and neck.

The forearm was immobilised in an above elbow slab. It was decided to treat surgically after obtaining medical fitness and informed consent. Under general anaesthesia, using dorsal approach, open reduction and internal fixation of proximal ulna fracture with reconstruction plate was done. Radial head excision was done. Closed reduction and Kirschner wire (K-wire) fixation of distal end of radius and ulna were done to restore the distal radio-ulnar joint. Postoperatively forearm was immobilised in an above elbow slab [Table/Fig-2].
Immediate postoperative radiograph-proximal ulna fixation, radial head excision, and distal radius fixation.
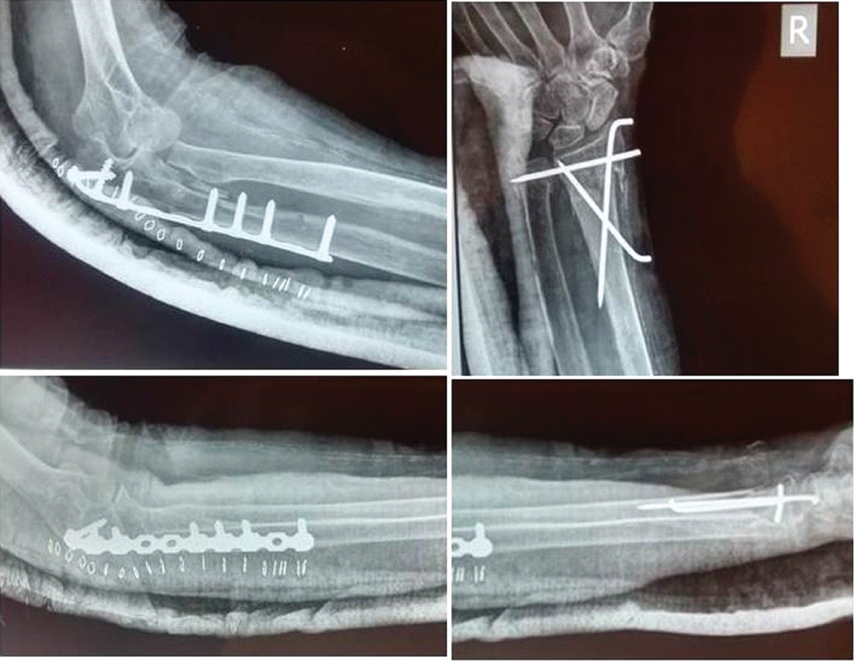
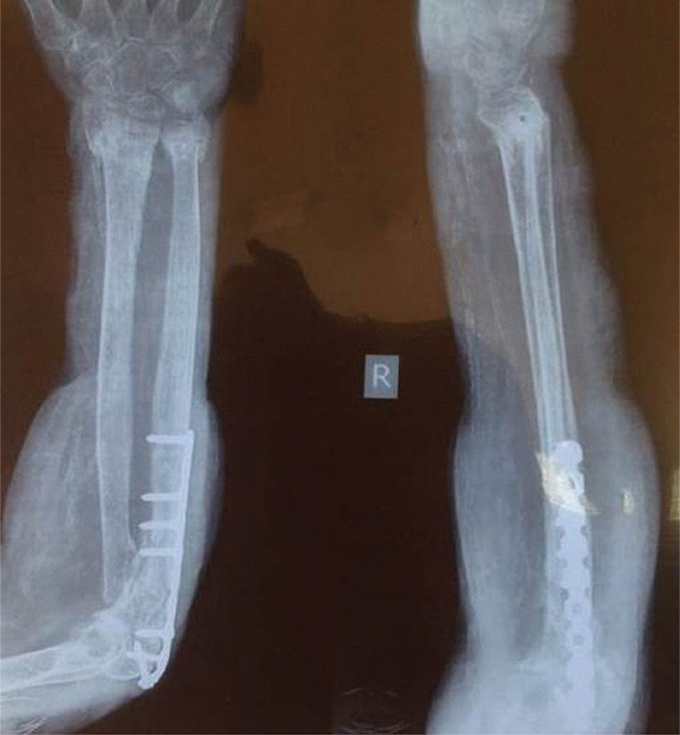
Postoperative period was uneventful and patient was discharged on 3rd postoperative day and was asked to review for follow up regularly. At three weeks follow up above elbow slab was removed and gentle, active mobilisation of elbow and wrist was started. At six weeks follow up later, the fractures had united both clinically and radiologically [Table/Fig-3]. K-wires were removed, active and passive mobilisation of elbow and wrist joint were continued. Later, at 12 weeks follow up, she had achieved near complete range of flexion and extension of elbow, supination and pronation of forearm, and palmar and dorsiflexion of wrist joint [Table/Fig-4,5].
