Paramolar with a Parapremolar: A Rare Occurrence
Pankaj Prasad1, Shikha Ahirwal2, Vikas Kumar3, Mohit Singh Chauhan4, Priyanka Rathor5
1 Consultant, Department of Conservative Dentistry and Endodontics, Government Dental College, Jaipur, Rajasthan, India.
2 Postgraduate Student, Department of Conservative Dentistry and Endodontics, Nair Dental College, Mumbai, India.
3 Postgraduate Student, Department of Conservative Dentistry and Endodontics, Government Dental College, Jaipur, Rajasthan, India.
4 Postgraduate Student, Department of Conservative Dentistry and Endodontics, Government Dental College, Jaipur, Rajasthan, India.
5 Junior Resident, Department of Conservative Dentistry and Endodontics, Government Dental College, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pankaj Prasad, T-26, Indra Colony, Narela-110040, Delhi, India.
E-mail: pankajultimateone@gmail.com
A supernumerary tooth is an extra tooth to the normal series which can either be deciduous or permanent, single or multiple, unilateral or bilateral in any quadrant of the jaw. Identification and management of supernumerary teeth should be well understood. This case report deals with the discussion of the causes and theories related to the formation of paramolar and parapremolar and their further identification, with management of complications.
Nonsyndromic, Panoramic radiography, Premolars, Supernumerary teeth
Case Report
A 27-year-old female reported to the Department of Conservative Dentistry and Endodontics, Government dental college, Jaipur with the chief complaint of pain in the lower right back tooth region of jaw from past one month. Patient also complaint of frequent cheek biting while eating, food lodgement, itching in gum with occasional bleeding. There was no relevant familial, medical and dental history. The facial appearance was normal and presented no skeletal or other abnormalities suggestive of any syndrome.
