Osteoarthritis, a degenerative joint disease, includes group of mechanical abnormalities involving degradation of joints, including articular cartilage and subchondral bone. Globally, 15% world population is affected with osteoarthritis and is the leading cause of physical disability and impaired quality of life in elderly [1,2]. In India, osteoarthritis with a prevalence of 22% to 39% is the second most common rheumatological problem [3]. The Centre for Disease Control and Prevention has estimated a 46% lifetime risk of developing knee osteoarthritis and 25% lifetime risk of developing osteoarthritis of hip joint [4]. It is the 11th highest contributor to global disability [3].
The management goals include pain relief, improvement and maintenance of the range of movement of affected joints and limit the functional impairment [4]. The National Institute for Health and Care Excellence (NICE) guidelines suggest lifestyle modifications, muscle strengthening exercise and weight loss as core treatment for knee osteoarthritis [4]. If further treatment is required, then Acetaminophen (Paracetamol) is recommended first line oral analgesic. Other Non-Steroidal Anti-Inflammatory Drugs (NSAID’s) like Ibuprofen, Ketoprofen, Flurbiprofen, and Nimesulide are commonly used [5]. These agents reduce pain and improve physical function, however they do so temporarily without healing the cartilage and subchondral damage. Long term NSAID use is associated with risk for renal insufficiency, gastrointestinal bleeding, hypertension and congestive heart failure [1]. Moreover, optimal therapeutic benefits of Paracetamol require doses of up to 4000 mg/day, with the evidence on safety being still debatable [5]. Stronger analgesics like Tramadol, Morphine and Fentanyl are indicated for persistent pain; however, the benefit is outweighed by frequent adverse events and is not recommended for routine use [3]. Intra-articular corticosteroid injection provides only short term analgesic effect. A cochrane meta-analysis reported effectiveness of corticosteroid injections for only up to two weeks [6]. Joint replacement surgery reserved for advanced cases, too is associated with appreciable complications.
With this background, we hypothesized that the analgesic, anti-inflammatory, anti-arthritic and chondroprotective effect of the various ingredients might act in synergism to provide pain relief and slow down disease progression in osteoarthritis. Thus, we proposed to evaluate the clinical efficacy and safety of Myostaal Forte for pain relief and disease progression in patients with knee osteoarthritis. Besides being the first line oral analgesic for the treatment of knee osteoarthritis, Acetaminophen (Paracetamol) is used as a comparator in this study. In addition, no polyherbal formulation is used as a standard for the treatment of knee osteoarthritis and the available herbal formulations containing only one or two herbal ingredients could not be used for comparison of efficacy and safety of Myostaal Forte.
Materials and Methods
The study was conducted as a single centre, prospective, open-labelled, randomised, active controlled (CTRI:REF/2016/03/010991), 2-arm, parallel group, assessor blind study in Orthopaedics outpatient Department in collaboration with Department of Pharmacology and Therapeutics in a tertiary care hospital after obtaining Institutional Ethics Committee approval (IEC (II)/06/15). The study duration was six months, being initiated on 02/02/2015 and the last patient’s final visit was on 06/07/2015.
Selection Criteria
According to the ACR guidelines [19], diagnosed patients of idiopathic knee osteoarthritis for minimum six months to maximum five years, of either sex in age group 40–70 years were enrolled if the baseline knee joint pain was ≥40 mm on VAS and have not taken any oral analgesic, muscle relaxant, or low dose antidepressant for pain in the last two weeks.
Patients with secondary arthritis related to systemic inflammatory arthritis, auto-immune disease, uncontrolled hypertension, diabetes mellitus requiring insulin injections and chronic severe respiratory disease were excluded from the study. Patients receiving corticosteroids, glucosamine, chondroitin, topical gels, creams and ointments, hot or cold fomentation were also excluded. Patients with history of life threatening cardiovascular and/or neurological event and/or clinically active renal, hepatic or peptic ulcer disease, and acute exacerbation of osteoarthritis requiring hospitalisation were excluded from the study.
Study Methodology
A total of 64 eligible patients were consented and randomised by computer generated random code system into two groups. They were prescribed either Tab. Myostaal Forte TDS or Tab. Paracetamol (650 mg) TDS for six weeks and asked to follow up at two, four and six weeks. At baseline and follow-up visits, patients were assessed by orthopaedician using the modified WOMAC [20], VAS and global assessment questionnaire [21].
The predefined primary endpoint was decrease in pain and disease progression as evident by reduction in modified total WOMAC and WOMAC subscale scores at eight weeks. The secondary endpoints were change in VAS score, patient’s global assessment score, physician’s global assessment score from baseline to six weeks and incidence of adverse events.