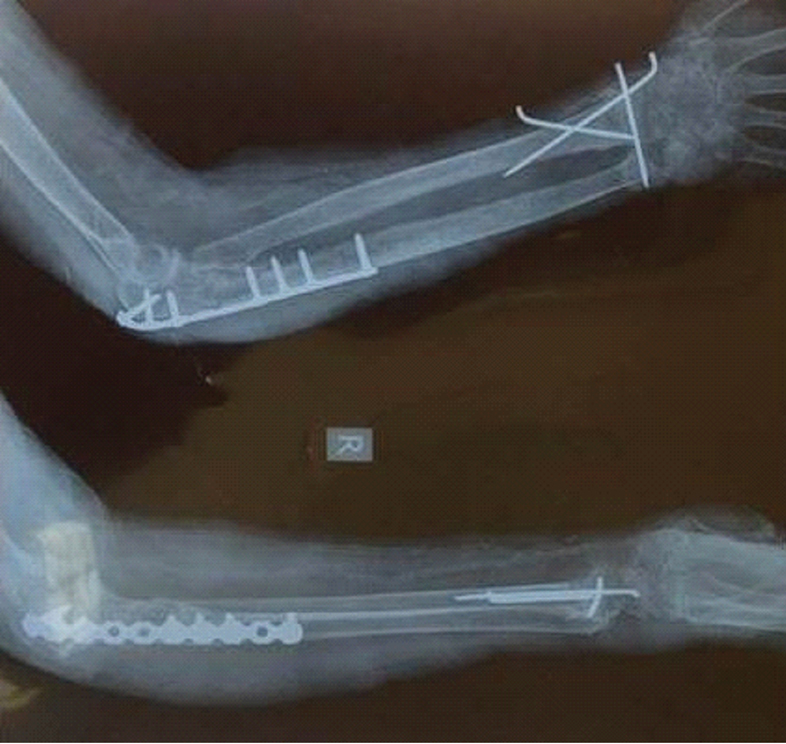
Radiograph at 3 months showing fracture union.
Clinical picture at 6 months- showing range of movements at elbow and wrist joint.

Discussion
In 1967, Monteggia fracture was systematically studied and classified by Bado JL [1]. Forearm fractures account for 1% of all fractures [2]. Monteggia fractures comprise 5%-10% of all forearm fractures which is commonly seen in middle aged individuals affecting both sexes equally. Many injuries are reported in literature which cannot be characterised into Monteggia lesion and are called Monteggia equivalents or variants [2-4].
Monteggia fracture dislocation must be evaluated thoroughly regarding the mechanism of injury and forces involved patient’s age, comorbidities, functional demands and dominance of upper limb. Neurological status of the limb should be assessed [4]. High incidence of posterior interosseous nerve has been reported due to stretching of the nerve by dislocated head. Whenever, required computed tomography including 3D reconstructions can be obtained to assess fracture geometry and plan surgery [3-5].
Meticulous preoperative planning is required for surgery. Templating with X-ray of normal side is necessary for intraoperative reconstruction and implant selection. All varieties of implants should be available which includes K-wires, Herbert screws, mini plates for fixation of radial head fractures, radial head implants, suture anchors, Limited Contact Dynamic Compression Plates (LC-DCP) and 4 mm cannulated screws [3,5].
