Osteoarthritis is an almost inevitable consequence of aging and is characterized by degenerative changes in the articular cartilage of diarthrodial joints and subsequent new bone formation at the articular margins [1]. Knee is the most commonly affected joint [2]. High Tibial Osteotomy (HTO) is the most common treatment of isolated osteoarthritis of medial tibiofemoral compartment of knee. It may be performed using a closing-wedge technique, by dome osteotomy, by medial opening hemicallotasis or by an opening-wedge technique [3]. The goal of the treatment is to relieve medial compartment knee pain and slow down the arthritic progression. This is achieved by partial unloading of the medial compartment with a 6-10 degree overcorrection of the mechanical axis [4].
In barrel vault osteotomy, dome shaped, smooth, concentric osteotomy of tibia just proximal to tibial tuberosity is made with a special jig. Distal fragment is overcorrected to achieve 100 valgus, and then cylindrical cast is applied. Patient is mobilised after two days with partial weight bearing. There are definite advantages of this technique over other methods of osteotomy [5]. But there are also disadvantages over other wedge osteotomies [6].
Although knee replacement has been shown to be effective in young patients the main concern is the potential adverse effect of high joint forces on the polyethylene articular surface and wear debris generated over many years, carries the risk of causing aseptic loosening. Total knee replacement has generally been reserved for older patient because numerous revisions of operations may be required in the course of lifetime [7].
Brouwer RW et al., concluded in their meta-analysis that there is silver-level evidence that no significant difference in pain, function and gait analysis was observed after HTO compared to Unicompartmental Knee Arthroplasty (UKA) [8]. HTO is an old procedure which was developed for medial compartment osteoarthritis of knee; the same thing is being stressed upon with use of different scores as HTO is still a joint preserving surgery which restores joint kinematics. Hence, the present study was conducted to evaluate the functional outcome of barrel vault tibial osteotomy in the management of osteoarthritis of the knee.
Materials and Methods
The present prospective study was conducted in Poona Hospital and Research Centre, between May 2012 and May 2015. Fifty five patients in the age group 45 to 60 years with suspicion of medial compartmental osteoarthritis knee were included in the study. Based on previously published study [5], setting an alpha error at 0.05, and power at 80%, sample size of 50 patients was calculated by formula [9] for this prospective study.
Patients with Medial compartmental osteoarthritis associated with patellofemoral osteoarthritis and also who had range of motion ≥ 90 degrees were included in the study.
Exclusion criteria involved Tri compartmental OA knee, medial and lateral compartment OA, patient with restricted range of motion/fixed deformities (knee flexion < 90 degrees, > 20 degrees of valgus correction needed, flexion contracture of > 15 degrees), patients with ligamentous instability, Lateral tibial subluxation of more than 1 cm, medial compartment tibial bone loss of more than 2 or 3 mm.
Ethical clearance was obtained from Institutional Ethics Committee and Scientific Advisory Committee of the institution. Informed written consent of the patients was obtained after explaining the details of the surgical procedure and risks involved.
Preoperative Assessment included detailed history, Knee society score and Visual Analogue Scale (VAS) score. Clinical examination included medial joint line tenderness, range of movement at knee, measurement of angular deformity, anterior drawer test, posterior drawer test, McMurray’s test, Varus/Valgus stress test, limb length discrepancies and foot/ankle deformity assessment. Radiographic findings were noted by weight bearing X-Rays of both Knees (anteroposterior and lateral views), Varus Valgus stress views, Scanogram of both lower limbs. Hip-Knee-Ankle (HKA) angle (mechanical axis) was measured on standing films preoperatively to determine the degree of correction required.
The patient was positioned supine on a radiolucent operating table. A thigh tourniquet was applied and the leg draped free. Preliminary diagnostic arthroscopy of the knee was performed to exclude lateral compartmental osteoarthritis knee. Five patients with lateral compartment arthritis were excluded from the study. Two separate longitudinal incisions were made for the fibular and tibial osteotomies. A short incision starting from 0.5 cm below the head of the fibula and extending over the postero-lateral border of the fibula was made. The fascia was divided in the same line and the fibular shaft was exposed by blunt dissection through the plane between the peroneus longus and gastrocnemius muscles. This exposure did not bring the peroneal nerve into view but avoided damage to it. Bone levers were inserted and one centimeter long fragment of fibula was resected at a level just below the tibial osteotomy.