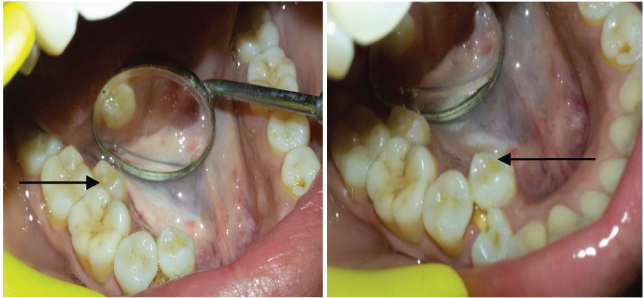
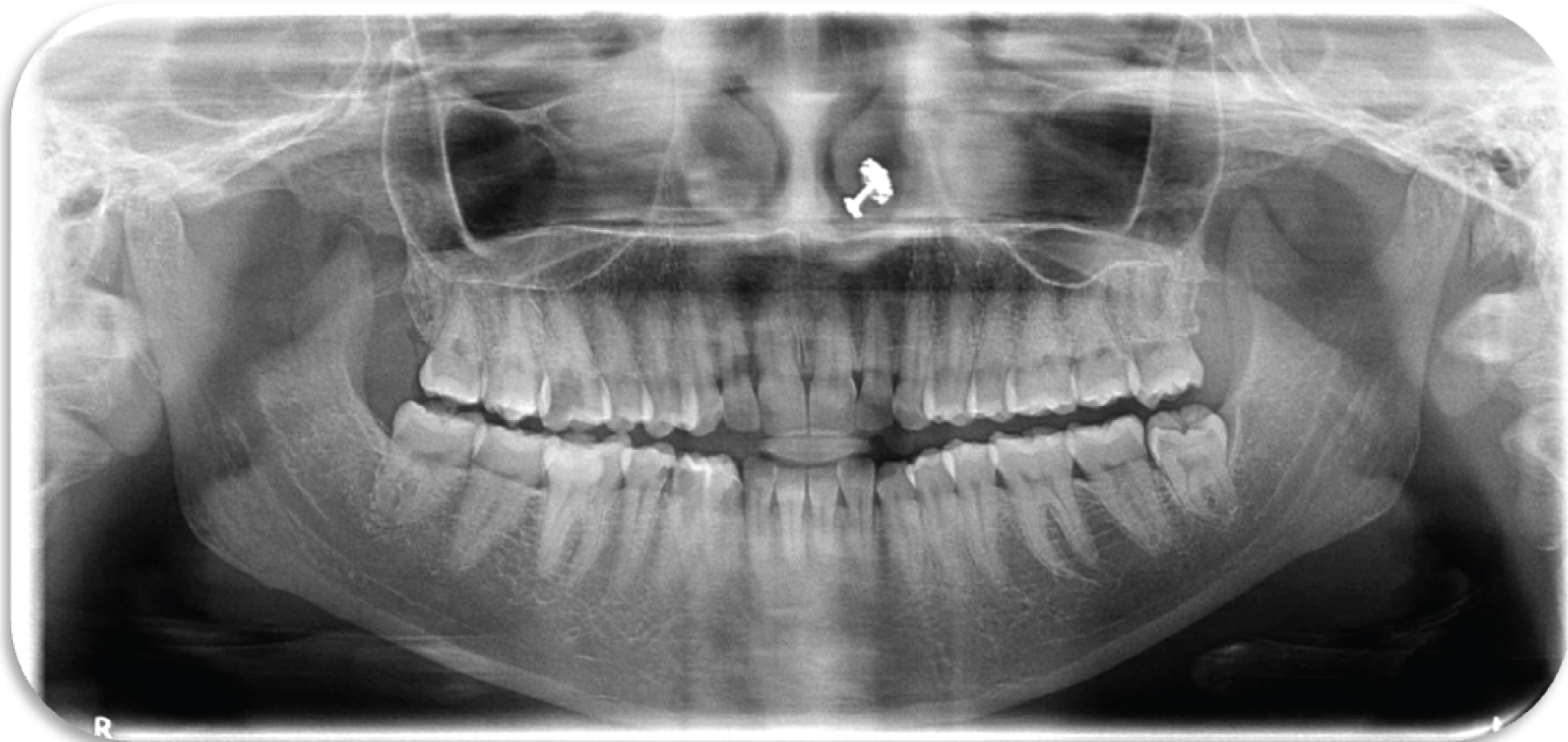
Intra oral examination revealed presence of full complement of permanent teeth along with supernumerary teeth which were present in maxillary [Table/Fig-1] and mandibular [Table/Fig-2] region on right side. A deep carious lesion which was tender on percussion was present in 44 and a distoproximal carious lesion was seen in 16. A supernumerary tooth was found in between 44 and 45 region (parapremolar) and another supernumerary tooth was present lingually w.r.t to 46 (paramolar). In maxilla, a supernumerary tooth was present buccally in relation to 16, without any displacement of the permanent teeth (paramolar). There was no underlying resorption, pathology or unerupted supernumerary teeth seen on panoramic radiographic examination [Table/Fig-3].

Paramolar in 46 region and parapremolar w.r.t 44, 45 region.
Panoramic radiograph showing multiple supernumerary teeth paramolar and parapremolar.
Patient was informed about presence of supernumerary teeth, which was the cause of her cheek biting and food lodgement. She was advised for extraction, followed by orthodontic treatment for alignment of her teeth. Patient refused for orthodontic treatment. Therefore following treatment plan was charted and patient consent was taken for same.
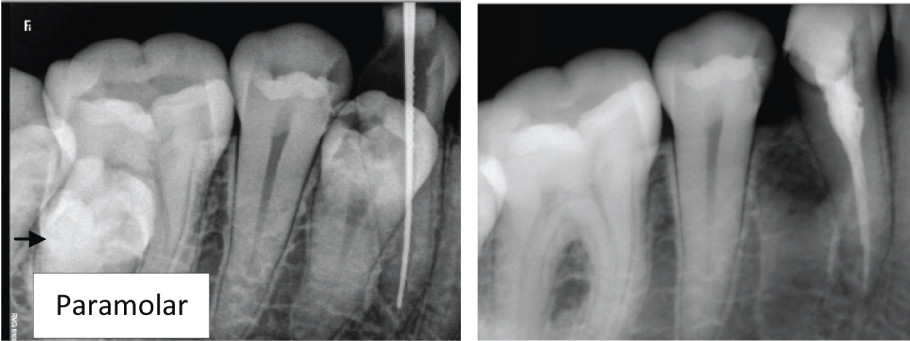
Single visit endodontic treatment was done for 44 [Table/Fig-4a,b] and composite restoration in 16.
a) Working length of 44; b) Obturated 44 and extraction socket of parapremolar.
Oral prophylaxis was also done in the same visit and chlorohexidine mouthwash was prescribed for one week.
