Anomalous Muscles Encountered in the Carpal Tunnel: A Report of Two Cases
Laxminarayan Bhandari1, Michelle Palazzo2
1 Senior Fellow, Hand and Microsurgery, Christine M Kleinert Institute, Louisville, Kentucky, USA.
2 Program Director, Hand and Microsurgery, Christine M Kleinert Institute, Louisville, Kentucky, USA.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Laxminarayan Bhandari, Abraham Flexner Way, Suite 850, Louisville, Kentucky, USA 6102027938
E-mail: lax321@gmail.com
Anomalous muscles are infrequently encountered in carpal tunnel surgery. They are challenging to identify and may mislead the surgeon by obscuring normal anatomy. Hence knowledge of their presence is essential. We report two cases of anomalous muscle encountered in the carpal tunnel during surgery. First case consisted of an anomalous muscle seen in carpal tunnel release surgery. The muscle had proximal tendinous origin at wrist and distal tendinous insertion on index finger. In the second case, we incidentally encountered an anomalous muscle, which originated from the distal end of radius, travelled through the carpal tunnel and fused with the flexor digitorum superficialis of the small finger. Through this case report we have discussed the current concepts regarding anomalous muscle in the carpal tunnel and its management.
Anomaly, Carpal tunnel syndrome, Lumbricals
Case Report 1
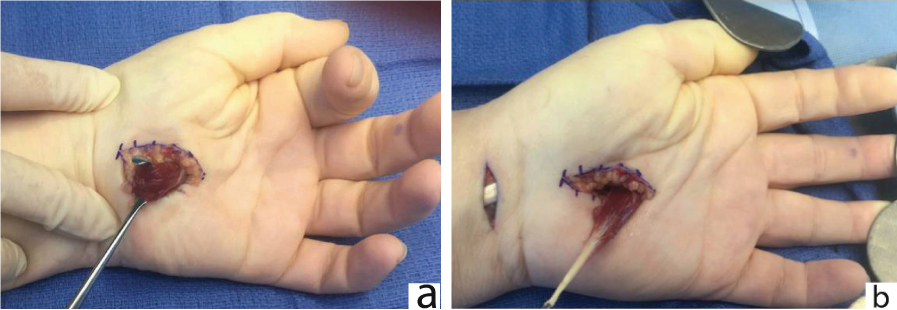
A 58-year-old female presented with bilateral tingling and numbness of the hands since past one year with occasional night symptoms. She had a positive Phalen test and Tinel’s sign at the carpal tunnel without thenar atrophy. The nerve conduction test was consistent with severe bilateral carpal tunnel syndrome. She previously had open carpal tunnel release on right side at another hospital six months ago without symptomatic relief. On left side, conservative treatment with multiple steroid injections failed to relieve her symptoms. Surgery was offered on her left side first. Under axillary block with tourniquet control, after opening the transverse carpal ligament, we identified a muscle in the carpal tunnel which was superficial to the Flexor Digitorum Superficialis (FDS) [Table/Fig-1]. Pull on the muscle led to proximal interphalangeal joint flexion of index finger. Within the carpal tunnel we could identify all four FDS and Flexor Digitorum Profundus (FDP) tendons. A 2 cm horizontal incision was placed in wrist crease. The tendinous origin of the muscle was divided. Muscle was retrieved through the proximal incision and divided distally. Three months later she underwent revision carpal tunnel release on her right side. No anomalies were noted. On One-month postoperatively the patient was doing well with full range of motion and improvement of symptoms.
a) Anomalous muscle in carpal tunnel, traction on which produces index proximal interphalangeal joint flexion. b) Tendinous origin of muscle excised from volar wrist incision and muscle retrieved into palm.
Case Report 2
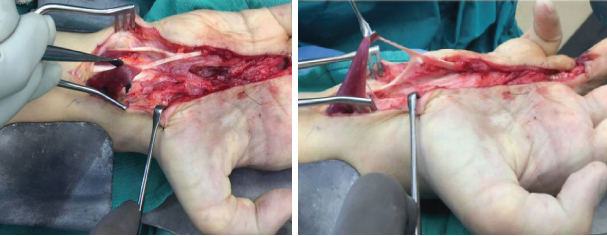
An anomalous muscle was identified while operating on a 24-year-old male for a crush injury to the hand. He had sustained tendon injury to his right ring finger as well as the median nerve. While operating, we encountered an anomalous muscle in the carpal tunnel, which originated from the distal end of radius, travelled through the carpal tunnel and its tendon fused with the FDS tendon to the small finger [Table/Fig-2]. The transverse carpal ligament was divided. The anomalous muscle was not resected as the patient did not have any symptoms of nerve compression. The patient underwent flexor digitorum profundus tendon and median nerve reconstruction as scheduled. One month postoperatively he recovered well and is undergoing physical therapy.
Anomalous muscle with its muscular origin from distal radius and tendon inserted into flexor digitorum superficialis of small finger.
Discussion
Anomalous muscles in carpal tunnel present a clinical challenge. Especially in small incision open carpal tunnel release surgery, since minimal exposure can make identification of anatomical anomalies difficult. Anatomical variations can obscure standard landmarks and may lead to incorrect tissue planes dissection. Furthermore, in clinical surgery, extending the incision in order to identify the origin and insertion of a muscle is undesirable due to the added morbidity to the patient. Hence, we believe anatomical descriptions are invaluable [1].
