Sacroiliac Joint Mobilisation versus Transcutaneous Electrical Nerve Stimulation for Pregnancy Induced Posterior Pelvic Pain- A Randomised Clinical Trial
Shlesha Maulik Vaidya1
1 Assistant Professor, Department of Physiotherapy, SPB Physiotherapy College, Surat, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shlesha Maulik Vaidya, 6/2546, Prashantam, Vaidya Street, Navsari-396412, Gujarat, India.
E-mail: drsmvaidya@gmail.com
Introduction
The prevalence of back pain in pregnancy is reported to be 75% especially in the last trimester, 20% of these report posterior pelvic pain.
Aim
To compare the effect of Sacroiliac Joint (SIJ) mobilisation and Transcutaneous Electrical Nerve Stimulation (TENS) on pain and functional status in individuals with pregnancy induced posterior pelvic pain.
Materials and Methods
A single blinded randomised clinical trial was conducted at Department of Physiotherapy, KM Patel Institute of Physiotherapy, Shree Krishna Hospital, Karamsad, Gujarat, India. A total of 30 pregnant participants of 20 to 35 years with uncomplicated pregnancy and positive FABER’S (Patrick’s) test were selected and randomly assigned into two groups. SIJ mobilisation and TENS was given to Group A and Group B respectively thrice a week for five sessions. Both the groups received lumbo-pelvic stabilisation exercises, activity modification and ergonomic advises. Visual Analogue Scale (VAS) was used for pain assessment and Roland Morris disability score was used to find impact on functional status. Baseline assessment was noted for pain and functional disability. Data were collected immediately after first intervention and at the end of five sessions.
Results
Both the outcome measures in intragroup analysis showed improvements. Mean change in VAS score after five sessions for Group A was 6.91 and for Group B was 4.91. Functional improvement as assessed by RMDQ was 91% for Group A and 89% for Group B. Intergroup analysis proved that SIJ mobilisation was more effective in reducing pain and improving functional status (p<0.05).
Conclusion
SIJ mobilisation and TENS are effective in treating pregnancy induced posterior pelvic pain and reducing associated disability. SIJ mobilisation is more effective in terms of improvement.
Functional disability, Low back pain, Roland Morris disability score
Introduction
The prevalence of back pain in pregnancy is reported to be 75%, especially in the last trimester, 20% of these report posterior pelvic pain. The pain may radiate to the posterior thigh and can also occur in conjunction with/or separately in the symphysis [1]. This pain is often associated with the difficulty in standing, walking, and sitting, stair climbing etc., [2]. Women who suffer this pain often present with reduced capacity for functional activities [3].
The SIJ is a strong and stable weight bearing joint that permits very little movement due to its natural structure. Various validated biomechanical models of the pelvis supports that the SIJ is stabilised by active and passive structures surrounding the pelvis [4,5]. It has been shown that pelvic ligaments such as the iliolumbar, long dorsal and the sacrotuberous play important role in maintaining pelvic girdle stability [6]. Moreover, the gluteus maximus, erector spinae and thoracolumbar fascia are the active structures that attaches to these ligaments and contribute to the stability of the pelvic girdle.
Posterior pelvic pain may begin at any time during pregnancy; however, on an average it begins in the 18th week of pregnancy. Pelvic instability is possibly related to an increase in the hormone level relaxin which is thought to create laxity in pelvic ligaments as the pelvic girdle adapts to an anticipated pregnancy and is preparing for childbirth [7]. This instability allows for increased motion, stressing the SIJ. Increased lumbar hyperlordosis, anterior pelvic tilt and widening of the pubic symphysis are caused by hormonal changes and the enlarged uterus. The core muscles around the pelvis get ‘stretched’ and weakened due to growing uterus.
There is large heterogeneity in the proposed treatment of posterior pelvic pain. Management includes variety of specialties and is the interdisciplinary approach. The proposed treatment options ranges from bed rest, water gymnastics, lumbo-pelvic stabilisation exercises, pelvic belt, acupuncture [8], TENS, injections of corticosteroid into the intra-articular space and mobilisation (gentle form of manipulation) [9]. However, there is dearth of evidence to establish the efficacy of SIJ mobilisation and TENS in pregnancy induced posterior pelvic pain. TENS and SIJ mobilisation have evidence as safe measures to deal with posterior pelvic pain during pregnancy. Till date no randomised clinical trials are available to establish their efficacy and to be recommended as treatment option inposterior pelvic pain. So, present study was conducted in order to identify the effect of TENS and SIJ mobilisation in pregnancy induced posterior pelvic pain.