The patient’s blood and urine sample was collected for routine biochemical investigations (complete haemogram, random blood sugar, liver function test, renal function test and urine routine and microscopy) at baseline and 6 weeks. Patients returned the empty strips to check for compliance. A trial diary was given to score daily pain, medication use, compliance and adverse effects, if any. At eight weeks, the general condition of the patient and the WOMAC score was noted by telephonic interview.
Rescue Medicine and Withdrawal Criteria
Patients with daily VAS score ≥ 70 mm for two consecutive days were prescribed Tab. Naproxen 750 mg/day as rescue medication for two days and assessed thereafter. Those requiring rescue for five consecutive days were withdrawn from the study.
The principal investigator or clinician could withdraw patient with severe disease evident from WOMAC score, if non-compliance reported in two out of three follow up visits and if a need to use any concomitant drugs during study that may interfere with assessment or influence the outcome.
Statistical Analysis
The data was tabulated using Microsoft Excel. The statistical analysis was done according to per protocol analysis using statistics software Graph pad Instat 3.1. Data was expressed as Mean±SD. For intra-group and inter-group comparison, unpaired t-test was used. Chi-square or Fischer exact test (if any value in the observation is less than 5) was used for comparing number of patients achieving reduction in the WOMAC and VAS scores. A p<0.05 was considered significant.
Results
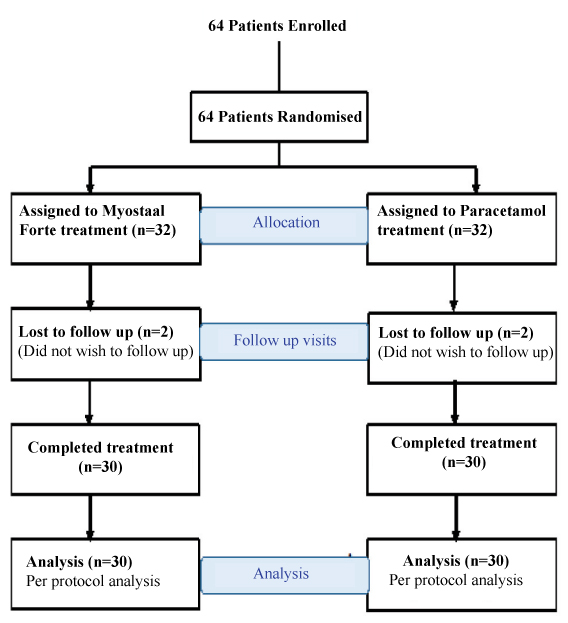
A total of 64 patients were recruited, out of which four lost to follow up (two from each group). In each group 30 patients completed the study duration [Table/Fig-1].
Flow diagram of the study.
Of the 60 patients, 44 were females and 16 were males. The mean age of the patients in the Myostaal Forte group was 54.64±7.47 years and 54.94±8.43 years in the Paracetamol group (p=0.884). The weight was comparable among patients in both the groups (p=0.771). The baseline WOMAC and VAS score was comparable in both the groups (p> 0.05) Table/Fig-2].
WOMAC subscale, total WOMAC and VAS score at baseline and each of the follow up visits in both the study groups.
| Variables/Visits | Baseline | Two weeks | Four weeks | Six weeks | Eight weeks |
|---|
| Study drug | MYO | PARA | MYO | PARA | MYO | PARA | MYO | PARA | MYO | PARA |
|---|
| WOMACSCORE | Pain | 12±2.80 | 11.2±2.75 | 10.1±2.14* | 10.43±2.42 | 8.74±1.70 | 8.6±2.54 | 6.93±2.05* | 7.2±2.85* | 6.34±1.94*† | 8.5±2.68* |
| Stiffness | 4.94±1.31 | 4.5±1.17 | 4.5±1.14 | 4.23±1.04 | 4.04±1.04 | 3.64±1.27 | 3.53±1.17 | 3.57±1.25 | 3.23±1.31 | 3.64±1.43 |
| Physical function | 42±9.23 | 40.67±8.62 | 36.97±7.72 | 36.5±8.75 | 32.9±6.70 | 32.34±8.44 | 27.13±6.0* | 29.4±7.79* | 24.17±7.31*† | 30±7.12* |
| Total | 58.93±12.11 | 56.57±1.33 | 51.74±10.04 | 51.16±11.1 | 45.67±8.40 | 45.57±11.11 | 37.6±8.0 | 40.17±10.61 | 33.73±9.53† | 42.13±10.19 |
| VAS Score | 68.4±9.44 | 67.24±11.32 | 62±9.1 | 61.17±10.79 | 52.9±9.1 | 52.9±11.69 | 47.8±6.59* | 47.67±11.5* | | |
MYO = Myostaal Forte, PARA = Paracetamol
Values are represented as Mean±SD
* p<0.05 as compared to baseline visit (Intragroup analysis)
† p<0.05 as compared to Paracetamol (Intergroup analysis)
The change in WOMAC subscale scores from baseline to eight weeks was statistically significant in both study groups on within group analysis except stiffness which was non significant. Baseline to two weeks revealed a statistically significant reduction in the WOMAC pain subscale score in the Myostaal Forte group, however, the same was not significant in the Paracetamol group. (p<0.05) [Table/Fig-2].