A second longitudinal incision five centimeter long centred on the tibial tuberosity was made. The patellar tendon was exposed and defined. Muscles were stripped down medially giving a clear exposure of the upper end of the tibia. The jig [Table/Fig-1] custom made by the orthopaedic surgeon was then inserted, one blade under and one blade over the patellar tendon. After the most satisfactory position for the dome was chosen, the jig was pulled down firmly against the patellar insertion. A single drill was positioned at a right angle to the axis of the tibia and left in situ. A hand drill was used as it was easier to control the depth. Another similar drill was used on the other side. These drills maintained the guide in the desired place. Then the remaining holes were drilled to complete the arc of the holes, penetrating both the cortices. The knee was flexed about 50o-60o by an assistant while the holes were drilled to protect the neurovascular bundle. The drill holes were then easily joined using a 6-8 mm osteotome which easily followed the holes. The final result was a single plane dome osteotomy [Table/Fig-2]. This could be easily displaced to suit the amount of correction required.
Barrel vault osteotomy jig.

Single plane arc osteotomy.

The skin was closed after using one suction drain. An adequate dressing was applied and all patients were given a cylinder cast in a position of valgus with an average of 100 with the help of metal goniometer.
HKA Angle and Knee Society Score were used to measure the outcome. VAS score was taken immediate postoperatively, on 2nd day, at two weeks, four weeks, six weeks, two months, four months and six months for pain measurement.
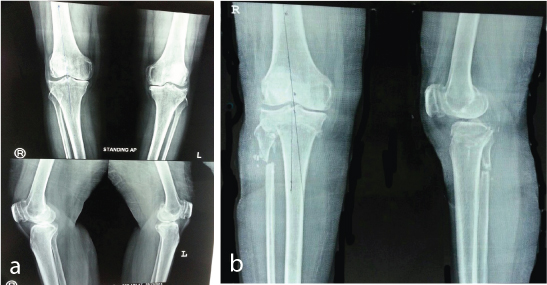
X-Rays were taken postoperatively. After initial subsidence of immediate postoperative pain, patients were allowed to sit up in bed and were encouraged to do static quadriceps and ankle pump exercises. They were allowed to stand on their feet after two days with elbow crutches, allowing them partial weight bearing on the operated leg. The plaster was changed after two days to get the desired alignment. During final correction the distal part of the osteotomy was shifted 5 mm anteriorly (maquet procedure) under fluoroscopic guidance under anaesthesia [Table/Fig-3]. This was done easily maintaining the contact between the two fragments. Full weight bearing was started third day postoperatively. Patients were discharged after 8 to 10 days and were seen after two weeks for change of plaster and removal of stitches. The position of the osteotomy was re-examined by X-Ray. The patients were instructed to continue walking with a gradual increase in weight bearing on the operated leg. After six weeks the plaster was removed and the stability of the osteotomy was checked clinically and radiologically. [Table/Fig-4a,b] depicts the X-Rays taken preoperatively and at six months postoperatively. Later on, the knee was mobilised in the Physiotherapy Department, but with the knee protected in a back splint till the quadriceps showed satisfactory strength.
Correction confirmed under C- arm.

a) X -Ray of the patient before barrel vault tibial osteotomy showing decreased joint space and varus at proximal tibia; b) X-Ray of the patient taken at six months after barrel vault tibial osteotomy that showed correction of the varus deformity at proximal tibia.
All the patients were reviewed at two weekly intervals for a period of two months and then every two months for further six months. At every visit patients were evaluated by clinical examinations, Knee society score and HKA angle radiologically. Grading of Knee society score was done as follows: Excellent - 80-100, Good - 70-79, Fair - 60-69, and Poor - <60 [10].
Data on categorical variables is presented as percentage of cases. Data on continuous variables is presented as Mean±SD. Statistical significance of difference of categorical variables was tested using Fisher’s-exact test. Continuous variables were tested by paired t-test, and ANOVA test. A p-values < 0.05 were considered to be statistically significant. Entire data was analysed using Statistical Package for Social Sciences (SPSS) version 20.0, Inc. Chicago for MS Windows.
