The identification of rationale behind programme development and factors affecting it, play significant role in CD/revision. It cannot be assumed that curriculum will remain static over time; hence, consideration must be given to ensure that reforms are accounted for at every step of the development process.
Various studies have been conducted and literature is available regarding the problems encountered during CD in higher education. But a comprehensive study on factors influencing CD and revision in health profession education scarcely exists. Many of them have focused on specific component in CD rather than whole process [4-7].
This study intended to investigate the perspectives and experiences of educators on challenges and issues involved in CD/revision of health profession courses. This possibly would assist them in anticipating hurdles at each step of CD, so as to be prepared with effective alternate strategies and rectify accordingly. This would ensure effective curricular revision and support in achieving University mission.
Materials and Methods
The exploratory study was designed to obtain the factors influencing the CD or revision. Institutional Ethical Committee approval was obtained prior to study.
The mixed method approach was employed with combination of both qualitative and quantitative methods [8]. The study was conducted by Department of Medical Education at JSS University, Karnataka, India, from May 2016 to September 2016. Data was gathered by in depth interviews, written questionnaire and focus group discussions. This was done to ensure triangulation of data and corroborate the findings within the study.
The survey questionnaire was designed with 18 items of both open and close ended types. The face validity was established through authorities’ in medical education. They evaluate if questions effectively captured the intent of study. The reliability was tested by giving questionnaire to three raters and was asked to fill it. There was strong positive correlation across raters. Pilot testing was done on three institutional curriculum committee members. The questionnaire was prepared considering various factors influencing each stage of Kern’s six-step approach to CD process [9]. The faculty involved in CD and revision of various courses started at our University, were identified. A total of eight faculties out of fifteen across various disciplines were shortlisted based on their absolute involvement and experience in CD process. Informed consent was obtained prior to the study. They were briefed about the intent of study and questionnaire was administered.
Based on their expected ability to provide valuable opinions judged by their experience and level of contribution to CD, three among eight faculties were selected for semi structured interviews and focus group discussion. Semi-structured interview was administered individually on the three recruited experts by moderator and was recorded. Focus group consisted of same panel of experts, moderator and a record keeper. The moderator briefed the group on the purpose and outline of discussion that lasted for 50 minutes. Both semi-structured interview and focus group discussion were carried out by same moderator to keep up continuity. Both were audio taped verbatim during the process by the concerned interviewer. The tapes were duplicated to be individually coded by two evaluators. The codes were transcribed and analysed. The evaluators derived the themes emerging from the codes. Point of saturation was ensured if same themes are emerging from the interview.
Statistical Analysis
The questionnaire data was analysed using descriptive statistics.
Results
A number of seven (87.5%) faculties expressed that the courses were running successfully, six (75%) faculties developed curriculum as team and rest worked individually and communicated to team members later. About four (50%) expressed that all stake holders were involved in CD process whereas three (37.3%) stated partial involvement, with students not being the part of the team. Only in seven (87.5%) courses - needs assessment was done. Majority of them were through expert panel group discussions. Only six (75%) faculties involved in CD had prior experience in it whereas remaining faculties were doing it for the first time. Only one among the eight faculties had previous exposure to formal training. They opined that prior training was mandate for CD as it would reduce flaws in the process, make the process easy, assist in systematic planning, and thus contribute significantly towards success of the course.