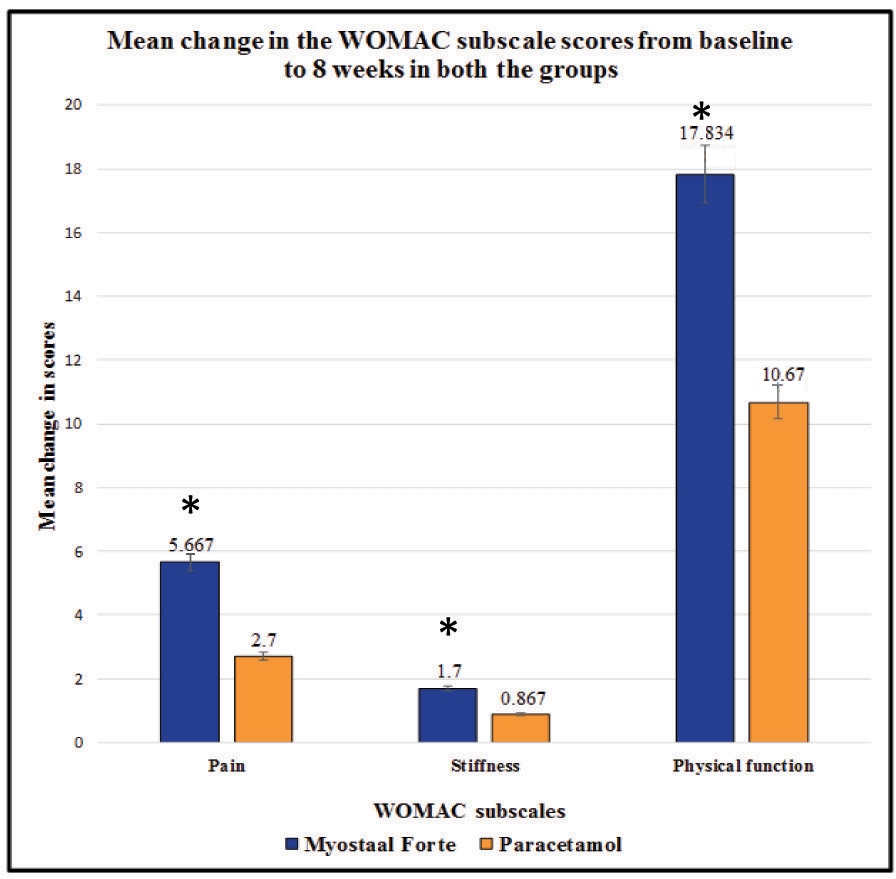
The total WOMAC score at each visit was comparable between the two treatment groups, except at eight weeks, when a statistically significant difference was seen in the Myostaal Forte group as compared to the Paracetamol group (p<0.05) [Table/Fig-2]. Even the change in WOMAC subscale scores was statistically significant at eight weeks in Myostaal Forte group as compared to Paracetamol group (p<0.05) [Table/Fig-3].
Mean change in WOMAC subscale scores from baseline to eight weeks in both the group.
Mean change in WOMAC subscale scores was statistically significant at eight weeks in Myostaal Forte group as compared to Paracetamol group.
* p<0.05 considered significant as compared to Paracetamol group.
