Intact surgical gloves are the most important barrier to bi-directional migration of micro-organisms between the hands of the surgical team members and patient [1,2]. Although surgical glove perforations correlate with duration of wear, yet very few prospective studies have addressed this issue in orthopaedic settings. Although use of single gloves is unsafe, Double glove use is still not universal [3]. Although double gloving offers protection to the surgical team by preventing intraoperative blood exposure [4]; it also causes discomfort and reduced sensitivity [5].
The surgical gloves are changed at various junctures during the surgery and in a routine orthopaedic case. The glove consumption may vary anywhere from 9-15 pairs depending on the persons and number of times they are changed. The scientific basis and effects of this practice is still not established, but we learnt that surgical team performs glove change fearing contamination, long exposure to external environment, personal beliefs or carelessness by surgical team members who may in turn be the implantation source while handling and transfer of surgical instruments to operating surgeon. We performed a prospective multicenter study to determine the rationale of frequent glove change during orthopaedic surgeries, differences amongst surgical parameters with and without changing the surgical gloves and whether this had an effect on surgical and functional outcomes.
Materials and Methods
From January 2014 to January 2016, a prospective multicenter study was conducted at three centers with dedicated orthopaedic operation theatres equipped with in house microbiological testing laboratories to determine the rationale of glove change during orthopaedic procedures and whether frequent glove change affected surgical parameters or clinical outcomes. The centers included were Hi-tech Medical College (Bhubaneswar-147 cases), Care hospital (Bhubaneswar- 52 cases) and Kalinga Hospital (Bhubaneswar-51 cases). Ethical clearance obtained from the ethical committee.
Patient Selection and Data Collection
Patient selection, informed consent from all the patients and patient details were obtained using a standard protocol by three surgeons (A, B and C). All surgeries were performed by the same surgical team. For each surgical procedure the patient’s name, date of birth, gender, underlying disease, surgical team members, surgical team member’s role, nature of the surgery, surgical duration, glove wear duration and puncture sites were noted. Surgical time was counted from skin incision to skin closure timing. A preoperative antibiotic (1.5 gm cefuroxime) was given intravenously 30 minutes prior to skin incision in all patients [6].
Patients included in the study were non-compound fracture fixation, intramedullary nailing or plating, soft tissue procedures like tendo achilles reconstruction and ACL reconstruction, hemiarthroplasty femur and Arthroscopic shoulder/Knee procedures. Patients excluded from the study were compound fractures, infection at any site and diabetes/septicaemia and refusal for consent.
Surgical parameters assessed were Surgical Timing, Glove Consumption, Microperforations, Surgical Cost. Clinical Outcomes assessed in both the groups were Wound Healing, Surgical Site Infection, Rehabilitation Timing, Fever etc.
Randomisation
A total of 250 patients were divided into 2 groups (n=125 each) based on a computer generated number by a person unaware of the study. In Group 1, surgical team operated with regular changing of gloves. In Group 2, only 1 set of double gloves were worn throughout the procedure, changed only in presence of an obvious or inner glove tear. Patients from both the groups were followed up for two months postoperatively.
Experimental Procedure
The gloves used throughout the study were ‘Surgicare’ Sterile Latex Powdered Surgical Gloves (FDA approved) made from natural rubber latex with minimum length of 280 mm and a sterility assurance level of 106 and a sterilant residue less than 5 ppm. The surgical gloves Conformed to International standards ASTM D 3577, ASTM D 3578, EN 455 part I, II and III and had a Factory Standard of AQL 1.5 (ASTM Standard AQL 4.0).
The surgical team was blinded from the study to prevent bias. In Group 2 surgeries, the team was instructed to wear only one set of double surgical gloves throughout the procedure which they could change in presence of an obvious glove tear. Before surgery, each surgeon performed surgical hand disinfection (“surgical scrub”) according to the reference surgical hand-disinfection procedure described in EN 1500, but scrub extended from the forearms to middle and distal third junction of arm till the contact time [7]. After thorough drying of the hands with a clean, disposable paper towel, hands and forearms were disinfected over a period of 3min with an alcohol-based hand disinfectant. After evaporation of the alcohol, surgeons wore sterile single set of double surgical gloves before the surgical procedure.