Dorsal approach is preferred for ulna and can be used for radial head fracture, if required. Anatomical reduction and rigid fixation of ulna is mandatory. This will allow reduction and maintenance of radial head [3]. Contoured plates or olecranon fixation plates can be used for a proximal fracture which allows more screws in proximal fragment and dorsal situation reduces the chance of failure of fixation. After fixation ulna, a true lateral view of elbow should be checked intraoperatively to assess radial head reduction. If ulna fracture is not anatomically reduced or there is soft tissue interposition, radial head fails to reduce. Management of radial head fracture when present is controversial. Options include fixation, excision or replacement. Radial head fractures are usually fixed with miniplates and headless screws [3,4].
In this case, female patient aged 67 years presented with fracture of proximal ulna and radial neck which can be considered Monteggia equivalent type 1 along with ipsilateral distal ulna and radius fracture. We managed this case using dorsal approach surgically and patient had reasonable functional result at end of six months. To the best of the author’s knowledge, there have been no reports in the literature of cases with exactly the same combination of injuries.
Monteggia fracture dislocations with radial head fractures have been reported to have lesser motion and poor functional results compared to patients with intact radial heads. Konrad GG et al., reported four Mason type III fractures which were treated with primary excision with two patients requiring revision fixation for loss of the initial fracture reduction [2]. Radial head fractures were correlated with a “poor” Broberg–Morrey score, but no difference in scores could be determined between the fixation and excision groups. Matar et al., studied 18 Monteggia fractures with radial head fractures. Radial head replacement was done to achieve joint stability in 9 patients with excellent to good results in 6 cases [6]. Monteggia fractures dislocation associated with ipsilateral distal radial physical injuries have been described in literature in children. This type of injury is reported rarely in adults [2,6,7].
Recognising the injury pattern and addressing all components of the injury as well as achieving elbow stability, restoring the length of the ulna and obtaining accurate and fixation of any coronoid fracture plays an important role in the adequate management of this significant but relatively uncommon injury is must for satisfactory results [2,6].
This report throws light on a rare injury pattern involving the forearm bones which emphasizes on the importance of awareness of possibility of various combinations of fractures when presenting with a fall on outstretched forearm. A better prognosis can be ensured by early diagnosis and prompt intervention owing to the severity of the injury and its complications.
Conclusion
Despite the typical pattern of Monteggia fracture seen in patients presenting with the above history, awareness of certain rare types will help in avoiding faulty management due to prejudice.
[1]. Bado JL, The Monteggia lesionClin Orthop Relat Res 1967 50:71-86. [Google Scholar]
[2]. Konrad GG, Kundel K, Kreuz PC, Oberst M, Sudkamp NP, Monteggia fractures in adultsJ Bone Joint Surg Br 2007 89(3):354-60. [Google Scholar]
[3]. Shew PC, Leung F, Radius and Ulnar shaft Fractures. In: Bucholz RW, Court-Brown CM, Heckman JD, Tornetta PRockwood and Green’s fractures in adults 2010 7th editionPhiladelphiaLippincott Williams and Wilkins:1731-54. [Google Scholar]
[4]. Eathiraju S, Mudgal SC, Jupiter BJ, Monteggia fracture-dislocationsHand Clin 2007 23(2):165-77. [Google Scholar]
[5]. Arora S, Sabat D, Verma A, Sural S, Dhal A, An unusual monteggia equivalent: a case report with literature reviewJ Hand Microsurg 2011 3(2):82-85. [Google Scholar]
[6]. Matar H E, Akimau P, Stanley D, Ali AA, Surgical treatment of Monteggia variant fracture dislocations of the elbow in adults: surgical technique and clinical outcomesEur J Orthop Surg Traumatol 2017 :1953-55. [Google Scholar]
[7]. Kembhavi RS, James B, Type II A Monteggia fracture dislocation with ipsilateral distal radius fracture in adult - a rare associationJ Clin Diagn Res 2016 10(8):RD01-RD03. [Google Scholar]