Materials and Methods
The present randomised clinical trial was carried out in a tertiary care hospital in Gujarat, India. Ethical clearance was obtained from Institutional Human Research and Ethical Committee. Participants were recruited from physiotherapy outpatient department after referral from obstetric department of the hospital. The data were collected over a period of 12 months from January 2013 to December 2013. Written informed consent was taken from each participant who participated in the study. Inclusion criteria were age group of 20-35 years, uncomplicated pregnancy and having pregnancy induced posterior pelvic pain unilateral or bilateral, pain score on VAS >50 mm and Positive FABER’S (Patrick’s) test [2]. Whereas, females with low back pain before pregnancy, lumbar pathology during pregnancy such as lumbar intervertebral disc pathology, radiculopathies, spondylolisthesis, trauma to the lumbo-pelvic region and participants who were part of other ongoing departmental research were excluded from the present study. A total of 32 pregnant female participants were recruited in the present study following eligibility criteria.
The participants were randomly divided into two groups: Group A and Group B via computerised randomisation method. Simple randomisation was employed using computer generated table of random numbers. One investigator managed the assignment scheme and provided the assignment to the treating physiotherapists in a series of consecutively numbered opaque envelopes. Allocation was concealed from the outcome assessor and participants at all times and from the physiotherapist until the point of treatment. Since, this was the single blind randomised design, assessor was unaware to which group the participant belonged. Primary assessment and outcome measures were taken by another qualified physiotherapist. VAS was used to assess pain. VAS is a commonly used tool for subjective assessment of pain. RMDQ is a reliable and valid tool to identify functional status of the patient with such pain [10]. Both the outcome measures were taken prior to first session and after completion of five sessions. Group A consisted of 16 participants to whom five sessions of SIJ mobilisation based on Maitland concept were delivered [11]. Group B consisted of 16 participants who received five sessions of TENS.
In order to deliver the comfortable position to the participant, side lying position was given with involved SIJ uppermost and pillow between the two knees. The abdomen was supported with pillow below it. Hot packs were applied to the involved part before the intervention to relax the tissues for 10 minutes. Subsequent intervention was given in the same position.
In Group A, Grade 1 and Grade 2 mobilisation were delivered as prescribed by Maitland [11]. Grade 1 mobilisation which are small amplitude rhythmic oscillations performed in the initial range of motion to reduce pain level. Grade 2 oscillations are large amplitude rhythmic oscillations performed in any range of motion but yet not reaching to the end range of motion to reduce pain. SIJ mobilisation consisted of graded postero anterior oscillations applied to the SIJ targeted at posterior superior iliac spine. Three sets of Grade 1 and 2, 30-second oscillations were applied to this segment at a rate of approximately 1 to 2 Hz.
Group B was given high frequency low intensity TENS for 30 minutes with frequency of 150 Hz and pulse width of 80-100 μs. The intensity was set according to the minimal sensory perception of the participant. Participants were placed in the same position as mentioned for mobilisation group. Single channel TENS was used and two electrodes placed over the painful area.
The interventions were given thrice a week for both the groups. Both the groups also received specific lumbo-pelvic stabilisation exercises [Table/Fig-1] that targeted activation of transversus abdominis and lumbar multifidus along with activity modifications and ergonomic advises.
Lumbo-pelvic stabilisation exercises.
| Strengthening of the Tranversus Abdominis (TrA) and Lubar Multifidus (LM) | Exercise for the TrA in four point kneeling Exercises for the TrA in dorsal decubitus with flexed knees Bridging for back extensors Co-contraction of the TrA and LM in upright position
|
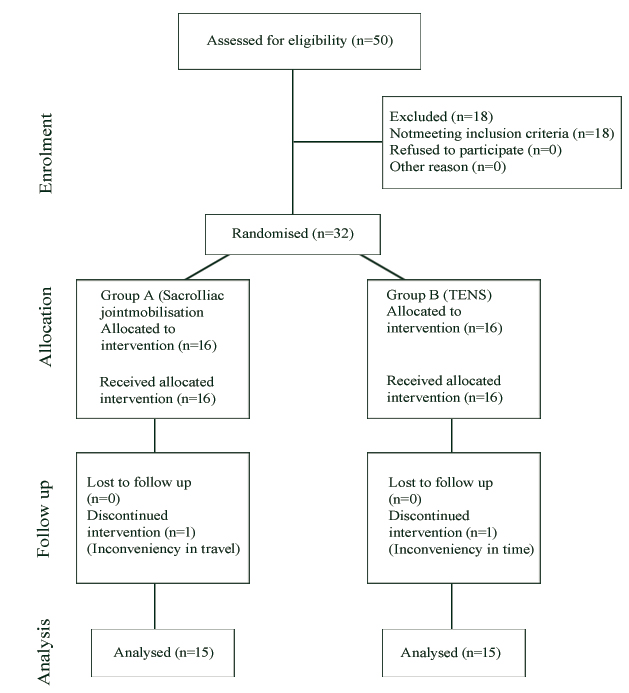
The exercises were done under supervision by the qualified physiotherapist. The exercises were done in two sets and each set constituted of eight repetitions. There were two drop outs, one each from both groups due to inconvenience caused by time and travel [Table/Fig-2].
