The Inflated Urobag Technique for Accessing the Pelvicalyceal System during Prone Percutaneous Nephrolithotomy in a Ptotic Kidney
Suresh Bhat1, Yateesh Srinivasa2, Fredrick Paul3, Ashwin Giridhar4, Manjunath Sathyanarayana5
1 Professor, Department of Urology, Government Medical College, Kottayam, Kerala, India.
2 Senior Resident, Department of Urology, Government Medical College, Kottayam, Kerala, India.
3 Associate Professor, Department of Urology, Government Medical College, Kottayam, Kerala, India.
4 Senior Resident, Department of Urology, Government Medical College, Kottayam, Kerala, India.
5 Senior Resident, Department of Urology, Government Medical College, Kottayam, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suresh Bhat, Professor, Department of Urology, Government Medical College, Kottayam, Kerala, India.
E-mail: drsureshbhat@yahoo.com
Percutaneous Nephrolithotomy (PCNL) is a common endourologic procedure done for removal of renal stones. The most important initial step involves making a safe puncture into the pelvicalyceal system, and establishing an access tract into pelvicalyceal system. This is a crucial step in the success of the PCNL. Though the procedure is relatively simple and straight forward, in conditions like hyper-mobile kidney or ptotic kidney, the pelvicalyceal system is abnormally oriented and the kidneys are excessively mobile making the puncture of pelvicalyceal system difficult. Till date there is no established technique to overcome this problem. The technique of resolving this problem involved placing an air filled urobag beneath the patient in the prone position on the ipsilateral side of abdomen. This technique of placing an inflated urobag called as “The inflated urobag” technique is a simple one, which relocates the kidney and hence the pelvicalyceal system to normal anatomical position, making the initial puncture easier. This also prevents excessive mobility of the kidney during puncture and dilatation of the tract. This technique, which is not described earlier, is extremely useful in the puncture and dilatation during prone PCNL in ptotic and hyper-mobile kidneys. We here in describe our experience in 15 cases of PCNL in ptotic or hypermobile kidney.
Hypermobile kidney, Lithotripsy, Percutaneous renal access, Urine collection bag
Case Series