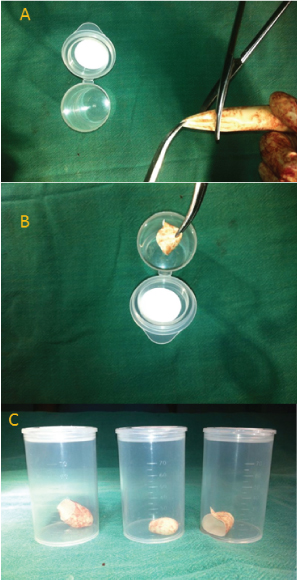
In Group 1, team members changed gloves regularly; therefore after surgery 1125 index finger portions (125*3*3) of dominant hand outer gloves over 125 operations were retrieved from surgeons, assistant surgeons and scrub nurse in Group 1. In group 2, the surgical team did not change gloves thus 375 index finger portions (125*3) of dominant hand outer gloves over 125 operations were retrieved from surgeons, assistant surgeons and scrub nurse in Group 2. The samples were collected in sterile plastic containers, coded and sent for Microbiological Testing (gram’s staining and standard cultures with various media) [Table/Fig-1].
Glove collection protocol for gram’s staining and standard cultures (a- Index finger tip pulled and cut; b) Sample put in sterile container; c) 3 samples put in sterile container and coded).
The outer dominant hand glove was reserved for microbiological testing in all cases. Therefore, the outer dominant hand glove was subjected to microbiological testing only and not micro-perforation testing.
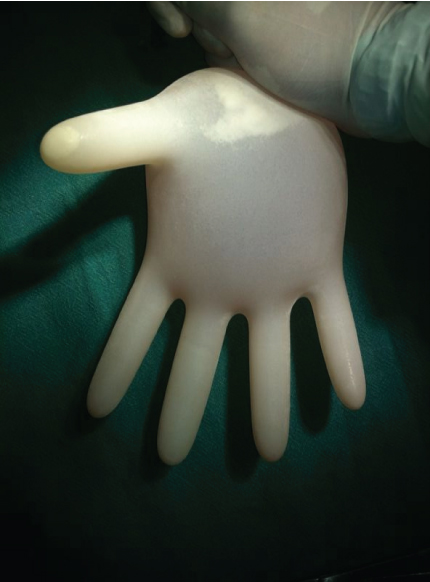
Micro perforation testing using water tight test was performed on outer non-dominant hand glove (unilaterally only) and both the inner gloves from both the groups using Watertight test (NF EN 455-1) [8,9].
In the watertight test, 1000cc water was filled in the vertically hanged gloves, any immediate leakage of water was noted and gloves were reexamined after 2-3 minutes for water leak [Table/Fig-2]. However, if the outer non-dominant hand glove sample was positive for microperforation, both the outer gloves for that pair (dominant and non-dominant hand glove or bilateral) would be considered punctured and reported.
Water-Tight test (European Norm 455, part 1).
Microbiology Processing
Gram’s staining was performed directly from these samples and culture was performed on freshly prepared Blood Agar Solid Media, chocolate agar media and MacConkey’s media in sterile petridish and thioglycollate liquid media, Peptone Water Liquid Media in sterile glass test-tubes by direct inoculation. Agar plates were incubated for 72hours at 37±1°C in a bacteriological incubator. Colony forming unit were counted and recorded at 24, 48 and 72 hours. Gram’s staining was reported at end of 24 hours.
Statistical Analysis
Statistical analyses included the median, mode, range, Interquartile Range (IQR) and sample standard deviation (s). Bacterial counts were expressed as median with (IQR). The independent-samples t-test was performed to compare two group’s scores on the same variable. The variables were tabulated in the Excel software. The data were analyzed descriptively and organized in tables and graphs. A value of p<0.05 was considered statistically significant. The 95% confidence intervals were measured when appropriate. Statistical analyses were performed using SPSS 13.0. (SPSS Inc, Chicago, IL, USA).