Flow chart representing the entire procedure of the study.
Statistical Analysis
Statistical analysis was done using Statistical Package for the Social Sciences (SPSS) version 17.0. Normality of data was checked though Kolmogorov-Smirnov test. Baseline homogeneity for outcome measures was established by unpaired t-test. Paired t-test was used for intragroup analysis and unpaired t-test was used for intergroup analysis and p-value was set at less than 0.05. Statistical power was set at 0.80.
Results
Both the groups were homogeneous in terms of baseline values for outcome measures (pain and functional disability) with p-value greater than 0.05 (0.644, 0.707). Mean age of the participants in the Group A and Group B was 25.53 and 25.86 years respectively (p 0.227). Mean Body Mass Index (BMI) value of Group A and Group B was 24.56 and 24.23 kg/m2 respectively. (p=0.234) Incidence of sacroiliac pain was 3.4%, 20% and 76.6% in first, second and third trimester respectively. Incidence of pain was 36.6% in primigravida and 63.4% in multigravida [Table/Fig-3].
Demographic data and sacroiliac pain incidence.
| Mean age(years) | Mean BMI(kg/m2) | Sacroiliac pain incidence(%) |
|---|
| Group A | Group B | Group A | Group B | First trimester | Second trimester | Third trimester |
|---|
| 25.53 | 25.86 | 24.56 | 24.23 | 3.4 | 20 | 76.6 |
Intragroup analysis revealed significant improvement in terms of VAS and RMDQ score (p-value <0.0001) at the end of five sessions in Group A and Group B respectively [Table/Fig-4]. Only 60% of subjects reported complete relief of pain in Group A. Improvement was better in terms of pain and functional disability at the end of five sessions. Mean percentage improvement in RMDQ score was 96.98% for Group A and 83% for Group B. Intergroup analysis proved that SIJ mobilisation is superior in terms of all outcome measures as compared to TENS, at the end of five sessions (p<0.0001) as shown in [Table/Fig-5].
Paired t-test to measure change in VAS and RMDQ from baseline within group.
| Group | Mean (SD) VAS score | p-value | Mean (SD) RMDQ | p-value |
|---|
| Group A | Pre | 7.51 (1.25) | <0.001 | 15.46 (3.50) | <0.001 |
| Post | 0.60 (0.73) | 0.46 (0.63) |
| Group B | Pre | 7.34 (0.70) | <0.001 | 15.06 (2.08) | <0.001 |
| Post | 2.43 (0.96) | 2.53 (1.30) |
Comparison between groups in terms of VAS and RMDQ using unpaired t-test.
| Mean (SD) | Group A | Group B | p-value |
|---|
| Change in VAS score at the end of 5 sessions | 6.91 (1.28) | 4.90 (1.08) | <0.001 |
| Change in RMDQ score at the end of 5 sessions | 15.00 (3.42) | 12.53 (1.84) | 0.02 |
Discussion
Pregnancy induced low back pain and posterior pelvic pain is a commonly found condition. Identification and treatment of the pain is very much essential as untreated condition carries risk of development of pain after pregnancy also [12]. In the present study, we compared the effects of two physical therapy treatment approaches to treat the posterior pelvic pain. SIJ mobilisation and TENS are commonly used interventions for pregnancy induced posterior pelvic pain. The results of the present study proved that both the interventions are effective in reducing pain and improving functional outcome. The pain reduction and improvement in functional status achieved by both the groups is statistically significant. Intergroup analysis proved VAS score was significantly lower in the Group A which received Maitland mobilisation. The significant difference was also observed in the RMDQ score between two groups.