Results
The present study was conducted on 50 patients of medial compartmental osteoarthritis of the knee. All cases were operated for barrel vault tibial osteotomy. Patient was followed up for six months. In the present study, 14/50 (28%) patients were between 45 and 50 years, 15/50(30%) were between 51 and 55 years and 21/50(42%) were between 56 and 60 years. Out of 50 patient, 17 (34%) patients were males whereas 33 (66%) were females.
It can be seen from [Table/Fig-5] that there was statistically significant difference between mean HKA angles, mean knee score, mean functional score at preoperative and postoperative measurements. There was significant improvement in mean HKA angle, mean knee score, mean functional score postoperatively at six month follow up. There was mean decrease of 0.80 of knee range of motion between preoperative and postoperative measurement, but it was not significant.
| Characteristic | Preoperative(N = 50) | Postoperative(six months)(N = 50) | p-value |
|---|
| Mean hip knee ankle angle (SD) | 189.50 (± 4.00) | 173.08(± 2.06) | < 0.001 |
| Mean knee score (SD) | 48.10 (± 12.74) | 86.14 (± 11.44 | < 0.001 |
| Mean functional score (SD) | 58.60(± 11.25) | 93.40(± 11.90) | < 0.001 |
| Mean range of motion | 120.00(± 11.61) | 119.70(± 14.12) | > 0.05 |
Paired t- test was used
In the present study, 40 patients (80%) had excellent functional outcome, 7 patients (14%) had good functional outcome, one patient (2%) had fair functional outcome, and two patients (4%) had poor functional outcome.
As depicted in [Table/Fig-6], there was statistically significant difference between mean HKA angle, mean functional score and mean range of motion with respect to functional outcome.
| Characteristic | Functional Outcome (at Six months) | p-value |
|---|
| Excellent(N=40) | Good(N= 7) | Fair(N = 1) | Poor(N= 2) |
|---|
| Mean hip knee ankle angle (SD) | 172.65(± 1.48) | 173.43(±1.72) | 174.00 | 180.00 | < 0.001 |
| Mean functional score (SD) | 97.88(± 5.17) | 83.14(±8.80) | 68.00 | 52.50(±3.54) | < 0.001 |
| Mean range of motion | 124.50(±7.14) | 107.86(±10.35) | 110.00 | 70.00(±14.14) | < 0.001 |
ANOVA test was used
As shown in [Table/Fig-7], there was statistically significant difference between VAS score and functional outcome at six months. Functional outcome was excellent when VAS score was zero.
Association between VAS Score and functional outcome at six month.
| Variables | VAS Score at six months | Total | p-value |
|---|
| 0 | 2 | 4 | 6 |
|---|
| Functional Outcome | Excellent | 25 | 14 | 0 | 1 | 40 | <0.001 |
| Good | 0 | 3 | 3 | 1 | 7 |
| Fair | 0 | 0 | 0 | 1 | 1 |
| Poor | 0 | 0 | 0 | 2 | 2 |
| Total | 25 | 17 | 3 | 5 | 50 | |
Fisher’s-exact test was used
Complications: There were no cases of intraoperative complications. Four percentage of patients had delayed union where as 6 % suffered from superficial infection.
In our study eight patients had retropatellar pain preoperatively. After the osteotomy the symptoms totally disappeared in seven patients. In one patient mild pain was observed.
Discussion
In the present study we evaluated the functional outcome of barrel vault osteotomy of proximal tibia for medial compartment osteoarthritis of the knee in 50 patients.
In the present research, mean age of the patients was 54.26 which is comparable to studies undertaken by Kodkani et al., and Bachhal et al., whereas Takeuchi R et al., and Takahashi T et al., reported mean age 69.00 years and 66 years respectively [5,11-13]. In the present research, 33/50 (66%) patients were females. Kodkani PS and Takahashi T et al., reported 16/19(84.2%) and 34/42(81%) female population respectively in their studies [5,13].