The exact cause of such anomalies is not known. Some authors contributed such anomalies to the “Ontogeny recapitulates phylogeny” theory [2]. However, that theory itself has largely been discredited [3]. It is known that the muscles originate by migrating myocytes directed into muscle anlage by tendon primordium. The anomalies are likely due to aberration in embryological signalling.
The anatomical variations seen in the carpal tunnel can be broadly divided into anomalies of the nerves, tendons, vessels, and muscles. The incidence of such anomalies encountered in carpal tunnel surgery is reported between 9.9-11.7% [4]. The muscular anomalies can be anomalous FDS, anomalous lumbricals, or palmaris profundus [Table/Fig-3]. Although these are the broad types, often times it is not possible to define an anomaly due to overlapping features [5-7].
Broad classification of various types of muscular anomalies encountered in Carpal tunnel in previous studies.
| Anomaly | Description | First reported by | Reference no. |
|---|
| Flexor Digitorum Superficialis | Muscle fibers are limited to the FDS. They originate from Distal radius, Ulna or ever FDS to get inserted into FDS. | Mainland in 1927 | [5] |
| Anomalous Lumbricals | Anomalies can be seen in their origin, attachment or numbers. They may arise from FDS or FDP; and may be tendinous with minimal muscle or predominantly muscular. The first case in this report was likely an anomalous lumbrical. | Butler and Bigley in 1971 | [6] |
| Palmaris profundus | Accessory muscle arising from the distal aspect of radius or ulna and inserting into palmar aponeurosis. The second case described in this report is likely to be Palmaris profundus. | Frohse and Frankel in 1908 | [7] |
The anomalous muscle in our first case was likely to be accessory lumbrical, as it has tendinous origin and insertion. Although we did not explore the origin and insertion, it is likely that the muscle originated from one of the flexor muscle proximally to get inserted into the FDS tendon distally. The second case was likely Palmaris profundus, having muscular origin from distal end of radius and distally the tendon fusing with FDS tendon of small finger.
The literature is not conclusive as to whether the anomalous muscle can cause clinical nerve compression. In most cases, the authors have advocated resection of the anomalous muscle [8]. There are reports where the patients are managed with just release of the carpal ligament, without resection of the muscle [9], or even with physical therapy alone [10]. However, it must also be noted that, the resection of these anomalous muscles did not lead to any residual deficits. Hence, we suggest excision of the muscle when there is a suspicion of it causing the compression, only after identifying the existence of normal structures to preserve function.
In some cases, preoperative MRI or even ultrasound may reveal the diagnosis [11]. However, imaging is not routinely done for carpal tunnel syndrome, and surgeon’s first encounter likely will be intraoperatively.
Conclusion
Anomalous muscles in the carpal tunnel include lumbricals, flexor digitotum superficialis, and palmaris profundus, however overlapping features are common. The literature is not conclusive as to whether these anomalies can cause nerve compression. However, when encountered intraoperatively, we suggest excision of the muscle when there is a suspicion of added compression, but only after identifying normal structures to preserve function.
[1]. Trivedi S, Satapathy B, Rathore M, Sinha MB, A rare case of anomalous origin of first lumbrical from the tendon of flexor digitorum superficialis to index fingerJ Clin Diagn Res 2016 10(11):AD03-AD04. [Google Scholar]
[2]. Elliot D, Khandwala AR, Kulkarni M, Anomalies of the flexor digitorum superficialis muscleJournal of Hand Surgery 1999 24(5):570-74. [Google Scholar]
[3]. Lovtrup S, On von Baerian and Haeckelian recapitulationSystematic Zoology 1978 27(3):48-52. [Google Scholar]
[4]. Tountas CP, MacDonald CJ, Bihrle DM, Carpal tunnel syndrome. A review of 507 patientsMinn Med 1983 66(8):479-82. [Google Scholar]
[5]. Mainland D, An uncommon abnormality of the flexor digitorum sublimis muscleJournal of Anatomy 1927 62:86-89. [Google Scholar]
[6]. Butler B, Bigley EC, Aberrant index (first) lumbrical tendinous origin associated with carpal tunnel syndromeJ Bone Joint Surg [Am] 1971 53(1):160-62. [Google Scholar]
[7]. Frohse F, Fränkel M, Die Muskeln des Menschlichen Armes. In: Bardeleber K, editorHandbuch der Anatomie des Menschen. Bd2 1908 Gustav FischerMünchen Jena:115-118. [Google Scholar]
[8]. Bakriga B, Amouzou KS, Ayouba G, Kombate N, Dellahn Y, Walla A, Anomalous muscles: a rare cause of carpal tunnel syndrome: a case reportInternational Journal of Orthopaedics 2017 4(1):705-07.Available from: URL: http://www.ghrnet.org/index.php/ijo/article/view/1959 [Google Scholar]
[9]. Javed S, Woodruff M, Carpal tunnel syndrome secondary to an accessory flexor digitorum superficialis muscle belly: case report and review of the literatureHand (NY) 2014 9(4):554-55. [Google Scholar]
[10]. Zeiss J, Jakab E, MR demonstration of an anomalous muscle in a patient with coexistent carpal and ulnar tunnel syndromeCase report and literature summary: Clin Imaging 1995 19(2):102-05. [Google Scholar]
[11]. Pardal-Fernandez JM, Carpal tunnel syndrome. The contribution of ultrasonographyRev Neurol 2014 59(10):459-69. [Google Scholar]