Percutaneous Nephrolithotomy (PCNL) is the most common procedure performed for the treatment of large renal stones. It involves puncturing the desired calyx of kidney and dilating the tract under fluoroscopic guidance. Later with help of nephroscope the stones are visualized and broken by lithotripsy device. Thus the fragments are removed. The initial step in PCNL is crucial which involves a proper puncture in to the pelvicalyceal system into the desired calyx with an 18 gauge puncture needle. The puncture is very much difficult in situations like hypermobile kidney or ptotic kidney since the kidney moves away from the puncturing needle. We here in report our experience in overcoming this problem in 15 cases of hypermobile kidney.
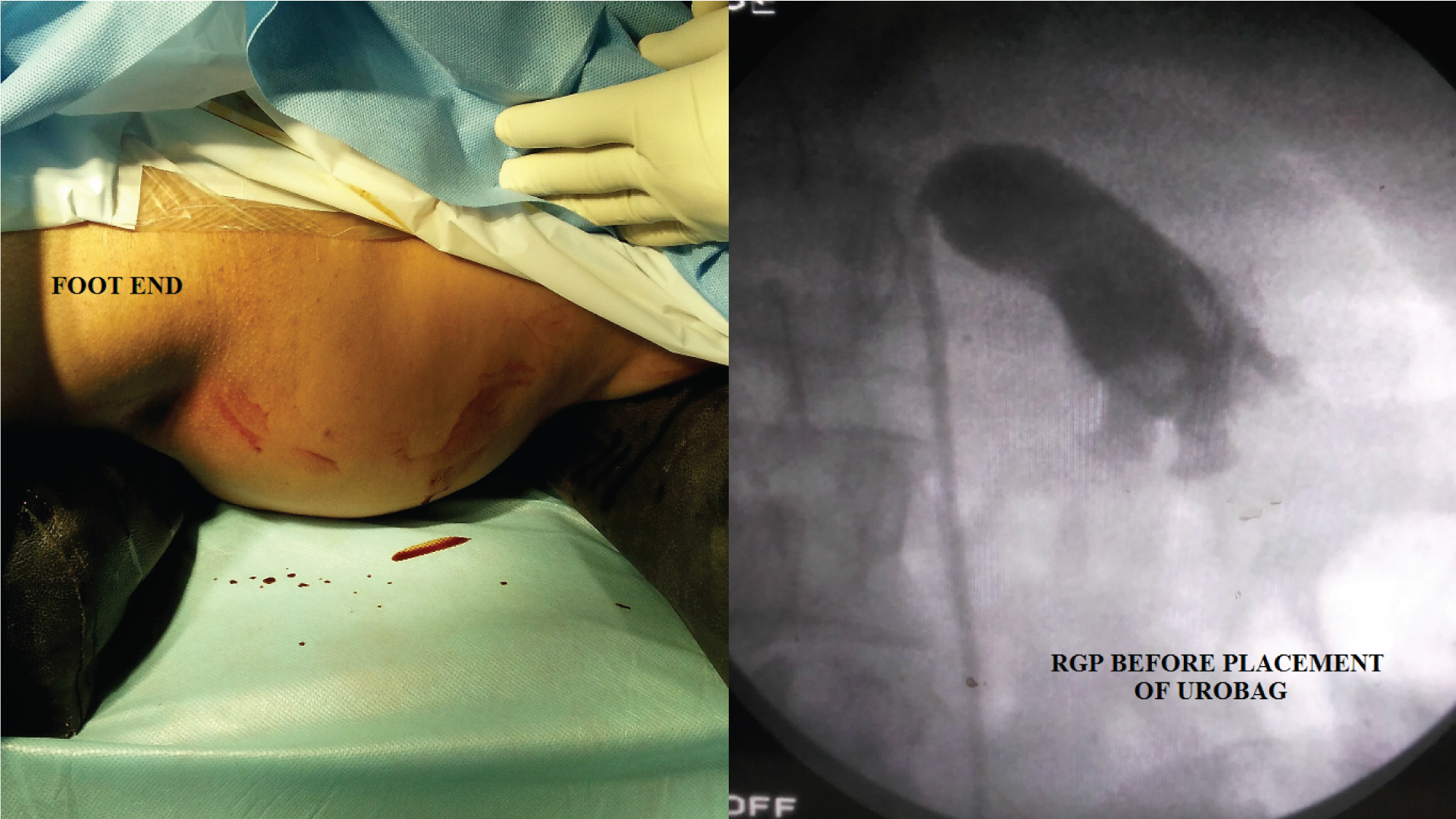
The study was done in a tertiary care centre where PCNL is done on a regular basis. The study was a prospective observational study. The study was carried out from January 2015 to December 2016. The patients who were found to have ptotic kidney in prone position during PCNL were included [Table/Fig-1]. A total of 15 cases were included.
Patient in prone PCNL with bolsters over chest and pelvis (left). Retrograde pyelography before PCNL puncture showing abnormally drooping right kidney with superimposition of calyces over pelvis (right).
Technique
The team of urologists who performed the PCNL has a cumulative experience of having done more than 3000 cases. The procedure was done under general anaesthesia. After the standard preparation and ureteric catheterization, the patient was turned prone and the bolsters kept horizontally beneath the chest and pelvis [Table/Fig-1]. These bolsters were placed to facilitate ventilation in prone position under general anaesthesia. Retrograde pyelography was done subsequently. If the kidney appeared drooped down and angulated acutely to the ureter [Table/Fig-1], an air filled urine collection bag was placed under the ipsilateral abdomen [Table/Fig-2]. This displaced the kidney to its normal position and orientation making the pelvicaliceal system punctures and dilatation fairly straight forward [Table/Fig-2]. This also fixed the kidney there by, preventing further movement during dilatation. In all the 15 cases, the kidney was found to be ptotic and hypermobile. Thus, after placing the air filled urobag the puncture and dilatation became easy without any problem. All the 15 patients had successful dilation of tract and removal of stones. One of the cases using the above explained Urobag technique is illustrated in [Table/Fig-1,2]. [Table/Fig-3] shows similar case in which the above technique was used.
Air filled urobag placed under the ipsilateral abdomen (left). Retrograde pyelography after placement of air filled urobag showing the kidney in normal position. This makes the puncture easier.