Low back pain in pregnancy is likely to be due to SIJ dysfunction which can be significantly improved with mobilisation [12]. In a systematic review, which analysed the interventions for treating pregnancy related pelvic and back pain revealed moderate quality evidence for multimodal intervention including mobilisation, exercise and education [13]. In a study of 170 pregnant females with painful low back, the females who received manipulation reported less pain during labour [14]. In a study involving 23 women having sacroiliac subluxation, 11 women received rotational manipulation in pregnancy and 91% of participants reported complete relief of pain [14]. These trials supported the findings of the present study with 60% of subjects reporting complete relief of pain with mobilisation. However, in present study, mobilisation produced results in short period of time which was less than two weeks unlike findings reported by previous trials [13-15].
In a randomised control trial, involving 169 pregnant women having low back pain or pelvic pain, one group received manual therapy, stabilisation exercises and standard obstetric care and another group received only obstetric care. The group that received standard obstetric care did not have any significant improvement [15].
Both mechanical and neurophysiologic mechanisms have been described to explain pain reduction and improved mobility following mobilisation, and it is conceivable that both mechanisms played a role in the findings of the present study. Joint mobilisation techniques are thought to be beneficial as they stimulate the mechanoreceptors. Passive motion has been reported to selectively stretch contracted tissues without damaging healthy adjacent tissues and correct the biomechanical and soft tissue dysfunction. Dorsal horn activation from a painful stimulus has been shown to decrease following joint mobilisation and breaks pain spasm cycle. This finding could explain the observations of several authors who have reported that passive movements applied elevated pain thresholds to various mechanical stimuli [16,17]. In addition, a study of the Hoffman reflex demonstrated a transient attenuation of alpha motor neuron excitability following mobilisation [18].
VAS score also decreased in Group B receiving TENS with no complications reported during its use. Studies typically refer to the gate control theory of pain to explain the effects of high frequency TENS. Specifically, it is suggested that stimulating large diameter afferent fibers inhibit input from small diameter afferent fibers in the substantia gelatinosa of the spinal cord [19]. This is thought to be a segmental inhibition along with increased beta endorphins in circulation. TENS is a safe and effective modality to reduce pain in the pregnancy induced posterior pelvic joint pain [20].
Study comparing effect of exercises, TENS and acetaminophen with the control group having back pain in the pregnancy concluded that TENS is a safe and effective way to reduce pain in the pregnancy [21]. In an update on pregnancy related pelvic pain, Kankaris NK et al., reported inconsistent findings on effect of TENS on pain. However, no negative effects were found with the use of TENS in any stage of pregnancy which supports the finding of our study [9]. No negative effects were reported for any of the patients.
Limitation
In the present study, there was lack of follow up for recurrence of pain in rest of the pregnancy and in post partum period. So another study with multicenter trial can be done with follow up to see the sustained effects of the intervention and the rate of recurrence.
Conclusion
Hence, it can be concluded that both mobilisation and TENS can be used as an intervention in pregnancy induced SIJ pain for reduction of pain and functional disability. Mobilisation can prove to be an effective non pharmacological superior intervention for pregnancy induced posterior pelvic pain. However, further high quality evidence needed to establish its efficacy.
[1]. Sturesson B, Udén G, Udén A, Pain pattern in pregnancy and “catching” of the leg in pregnant women with posterior pelvic painSpine 1997 22(16):1880-84.10.1097/00007632-199708150-000139280024 [Google Scholar] [CrossRef] [PubMed]