Results
The average participants per surgical procedure were 2 surgeons and 1 scrub nurse (Interquartile Range: 2.75–3.75) and Surgical timing varied from 30- 210 minutes (mean-103 mins). In Group-1, mean age of patients was 54.6 years (S.D-9.2) and range 45.4-63.8 years and in Group-2, mean age of patients was 51.9 years (S.D-8.4) and range 43.3-60.3 years. The shortest procedure was nail dynamisation with 30 (S.D-15 mins) and the longest procedure was 130 (S.D-15 mins).
Microbiological testing revealed growth in one glove sample from Group-2, where the surgeon sample showed deposits in peptone water culture, which was sub-cultured and revealed AcinetobacterBaumannii in a case of bone biopsy of a pathological fracture clavicle with bony collapse. There were no instances of whole team contamination. Glove contamination rate in Group-2 was 0.2%.
Micro perforation testing revealed 64 pair outer glove punctures in 375 pair of outer gloves tested over 125 operations from Group-2. In Group-1; 138 pair of outer gloves was punctured in 1125 pairs of outer gloves tested over 125 operations from Group-2. None of the inner gloves were perforated in either group on all occasions [Table/Fig-3]. This gives an outer glove perforation rate of 5.85% in Group-1 and 8.15% in Group-2 with overall outer glove perforation rate of 7.42%. Obvious outer glove tears were observed in Surgeon’s glove during 8 surgical procedures, for which the outer pair of gloves were changed (3 times in Group-1 and 5 times in Group-2). Micro perforation pattern revealed index finger to be the most common perforation sites.
Micro perforation pattern.
| Micro Punctures | Index Finger | Middle Finger | Both Index and Middle | Thumb |
|---|
| OUTER GLOVES:(Non-Dominant Hand Glove) | | | | |
| Group-1 (138 out of 1125) | 67 | 45 | 15 | 11 |
| Group-2 (64 out of 375) | 34 | 21 | 5 | 4 |
| INNER GLOVES: (Bilateral) | | | | |
| Group-1 (0 out of 1125) | - | - | - | - |
| Group-2 (0 out of 375) | - | - | - | - |
Micro-perforation incidences were proportional to duration of surgical procedures; operations lasting 120-210 minutes had 66.6% outer glove puncture rates, 61-120 minutes had 37.2% outer glove puncture rates, 30-60 minutes had 20% outer glove puncture rates (p<0.05). Bony procedures had higher perforation rates of 58% than soft-tissue procedures of 50% (p<0.05). The mean operative time for bony procedures was 124.5 (range 30-210) minutes while that for soft tissue operations was 96.4 (range 90-100) minutes. Surgeons had higher glove perforation rates of 51.2%, while assistant’s glove perforation rate was 34.5%, there were no perforation in the scrub nurse’s gloves.
Surgeries in Group 1 had increased surgical timing of 5.8 to 14.2 minutes (p<0.05) and increased glove consumption of 9-15 pairs (p<0.05) as compared to surgeries in Group-2 with glove consumption of 6 pairs. Group-1 surgeries were costlier than Group-2 surgeries by 150 to 450 Rupees depending on the glove consumption in each surgery [Table/Fig-4].
Surgical Variable comparison in Group-1 and Group-2.
| S.no | Surgical Variable | Group 1 | Group 2 | p-value |
|---|
| 1. | Surgical Timing Difference | 10 +/- 4.2 minutes | - | (<0.05) |
| 2. | Glove Pair Consumption (minimum)* | 9-15 pair | 6 pair | (<0.05) |
| 3. | Surgical Cost Difference** | +Rs.150-450 | - | (<0.05) |
| 4. | Micro-perforations Rate (outer) | 5.85% | 8.15% | |
| 5. | Micro-perforations Rate (inner) | nil | nil | |
| 6. | Bacterial contamination | nil | 1 sample (Surgeon) | |
| 7. | Surgical Site Infection | nil | nil | |
| 8. | Biomedical Waste Load | More | Less | |
*- 3 member team; 9,12,15 for 1,2,3 changes respectively.
**- Rs 150,300,450 for 1,2,3 changes per procedure respectively.
The postoperative course of patients in both the groups was normal. There was no incidence of surgical site infection or early postoperative complications in either group. At two months, patient from both groups had no surgical site infection, similar wound healing and rehabilitation timings. Moreover, the surgical team members were safe from micro-punctures and thus physical contact with patient’s blood and fluid. As none of the inner gloves were perforated throughout the study. This intact barrier prevents bidirectional load of microorganisms thus preventing infections. Also, all the patients in our study were screened for routine viral markers before they were operated. Moreover, all the hospital employees are screened regularly for viral markers as a general practice and protocol.