The following [Table/Fig-8] shows mean HKA angle preoperatively and postoperatively of various studies at six months follow up. As shown in [Table/Fig-8]. our findings were comparable with other studies [5,7,11-13]. The following [Table/Fig-9] shows our results were comparable to other studies [5,7,14].
Comparison of mean HKA angle preoperatively and postoperatively of various studies.
| Study | Preoperative meanHKA | Postoperative mean HKA |
|---|
| Kodkani PS [5] | 191.1o | 173.1o |
| Bachhal V et al., [11] | 190.6 | 176.0 |
| Takeuchi R et al., [12] | 181.3 | 169.6 |
| Zaki SH and Paul PJ [7] | 187 | 174 |
| Takahashi T et al., [13] | 184 | 168 |
| Present study | 189.50 | 173.08 |
Comparison of mean knee score preoperatively and postoperatively of various studies.
| Study | Preoperative mean knee score | Postoperative mean knee score |
|---|
| Kodkani PS [5]. (2007) | 49.58 | 88.89 |
| Zaki SH and Paul PJ [7]. (2009) | 38 | 82 |
| Aydoğdu S and Sur H [14]. (1997) | 54 | 83 |
| Present study | 48.10 | 86.14 |
The following [Table/Fig-10] shows our results were comparable to other studies [5,7,12,14].
Comparison of mean functional score preoperatively and postoperatively of various studies.
| Study | Preoperative | Postoperative |
|---|
| Kodkani PS [5] | 60.53 | 96.32 |
| Zaki SH and Paul PJ [7] | 35 | 75 |
| Takeuchi R et al., [12] | 59.3 | 94.1 |
| Aydoğdu S and Sur H [14] | 55 | 81 |
| Present study | 58.60 | 93.40 |
In the present research, there was no improvement in mean range of motion postoperatively. There was mean decrease of 0.8o of knee range of motion. High tibial osteotomy is an operation which when done without any intraarticular procedure has little effect on the preoperative range of motion. Saeed H Zaki and Paul J. Rae [7] reported no change in range of motion postoperatively, Chiang H et al., reported decrease in range of motion by 100 postoperatively [15] whereas, Bachhal V et al., reported increase in range of motion by 0.30 postoperatively [11].
In the present research, functional outcome was excellent in 40/50 (80%), good in 7/50 (14%), fair in 1/50 (2%) and poor in 2/50 (4%) of patients postoperatively. Kodkani PS reported excellent and good outcome in 15/19 (79%) and 4/19 (21%) patients respectively [5] whereas Maquet P reported excellent and good outcome in 32/41(78%) and 5/41 (12.2%) patients respectively [16]. In a study conducted by Bachhal V et al., 57% patients had excellent functional outcome [11].
In our study retro patellar pain was associated with degenerative changes in patellofemoral joint. Out of eight patients having retropatellar pain, symptoms totally disappeared in seven patients after osteotomy whereas one patient had mild pain. We believe the relief of retropatellar pain was due to the Maquet effect. Maquet effect is anteriorization of tibia distal to the high tibial osteotomy (possessing attachment of ligamentum patellae to tibial tuberosity) to relieve patellofemoral symptoms of osteo-arthritis of knee [17].
Superficial wound infection was seen in three patients (6%), which were treated successfully with appropriate antibiotics. The end results of the operation were not affected by the occurrence of infection. There was no deep infection. Bachhal V et al., reported infection in 23/37 (62.2%) of patients [11] whereas Zaki SH et al., in 3/ 46 (6.5 %) of patients [7].
In our research two patients had delayed union. They united after prolonged immobilisation in plaster for 16 weeks. But both the patients lost more than 50o of preoperative flexion. Bachhal V et al., [11] reported 2/ 37 (5.4 %) delayed union in their research.
Limitation
Follow up period after barrel vault HTO was only six months.
Conclusion
There was significant improvement in mean Hip-Knee-Ankle angle, mean knee score, mean functional score postoperatively at six month follow up. There was significant difference between mean HKA angle, mean functional score and mean range of motion with respect to functional outcome. Barrel vault tibial osteotomy is useful in the management of medial compartmental osteoarthritis of the knee in patients between 45 and 60 years of age.
Paired t- test was used
ANOVA test was used
Fisher’s-exact test was used