[2]. Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B, European guidelines for the diagnosis and treatment of pelvic girdle painEur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc 2008 17(6):794-819.10.1007/s00586-008-0602-418259783 [Google Scholar] [CrossRef] [PubMed]
[3]. Röst CCM, Jacqueline J, Kaiser A, Verhagen AP, Koes BW, Pelvic pain during pregnancy: a descriptive study of signs and symptoms of 870 patients in primary careSpine 2004 29(22):2567-72.10.1097/01.brs.0000145416.22782.9f15543075 [Google Scholar] [CrossRef] [PubMed]
[4]. Snijders CJ, Vleeming A, Stoeckart R, Transfer of lumbosacral load to iliac bones and legs Part 1: Biomechanics of self-bracing of the sacroiliac joints and its significance for treatment and exerciseClin Biomech Bristol Avon 1993 8(6):285-94.10.1016/0268-0033(93)90002-Y [Google Scholar] [CrossRef]
[5]. Snijders CJ, Vleeming A, Stoeckart R, Transfer of lumbosacral load to iliac bones and legs Part 2: Loading of the sacroiliac joints when lifting in a stooped postureClin Biomech Bristol Avon 1993 8(6):295-301.10.1016/0268-0033(93)90003-Z [Google Scholar] [CrossRef]
[6]. Pool-Goudzwaard A, Hoek van Dijke G, Mulder P, Spoor C, Snijders C, Stoeckart R, The iliolumbar ligament: its influence on stability of the sacroiliac jointClin Biomech Bristol Avon 2003 18(2):99-105.10.1016/S0268-0033(02)00179-1 [Google Scholar] [CrossRef]
[7]. Mitchell DA, Esler DM, Pelvic instability-painful pelvic girdle in pregnancyAust Fam Physician 2009 38(6):409-10. [Google Scholar]
[8]. Kvorning N, Holmberg C, Grennert L, Aberg A, Akeson J, Acupuncture relieves pelvic and low-back pain in late pregnancyActa Obstet Gynecol Scand 2004 83(3):246-50.10.1111/j.0001-6349.2004.0215.x14995919 [Google Scholar] [CrossRef] [PubMed]
[9]. Kanakaris NK, Roberts CS, Giannoudis PV, Pregnancy-related pelvic girdle pain: an updateBMC Med 2011 9:1510.1186/1741-7015-9-15:21324134 [Google Scholar] [CrossRef] [PubMed]
[10]. Roland M, Fairbank J, The roland-morris disability questionnaire and the oswestry disability questionnaireSpine 2000 25(24):3115-24.10.1097/00007632-200012150-0000611124727 [Google Scholar] [CrossRef] [PubMed]
[11]. Maitland GD, Hengeveld E, Banks K, English K, Maitland’s Vertebral Manipulation 2005 Edinburgh; New YorkElsevier Butterworth-Heinemann [Google Scholar]
[12]. McIntyre IN, Broadhurst NA, Effective treatment of low back pain in pregnancyAust Fam Physician 1996 25(9 Suppl 2):S65-S67. [Google Scholar]
[13]. Pennick VE, Young G, Interventions for preventing and treating pelvic and back pain in pregnancyCochrane Database Syst Rev 2007 (2):CD00113910.1002/14651858.CD001139.pub2 [Google Scholar] [CrossRef]
[14]. Diakow PR, Gadsby TA, Gadsby JB, Gleddie JG, Leprich DJ, Scales AM, Back pain during pregnancy and laborJ Manipulative Physiol Ther 1991 14(2):116-18. [Google Scholar]
[15]. George JW, Skaggs CD, Thompson PA, Nelson DM, Gavard JA, Gross GA, A randomized controlled trial comparing a multimodal intervention and standard obstetrics care for low back and pelvic pain in pregnancyAm J Obstet Gynaecol 2013 208(4):295.e1-e7.10.1016/j.ajog.2012.10.86923123166 [Google Scholar] [CrossRef] [PubMed]
[16]. Colloca CJ, Keller TS, Electromyographic reflex responses to mechanical force, manually assisted spinal manipulative therapySpine 2001 26(10):1117-24.10.1097/00007632-200105150-0000511413422 [Google Scholar] [CrossRef] [PubMed]
[17]. Hanrahan S, Van Lunen BL, Tamburello M, Walker ML, The short-term effects of joint mobilizations on acute mechanical low back dysfunction in collegiate athletesJ Athl Train 2005 40(2):88-93. [Google Scholar]
[18]. Dishman JD, Bulbulian R, Spinal reflex attenuation associated with spinal manipulationSpine 2000 25(19):2519-24.10.1097/00007632-200010010-0001511013505 [Google Scholar] [CrossRef] [PubMed]
[19]. Melzack R, Wall PD, Acupuncture and transcutaneous electrical nerve stimulationPostgrad Med J 1984 60(710):893-96.10.1136/pgmj.60.710.8936334851 [Google Scholar] [CrossRef] [PubMed]
[20]. Coldron Y, Cook T, Notcutt W, Watson T, Safe use of transcutaneous electrical nerve stimulation for musculoskeletal pain during pregnancyAvailable from www.csp.org.uk/sites/files/csp/secure/crothers.pdf. [Access Date 6th November 2016] [Google Scholar]
[21]. Keskin EA, Onur O, Keskin HL, Gumus II, Kafali H, Turhan N, Transcutaneous electrical nerve stimulation improves low back pain during pregnancyGynaecol Obstet Invest 2012 74(1):76-83.10.1159/00033772022722614 [Google Scholar] [CrossRef] [PubMed]