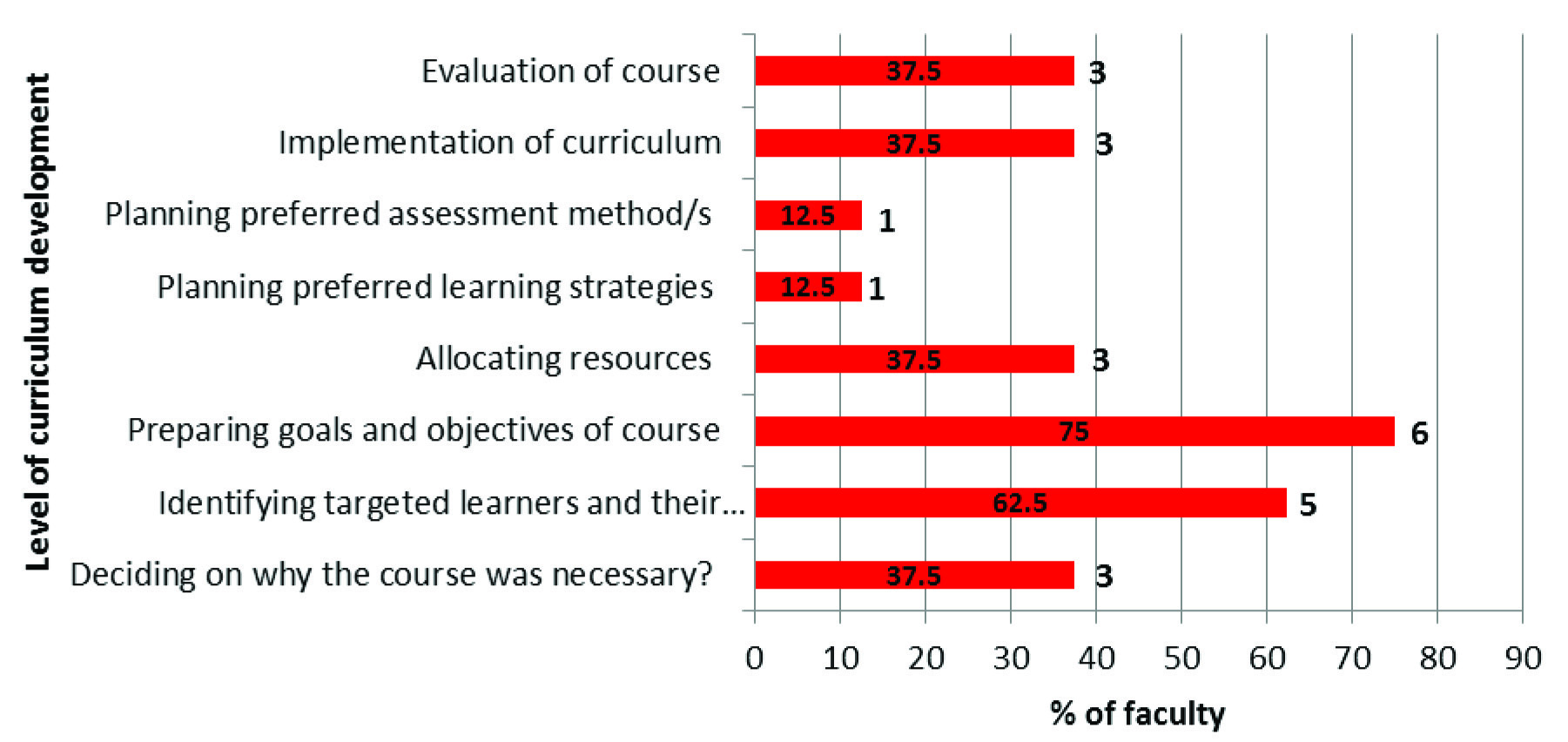
The faculty perception on extent of challenge gone through during the CD process is depicted in [Table/Fig-1].
Faculty (n=8) perception on difficulty level of steps involved in curriculum development.
Notes: Number next to bar indicate the number of faculty for each response.
Time allotted was sufficient and planning was fair. Only six faculties (75%) stated that CD process did not turn out to be an organised approach. And four (50%) expressed that allocation of finance and resources were adequate and four (50%) as just sufficient.