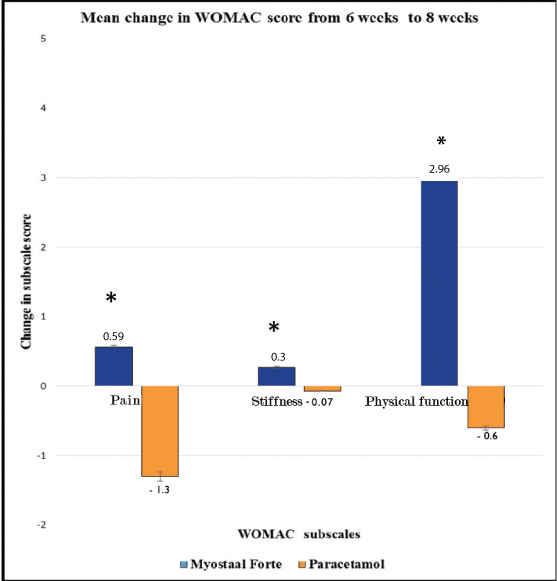
At eight weeks, the WOMAC pain and physical function score was significantly better in the Myostaal Forte group as compared to the Paracetamol group. The WOMAC stiffness subscale score was comparable between the two study groups [Table/Fig-2] From six weeks to eight weeks, the change in the WOMAC pain score was 0.56±1.15 in the Myostaal Forte group and -1.3±1.99 in Paracetamol group and this difference was found to be statistically significant. The change in the WOMAC stiffness score in the Myostaal Forte group was significantly better 0.27±0.65 as compared to the Paracetamol group -0.07±0.80. The change in WOMAC physical function subscale score was significantly positive in the Myostaal Forte group 3.9±3.79 as compared to the negative change in the Paracetamol group -0.6±4.1 [Table/Fig-4].
Mean change in WOMAC score from six weeks to eight week.
From 6 weeks to eight weeks, the change in the WOMAC pain, stiffness and physical function score in the Myostaal Forte group was statistically significant as compared to the Paracetamol group.
*p<0.05 considered significant as compared to Paracetamol group
Analysis of secondary efficacy variables revealed statistically significant change in VAS score from baseline to six weeks in both the Myostaal Forte and Paracetamol group. However, inter group analysis did not reveal any significant difference in the VAS score at six weeks. (p>0.05) [Table/Fig-2]). The mean change in the VAS score from baseline to each of the follow up visit was also comparable between the two groups (p>0.05) [Table/Fig-2].
The number of patients with decrease in the pain intensity from baseline to six weeks was statistically significant in both the treatment groups (p<0.05) [Table/Fig-5].
Distribution of patients according to VAS score at baseline and at six weeks in both the study groups.
| VAS score/Treatment Group | Myostaal forte group | p-value | Paracetamol group | p-value |
|---|
| Baseline | Six weeks | Baseline | Six weeks |
|---|
| Mild | 2 | 10 | 0.0013* | 1 | 9 | 0.0007* |
| Moderate | 20 | 20 | 21 | 21 |
| Severe | 8 | 0 | 8 | 0 |
Data represents number of patients, per protocol analysis.
Chi-square test; *p<0.05 considered significant.
Of the eight patients with severe pain at baseline, in two weeks the pain severity reduced to moderate in all eight patients in Myostaal Forte group, whereas in only four patients in Paracetamol group. The difference was found to be statistically significant (p<0.05).
All patients in both groups showed a satisfactory improvement in the physician’s global assessment. On patient’s global assessment, 30 patients in Myostaal Forte group and 24 patients in Paracetamol group felt a complete symptomatic relief with a comparable statistical significance.
On safety assessment, eight patients in Paracetamol group and three patients in Myostaal Forte group experienced adverse events. Paracetamol group patients suffered from gastric acidity, heartburn (n=7), sedation (n=1), fatigue and generalised weakness (n=2) and itching with dryness of skin (n=1). Abnormal laboratory parameters were detected at six weeks in three patients with Myostaal Forte treatment. A total of two patients had asymptomatic decrease in RBC count and haemoglobin level and one patient had abnormal increase in random blood sugar levels. However, there were no significant adverse events and changes in the laboratory parameters and the compliance to treatment was excellent in both the groups.
Tolerability was rated as excellent by 100% of the Myostaal Forte treated group, and 80% of the Paracetamol group with no significant adverse events attributable to either Myostaal Forte or Paracetamol.
Discussion
Present study evaluated the clinical efficacy and safety of Myostaal Forte in knee osteoarthritis. We found that Myostaal Forte elicited significant reductions in pain, stiffness and functional indices of osteoarthritis disease activity in eight weeks. An early onset pain relief was seen with significant reduction in the WOMAC pain score and a higher number of patients with decreased pain intensity on VAS scale from baseline to two weeks. On treatment cessation after six weeks, change in WOMAC subscale scores were significantly positive, indicating a carryover effect that can be potentially useful in maintainence of remission.