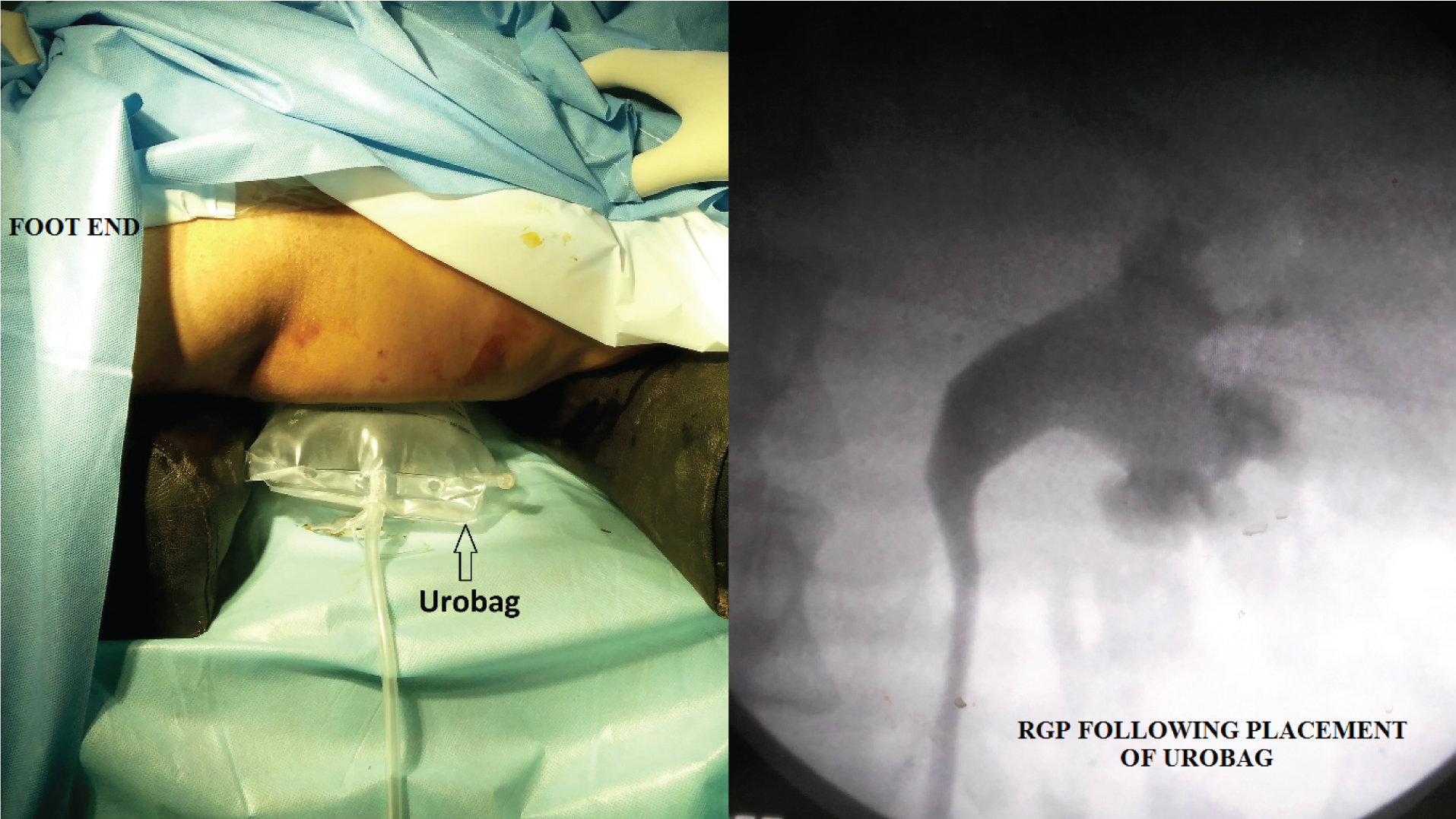
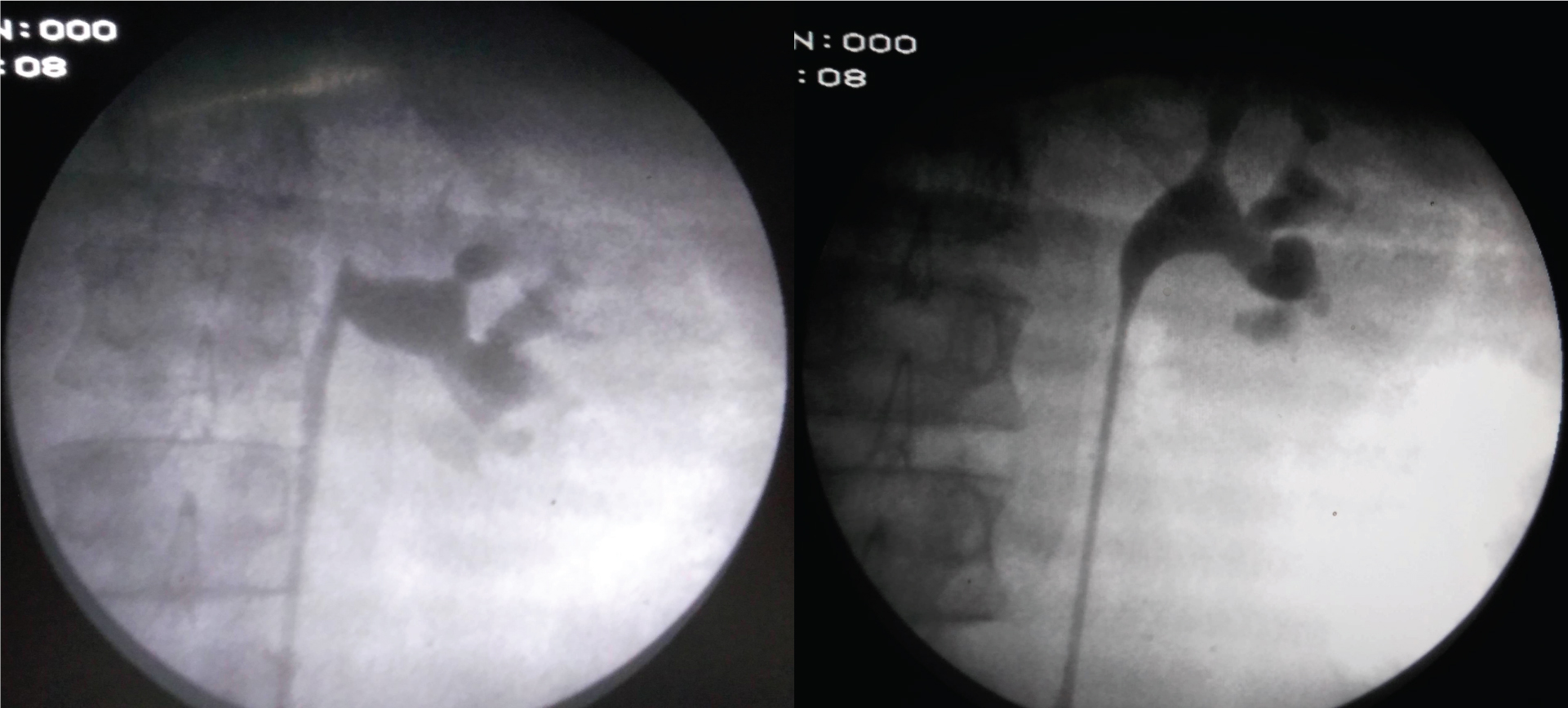
Illustration of another case showing retrograde pyelography of patient during PCNL in prone position. Figure shows ptotic kidney with abnormal orientation of pelvicalyceal system (left). Retrograde pyelography after placement of inflated Urobag showing normal position and orientation of kidney, making the puncture into desired calyx much easier (right).
Discussion
PCNL is the most common minimally invasive procedure performed for removal of renal calculi. Fernstrom and Johansson (1976), reported the removal of renal calculus through a nephrostomy tract for the first time [1]. It is done either in prone or supine position, prone position being most commonly used [2]. The procedure involves making a puncture into the pelvicalyceal system and establishing a tract under fluoroscopic or ultrasound guidance. Once entry into the Pelvicalyceal System (PCS) has been established, stones are usually broken by ballistic or laser lithotripter and the fragments are removed [3]. This procedure is not devoid of complications, with haemorrhage from the kidney being the most important and dreaded complication. Other complications like adjacent organ injuries, residual fragments and sepsis also do occur [4].