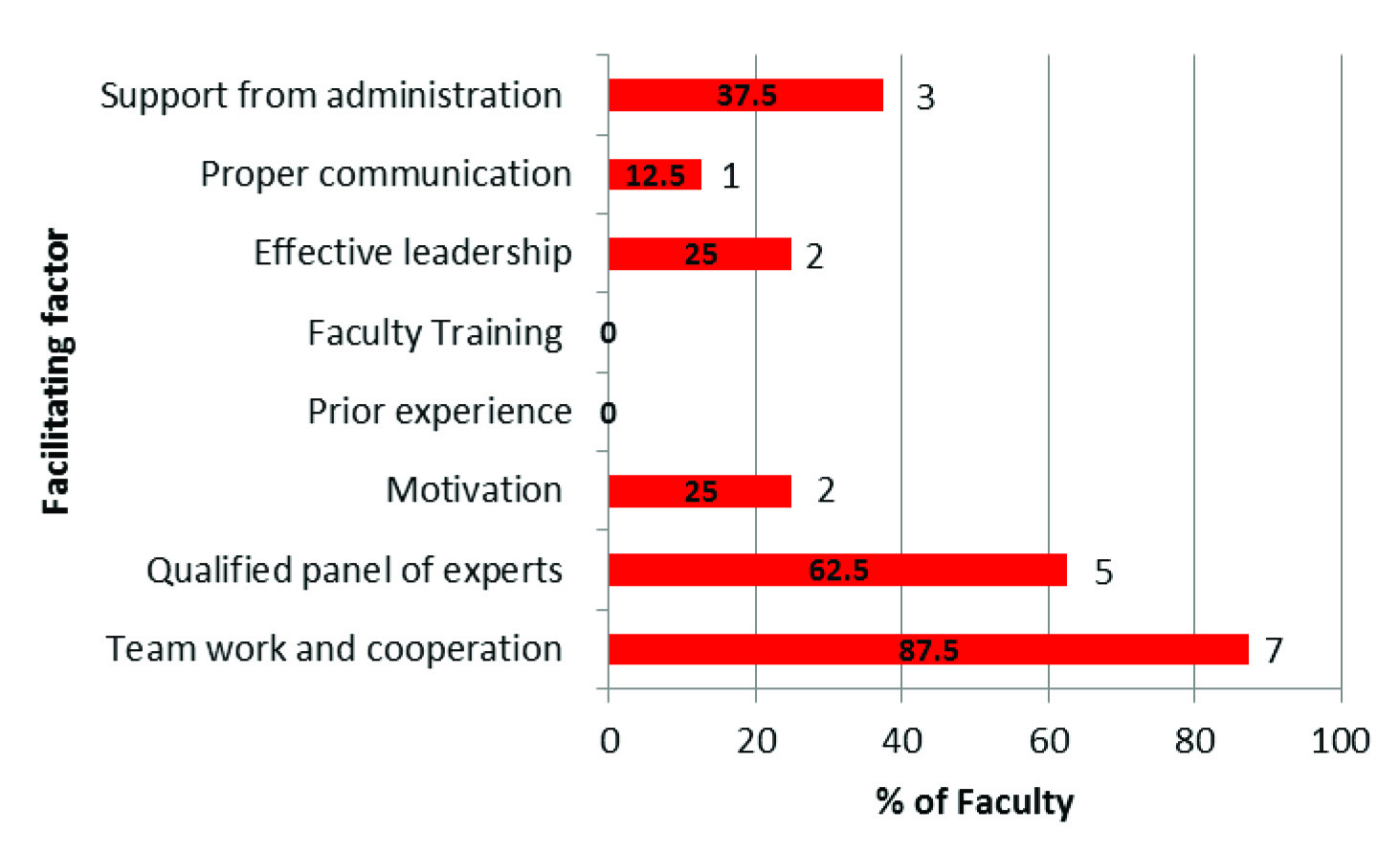
The factors facilitating and hindering CD are given in the [Table/Fig-2,3].
Faculty (n=8) viewpoint on facilitating factors that contributed towards curriculum development.
Notes: Number next to bar indicate the number of faculty for each response.