Experimental studies on Myostaal Forte have shown a significant time dependent protection against chondrocyte layer damage and palliation of inflammation in a model of Monoiodoacetate induced osteoarthritis. This effect was attributed to its ingredients Shodhit Guggulu (Processed Commiphora wightii) and Shallaki (Boswellia serrata) [2]. Moreover, experimental studies on the individual herbal ingredient has shown that processed Commiphora wightii, Withania somnifera, Curcuma longa, Tinospora cordifolia, Alpinia galanga and Vitex negundo possess analgesic and chondroprotective effect on diseased osteoarthritic cartilage by varying mechanisms [2,9-11,13,15]. Triterpenoids present in Boswellia serrata and Zingiber officinale possess analgesic effect by virtue of selective inhibition of cyclooxygenase-2 enzyme thereby lessening the gastrointestinal side effects [12,22]. Arabinogalactan polysaccharide in Tinospora cordifolia has shown to induce significant increase in the joint cartilage thickness in preclinical studies [11]. Sesquiterpene isolated from Cyperus rotundus has demonstrated positive modulation of GABAergic neurotransmission [14]. Thus, our study suggest the possibility that the active constituents of the herbs such as triterpenoids, curcuminoids, arabinogalactan, gingerols, isocurcumenol act synergistically leading to the overall analgesic and chondroprotective effects of Myostaal Forte.
A few clinical trials with the main individual herbal ingredients of Myostaal Forte in patients with knee osteoarthritis support the results of the present study [22-24]. Corroborating with the results of the present study, a double-blind randomised trial evaluated the efficacy and safety of Boswellia serrata in knee osteoarthritis and revealed clinically and statistically significant improvement in the WOMAC pain score and functional ability with the test drug as early as seven days of treatment [22]. Myostaal Forte thus represents a good therapeutic alternative for pain relief in acute flares in moderate to severe cases of knee osteoarthritis.
A clinical trial with Commiphora wightii in knee osteoarthritis revealed a significant improvement in the total WOMAC score in one month and continued improvement during the second month after treatment cessation. The study prominently showed improved pain and functional ability which was sustained over baseline values even when the treatment was stopped for a month, apparently due to chondroprotective properties of the herb [23]. Our study with Myostaal Forte Tablets, containing Commiphora wightii and Boswellia serrata the primary ingredients, show an analogous carry over effect consistent with this previous study. In addition, the cartilage protective property of Shallaki, Ashvagandha, Haridra, Guduchi, Kulanjana, Musta and Dashamoola may further be contributing to persistent effect after treatment discontinuation.
A clinical evaluation of another polyherbal formulation containing Withania somnifera, Boswellia serrata, Zingiber officinale, and Curcuma longa revealed a statistically significant reduction in the VAS and WOMAC scores compared to placebo [24]. The present study with Myostaal Forte, which contains all these plant extracts in addition to other herbs with an anti-inflammatory and chondroprotective potential, revealed results that were consistent with this study.
Drop-outs from the study were in an acceptable rate, with majority due to non-availability for follow-up. The present study design did not include a placebo arm, and as such poses limits to the interpretation. However, the advantage of this approach is that need for rescue medication is less and the data may not be clouded by the mixed effects of both treatment and rescue medication. The study being assessor blind, the results we have received can be credible. However the fact that patient was non-blinded could have given a favourable subjective response. Therefore, we recommend a double blind randomised controlled trial in future to create a stronger level of evidence.
Conclusion
Myostaal Forte and Paracetamol both produced a steady reduction in osteoarthritis symptoms, particularly pain. The investigational drug Myostaal Forte was safe and well tolerated. Myostaal Forte resulted in significantly faster onset of pain relief as compared to Paracetamol, suggesting therapeutic application in acute pain in knee osteoarthritis. The symptomatic relief was sustained over two weeks after treatment cessation in Myostaal Forte, whereas following discontinuation of Paracetamol, relapse of pain and physical disability occurred within two weeks. Presumably, the pleotropic beneficial effects of Myostaal Forte is due to a conflux of multiple active ingredients acting synergistically which provides potential analgesic, anti-inflammatory and chondroprotective efficacy.
Conflict of Interest: One of the co-investigator, Dr. M. B. Chawda, is associated with the sponsor, ‘Solumiks Herbaceuticals Pvt Ltd’ which provided financial support for the clinical trial. No other relationships or activities have influenced the submitted work.
MYO = Myostaal Forte, PARA = Paracetamol
Values are represented as Mean±SD
* p<0.05 as compared to baseline visit (Intragroup analysis)
† p<0.05 as compared to Paracetamol (Intergroup analysis)
Data represents number of patients, per protocol analysis.
Chi-square test; *p<0.05 considered significant.