Discussion
Various reports recommend that surgical team members in operating field should change gloves after 30 to 180 [10,11] minutes of surgery owing to increase in the rate of micro-perforation over time [10]. During any surgical procedure, call for a glove change is made by the operating surgeon himself. Overall glove consumption for each surgical procedure depends on surgeon’s habits and beliefs. Surgical glove cost contribute significantly to operation costs with each pair ranging anywhere from Rs. 45-80 per pair. In our study, we observed that under standard operating conditions; routinely changing surgical gloves does not affect the peri or postoperative course of the patient and the results are similar to operations performed without changing gloves throughout the procedure. Also, surgical team safety was maintained due to absence of micro-perforations of inner gloves, thus making them safe to be continued throughout procedure.
Whereas, various authors have reported glove perforation rates of 12-15% [4,9,12,13]. We report outer glove perforation rate of 5.85% in Group-1 and 8.15% in Group-2 with overall outer glove perforation rate of 7.42% and no inner glove perforation. Double gloving reduces the glove failure incidence and thus diminishes surgical team member’s exposure to patient’s blood [14] and fluids thereby reducing infection incidence. The surgical procedures involving regular changing of surgical gloves (group-1) had low outer glove micro perforation rates but longer duration, higher surgical costing and high biomedical waste load per surgery for similar operative procedures as compared to ones performed without changing of surgical gloves (group-2) [Table/Fig-4].
Even a good preoperative surgical hand disinfection reduces, but not eradicates the resident flora on the surgeon’s hands, and thus does not eliminate the risk of transmission of such organisms into the surgical site in the event of a glove breach, therefore an intact glove barrier is desirable to check cross migration of microorganisms [15,16]. We report a 0% inner glove puncture even without changing the surgical gloves throughout the procedure.
Thus, the surgical procedures performed with regular changing gloves had significant high surgical cost (p<0.05) and surgical timing (p<0.05). The postoperative wound condition, suture removal and functional results were similar in both groups. There were no incidences of infection throughout the study.
By adopting standard and meticulous surgical behavior and refraining from unnecessary glove change, surgical cost can be brought down. In our country, people struggle hard to earn even a single rupee, mostly sell off their investments to afford a decent treatment for near and dear ones. Any cost between Rs 150-450 per operation can be reduced from overall surgical cost, which on a national scale becomes a significant figure. Judicious surgical glove consumption is a patient friendly and environment friendly option too, thereby also reducing the hospital’s biomedical waste load. Moreover, similar surgical and functional results were observed in procedures performed with or without glove change.
Intramedullary nailing or plating, soft tissue procedures like tendo achilles reconstruction or bursectomy, Hemi-arthroplasty Femur and Arthroscopic shoulder/knee procedures can be performed with a set of double gloves worn throughout the procedure, changed only in presence of obvious glove tear.
It is recommended to use a pair of double gloves in all orthopaedic procedures. This adds to the surgical team safety and reduces infection incidences. The limitations of our study were a limited number of patients (n=250) and limited orthopaedic procedures. In the future, the study’s inclusion criteria can be expanded to complex surgeries like Knee, Shoulder and Hip arthroplasty, Arthroscopic Multiligamentous Reconstruction and Deformity Correction procedures and to perform study on a larger group and include more centers.
Conclusion
Under standard operating conditions, procedures performed without glove change are shorter and cost effective than procedures performed with regular changing of surgical gloves. Surgical and functional results are similar in procedures performed with or without changing surgical gloves.
Double surgical gloves offer added protection to the surgical team. A surgical glove needs change only in presence of obvious or inner glove tear. Judicious use of surgical gloves is a patient and environment friendly option, thereby reducing the hospital’s biomedical waste load.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this manuscript.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
*- 3 member team; 9,12,15 for 1,2,3 changes respectively.
**- Rs 150,300,450 for 1,2,3 changes per procedure respectively.