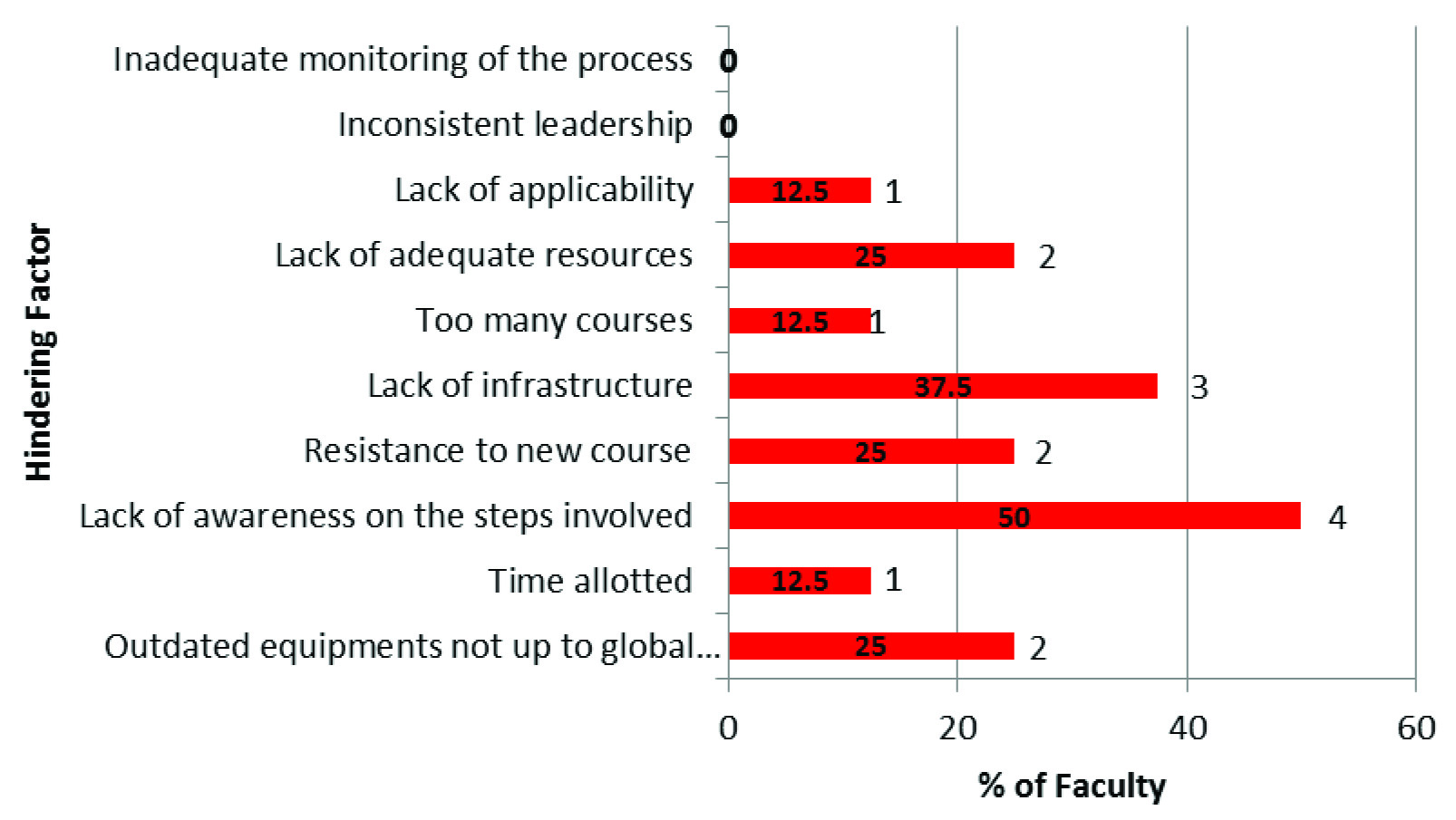
Faculty (n=8) viewpoint on hindering factors that affected curriculum development.
Notes: Number next to bar indicate the number of faculty for each response
Infrastructure refers to physical facilities – classrooms, IT enabled facilities
Adequate resources refer to manpower, experts, information regarding new program.
A number of seven faculties (87.5%) expressed their concern that addition of new courses affected their basic course they ought to teach. Global requirements were taken into account in four (50%) courses but were not definitely in the rest. The courses were adequately monitored in six (75%) of courses. And four (50%) were highly satisfied with their CD process, three (37.5%) were just satisfied, whereas remaining were unsatisfied with the CD process altogether. Only six (75%) of those involved in CD evaluated the effectiveness of the programme but it was not through structured format.