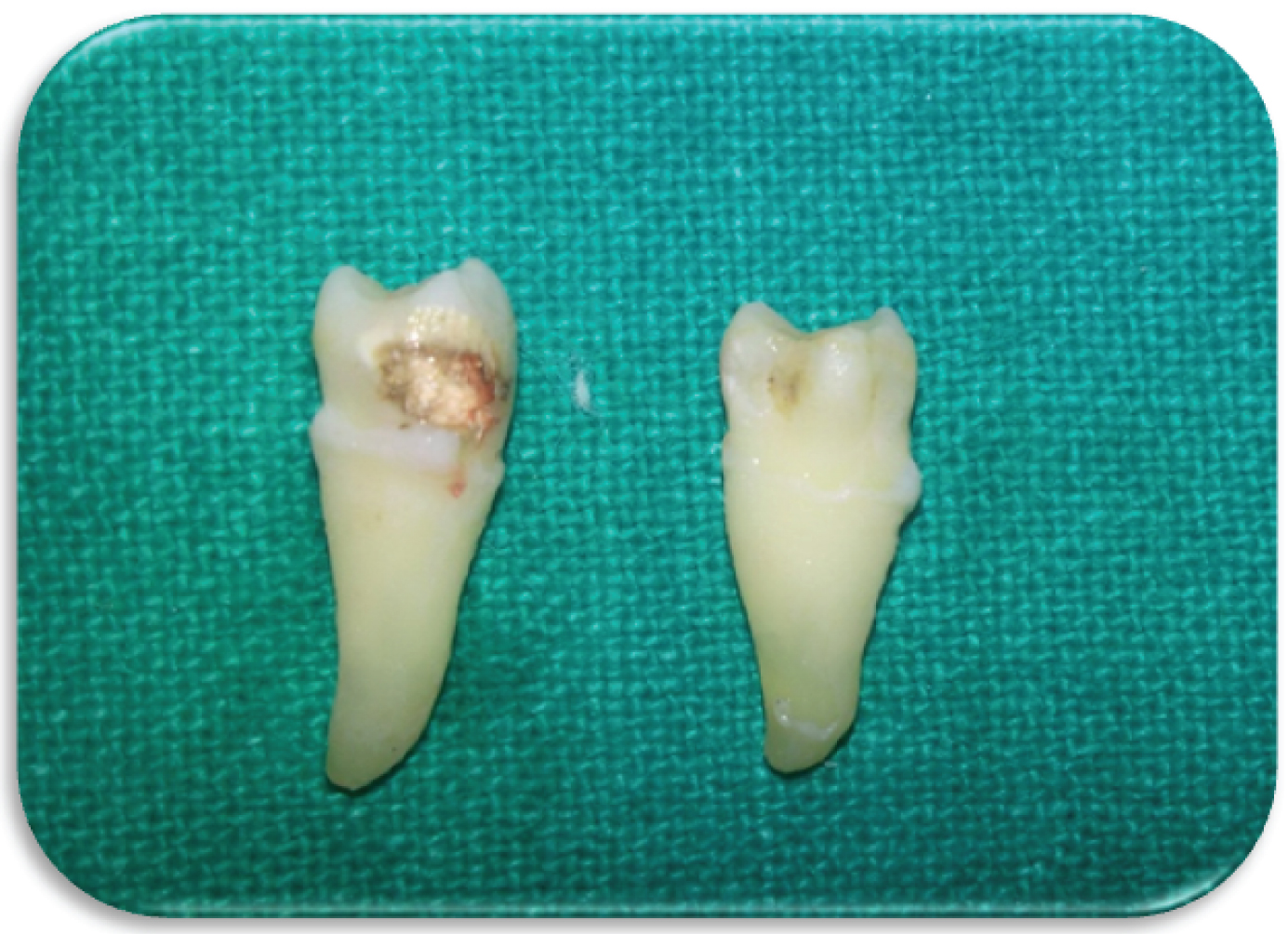
After one week, extraction of paramolar of 16 region and parapremolars [Table/Fig-5] was done under local anaesthesia.
Extracted parapremolar of 44, 45 region and maxillary paramolar 16 region.
After the completion of treatment, patient was followed up. Post treatment radiographic image shows healing socket of parapremolar [Table/Fig-4b]. Patient didn’t complaint of any pain, chewing difficulty or food lodgement in subsequent visits.
Discussion
A supernumerary tooth is an extra tooth to the normal series which can be present in any quadrants of the jaw. They can be present in one jaw or both the jaws being more prevalent in maxillary anterior region. There is no gender predilection in deciduous dentition but in case of permanent dentition males have double the chances of getting a supernumerary [1]. Many studies reported the prevalence of 0.15% to 3.8% supernumerary teeth in the permanent dentition. Single supernumerary teeth were in 76-86% of the cases, while two supernumerary teeth were found in 12-23% of the cases and three or more such teeth in the same individual found in 2-8% of cases [2].
In the above case report, we found 3 unilateral supernumerary teeth (2 paramolars and 1 parapremolar) in one individual that makes it a rare entity. According to Rajab and Hamdan, this percentage was nearly 1% when hyperdontia comprises five or more supernumerary teeth, while Açikgöz et al., reported 0.06% prevalence of multiple supernumerary teeth [3,4]. Multiple supernumerary teeth are mostly commonly in cleft-lip and palate or syndromes like cleidocranial dysplasia and Gardner’s syndrome [5].
Several theories have been suggested for occurrence of supernumerary. The “Phylogenic theory” relates to phylogenic process of atavism (evolutionary throwback) [6]. Hyperdontia is the result of the reversional phenomenon or atavism. Atavism is the return to or the appearance of an ancestral condition or type. Hence a supernumerary paramolar or parapremolar may be an atavistic appearance. The “dichotomy theory” says that supernumerary tooth is created as a result of dichotomy of the tooth bud [7]. Paramolars are often seen less in maxilla [8], rarely bilateral [9], extremely rare in primary dentition and only one such case has been reported.
Presence of supernumerary teeth leads to delayed eruption of associated permanent teeth retention or ectopic eruption of adjacent teeth, displacement or rotation of adjacent teeth, crowding, malocclusion: interdentally spacing, traumatic bite when buccally positioned paramolar causes laceration of buccal mucosa, dilaceration or delayed or abnormal root development, pulpal necrosis and root resorption of adjacent tooth due to pressure exerted by supernumerary tooth [10]. Dental caries is caused due to plaque retention in inaccessible areas as seen in our case, deeply carious parapremolar and mandibular first premolar of right side.
Most supernumerary teeth are impacted and frequently are discovered by chance during radiographic examination with no associated complications. The most useful radiographic investigation is the Orthopantomogram (OPG), with additional views of the maxilla and mandible, in the form of occlusal or peripaical radiograph. In addition, Cone-Beam Computed Tomography (CBCT) has recently been used to evaluate position of supernumerary tooth [11]. Clinical management of paramolars and parapremolars depends on its position and potential effect on the adjacent structures. Extraction or observations are the treatment modalities. Extraction is generally considered when there is failure of eruption of permanent teeth or potential complications such as crowding, cheek biting, root resorption, impaction and cyst formation. In our case extraction of both paramolar and parapremolar was carried out to facilitate proper oral hygiene and to prevent cheek biting [11].
The extraction of supernumerary teeth should be carried out cautiously, without causing any damage to the anatomical structures or to the roots of the adjacent teeth, if the supernumerary teeth are not causing any complications such as chewing difficulties or interference in orthodontic treatment, they can be monitored periodically [11].
Conclusion
Although the presence of supernumerary tooth is infrequent but the clinician should be aware of the sign and symptoms associated with a supernumerary. After performing all the required investigations and diagnosis, proper treatment plans should be made so that the patients wouldn’t get any complications later.
[1]. Kinirons MJ, Unerupted premaxillary supernumerary teeth: A study of its occurence in males and femalesBr Dent J 1982 153(3):110 [Google Scholar]
[2]. Yagüe-García J, Berini-Aytés L, Gay-Escoda C, Multiple supernumerary teeth not associated with complex syndromes: a retrospective studyMed Oral Patol Oral Cir Bucal 2009 14(7):331-36. [Google Scholar]
[3]. Rajab LD, Hamdan AM, Supernumerary teeth: Review of the literature and a survey of 152 casesInt J Paediatr Dent 2002 12(4):244-54. [Google Scholar]
[4]. Açikgöz A, Açikgöz G, Tunga U, Otan F, Characteristics and prevalence of non-syndrome multiple supernumerary teeth: a retrospective studyDentomaxillofac Radiol 2006 35(3):185-90. [Google Scholar]
[5]. Williams P, An unusual case of hyperdontiaBr Dent J 1998 184(8):371-72. [Google Scholar]
[6]. Smith JD, Hyperdontia: report of a caseJ Am Dent Assoc 1969 79(5):1191-92. [Google Scholar]
[7]. Liu JF, Characteristics pf premaxillary supernumerary teeth: a survey of 112 casesASDC J Dent child 1995 62(4):262-65. [Google Scholar]
[8]. Timocin N, Yalcin S, Ozgen M, Tanyeri H, Supernumerary molars and paramolars, A Case ReportJ Nihon Univ Sch Dent 1994 36(4):154-50. [Google Scholar]
[9]. Hou GL, Lin CC, Tsai CC, Ectopic supernumeray teeth as a predisposing cause in localized periodontics cause in localized periodontitis. Case reportAust Dent J 1995 40:226-28. [Google Scholar]
[10]. Dubuk AN, Selvig KA, Tellefsen G, Wikesjo UM, Atypically located paramolar. Report of a rare caseEur J Oral Sci 1996 104(2 Pt 1):138-40. [Google Scholar]
[11]. Nayak G, Shetty S, Inderpreet S, Pitalia D, Paramolars— a supernumerary molar: a case report and over viewDent Res J 2012 9(6):797-803. [Google Scholar]