The responses arising from interview and focus group discussions were collated and categorised into individual and institutional issues [Table/Fig-4,5]. Those not fitting into above were separately documented as general issues.
Individual issues affecting curriculum development/revision.
| Facilitating factors | Hindering factors |
|---|
| CommitmentSelf-motivationCoordination within team | Forcefully imposed to work for the courseLack of awareness of steps involved Lack of prior experienceResistance from stakeholders |
Institutional issues affecting curriculum development/revision.
| Facilitating factors | Hindering factors |
|---|
| Expert panelTeam workAdministrative supportInfrastructureAdequate resourcesCourse monitoring | Lack of trainingPartialEffective and timely communicationToo many courses – work overload |
The general issues influencing CD emerged during interview and focus group discussions were: consideration on global applicability of the course, placements, disparity between changing trends with advancement, structured formal evaluation of effectiveness of the programme.
Discussion
CD is a dynamic process, driven by changing healthcare needs, advancements in subject knowledge and educational technologies. As we are moving towards outcome based education system, robust methods to update, monitor and evaluate the curriculum are fundamental requirements. Whatever may be the circumstance, knowledge of factors affecting the curricular aspects whether institutional, individual or general are crucial to ensure productive outcome.
Studies of successful reforms have stressed that such modifications should focus on every aspect of CD process: education to evaluation, teacher training, content structure, educational context, organizational structure and institutional culture [8]. Consensus among team members builds a supportive atmosphere wherein they are prepared to commit and engage in activities conducive to successful outcome [10]. Teamwork rather than individual efforts would assist to predict the possible obstacles and build constructive strategies to overcome challenges. Brown JD asserted the fact that when everyone works together on curriculum, this responsibility will be no more extra pile of work and will get imbibed as a part of occupation [5]. Synergy and collaboration among team members in an institution ensures better outcome rather than compartmentalised approach [11]. Teamwork was one of the institutional facilitating factors that impacted CD and revision in this study. Absolute involvement of faculty was not feasible due to hospital obligations.
According to Chung Lam C, the difficulties encountered during curricular reforms include lack of involvement, lack of communication among stakeholders regarding policy design, formulation, and implementation [12]. The deterring factor noted in the present study was lack of participation of students and external experts, which might have impacted the final outcome. This finding is supported by the survey of Wood JN on importance of stakeholders showed that 72%-75% of educators do not engage stakeholders especially, students and community members. This was observed specifically in evaluation review of CD and approval of written curriculum with resources [6]. Also, the resistance was encountered for starting new course due to their prior involvement in other programme.
The first step in planning any professional development activity is to assess the learning needs of the target group or individual to determine the structure of the program in terms of objectives, content, and activities [10]. It evaluates the requirements of a curriculum, possible content and instructional strategies to provide appropriate, realistic information on implementation depending on availability of resources at the institution. If needs assessment is not done, a magnificent curriculum could be developed, but the requirements of target audience may not be met [13]. Needs assessment was accomplished satisfactorily at our University through expert panel discussions. But an array of needs assessment approaches would make a programme inherently effective and marketable. Brown JD in his study on problems encountered in curriculum process identified that, its needs assessment had failed miserably. The reason being focus on only administrator needs overlooking other stakeholders, steering mismatch between teaching learning with assessment leading to complete disaster [5].
Faculty development activities are essential to academic vitality. Though curriculum skills are widely acknowledged to be an important part of faculty development, reports on outcomes of programs that teach those skills are rarely found in the medical education literature. Snyder S from her study concluded that faculty development fellowship produced a significant number of new curricula or enhancements to existing curricula of acceptable quality as a result of participation in the curriculum workshop series [14]. Faculty development initiatives are a crucial component of curricular change [15]. For teachers to effectively carry out the role of curriculum implementation, adequate and elaborate training is a must. Implementation problems are bound to occur if formal training is lacking to educate faculty regarding steps involved in CD [16]. The present study uncovered the significant dearth of faculty training in CD. This would be the possible justification for having framing objectives to be most challenging step during CD. Also, the faculties expressed it to be a most significant hindering factor.
Beginners may find curriculum development process incomprehensible. Once the conceptual framework is in hand and attributes of curriculum design are understood, beginners must get acquainted to macro level and micro level planning, learning theory, and student assessment/program evaluation [17]. Kern’s six-step approach to curriculum development is an effective method that can be employed for developing educational products [18]. It provides “a practical, theoretically sound approach to developing, implementing, evaluating and continually improving educational experiences in medicine” [9]. The complex process of curriculum design is faced by challenges in each of its stages of development from the initial aim or objective, how it was developed and consensus reached. The participants expressed that step involving framing objectives followed by needs assessment as most challenging. Preparedness towards challenges would assist to deal them efficiently. Development of curriculum is time-consuming and challenging. Multiple roles of academicians at universities pose a challenge of devoting their valuable time towards CD. Also, it is strongly advised that CD time has to be explicitly and accurately identified as being a fixed number of hours for productive outcome [19]. Whatever may be the model of curriculum planning employed, the obligate necessity is well organised, strong and transparent planning process than emphasis on the type of model [20,21]. Success of any program in teaching and learning depends on careful planning of curriculum rather than just sheer chance [22].
Whatever may be the approach towards CD, authorities must give high priority to curriculum planning [21]. The major concern brought out in the current study concerning planning was that the process did not happen in a structured manner following each step one after the other. This taxed the faculty in terms of resource management and time.
The factors that influence curriculum from within and out with the institutional context can be isolated and examined one by one, but the true complexity and richness lies in their fluid interplay [23].
The support of administrators plays a critical role in implementation of change in curriculum practices. Significant differences in degree of implementation have been found in situations where assistance and support is received from supervisory personnel, including consultants [24]. The support from administration was one of a noteworthy enabling factor expressed by the partakers of this study.
The medical educators in India cater to diverse health professional educational courses in addition to medical programme. In the recent decade unprecedented growth in quite a lot of courses under health universities have posed a challenge in terms of CD and quality assurance. Also, the discrepancy in number of faculty intake and workload has affected the academic demands. Striking balance between regulatory bodies and additional expectations has added intricacy to new potential roles associated with curricular developments.
Incorporation of global standards into national educational standards would ensure quality preservation and improvement. Curricular efforts are the primary area of emphasis if the education seeks to globalise [25]. Global requirements were taken into account at our university the evidence being decent number of overseas students.
Monitoring is a periodic assessment that determines how the curriculum is working. To ensure quality there must be inbuilt monitoring system at organisational level. Several educators indicated their belief that other than some informal monitoring by Principals, little attention has been paid to the monitoring of implementation [15]. But Hal GE and Loucks SF sees implementation monitoring as a shared responsibility [26]. According to Kirkgoz Y, an important step in curriculum renewal is development of a system for monitoring. He suggested that communication with stakeholders through meetings served to get planned curriculum run smoothly via regular monitoring [27].
Though CD is one of the most significant matters in higher education; little attention has been given to the evaluation of curriculum, its review and transformation in the institutions [4]. It is rarely done in systematic manner with emphasis on aspects that have little role in modifying education. Even the present study stressed the deficiency in structured formal assessment of effectiveness of the programme which could be one of the major factors contributing to ultimate programme outcome. Spiel C et al., from their study on baseline systematic evaluation of curriculum and challenges confronted by evaluators recommended that it could be generalised to any other curricula. But special needs and apprehensions of various stakeholder groups should be taken into consideration [28].
Limitation
The number of participants in the study was major limitation. Extension of the study for remaining faculties has been planned. Similar studies should be executed across universities to identify and evaluate the factors that affects CD.
Conclusion
CD and revision are inseparable components of an educational process. Training of every faculty must be an essential element of educational programme. This holds good especially in health profession education where formal teachers’ training is not mandatory. Stringently adhering to each step in CD process would ensure proper alignment of course objectives to evaluate and contribute to successful educational outcome. Lastly, attentiveness concerning possible challenges and issues arising during the CD process would assist to anticipate them timely and act accordingly.