Making a safe puncture and establishing an access into pelvicalyceal system is a crucial initial step in the success of the PCNL [5]. In most cases the puncture is fairly straight forward provided, the pelvicalyceal anatomy is normal. Some conditions make PCNL puncture difficult and challenging. These include stones in ptotic kidney, hyper-mobile kidney, calyceal diverticulum, horseshoe or pelvic kidney and morbidly obese patients [6].
Nephroptosis or ptotic kidney is an uncommon situation where in, the kidney descends down more than 5 cm during position change from supine to upright position [7]. This ptosis also has been seen during change of position from supine to prone position which occurs during prone PCNL. The term nephroptosis was first coined by Glenard in 1885 [8]. However hyper-mobile kidney was first described in the literature by Franciscus de Pedemontanus in the 13th century [9]. In literature the term ptotic kidney and hypermobile kidney are loosely used.
Ptotic kidney is usually asymptomatic and goes unnoticed. They are detected on intravenous urography taken for some other indications. Only about 10-20% of ptotic kidneys is symptomatic and requires surgical treatment [10].
In prone PCNL, the PCS of the kidney to be punctured is delineated by injecting Urograffin 76% contrast agent (sodium amidotrizoate and meglumine diatrizoate mixture) [11]. In ptotic and hyper mobile kidneys, the anatomic orientation of the kidney and the PCS is altered. The PCS is seen to be drooping downwards. The calyces are sometimes superimposed [Table/Fig-1]. Since the kidney is unusually hyper mobile, it moves away from the needle making puncture and dilatation difficult. The tract becomes abnormally longer leading to kinking of the guide wire. In our experience we have encountered ptotic and hyper-mobile kidney in prone PCNL in 15 cases. We overcame this difficulty by placing an inflated urobag underneath the ipsilateral abdomen as shown in [Table/Fig-2].
In literature there is no established technique to overcome this difficulty. Lezrek et al., described a useful technique for puncture and dilatation in abnormally mobile kidneys using bi-prong forceps dissection [12]. In this technique, after initial puncture the authors used bi-prong forceps for dissection of renal parenchyma and entry into pelvicaliceal system. Rais-Bahrami et al., used Foleys catheter balloon for pinning the kidney to the lateral abdominal wall in hypermobile kidneys [6]. In this technique, initial entry into the PCS was made in a calyx away from the calyx intended for nephrolithotomy. Through this calyx, Foley catheter was introduced and balloon inflated and pulled outwards under fluoroscopic guidance for fixing the kidney. In our opinion, when compared to both the above techniques by Lezrek et al., and Rais-Bahrami et al., our technique is simple in that no extra tract is required to fix the kidney there by avoiding unnecessary morbidity. This modification and innovation is simple, non invasive, straight forward and cost effective with no extra morbidity. To our knowledge this technique has not been described so far in prone PCNL.
Conclusion
Placement of an air filled urine collection bag beneath the abdomen of patients in the prone position during PCNL in a ptotic/hypermobile kidney is a simple and useful maneuver. This method helps in correcting the abnormal position and mobility of kidney during puncture of pelvicalyceal system thus facilitating puncture and dilatation.
[1]. Fernstrom I, Johansson B, Percutaneous pyelolithotomy. A new extraction techniqueScand J Urol Nephrol 1976 10:257-59. [Google Scholar]
[2]. Beiko D, Supine versus prone PCNL: The debate continuesCanadian Urological Association Journal 2011 5(4):266-67. [Google Scholar]
[3]. Cho C, Yu JH, Sung LH, Chung JY, Noh CH, Comparison of percutaneous nephrolithotomy using pneumatic lithotripsy (lithoclast®) alone or in combination with ultrasonic lithotripsyKorean Journal of Urology 2010 51(11):783-87. [Google Scholar]
[4]. Kyriazis I, Panagopoulos V, Kallidonis P, Ozsoy M, Vasilas M, Liatsikos E, Complications in percutaneous nephrolithotomyWorld J Urol 2014 33(8):1069-77. [Google Scholar]
[5]. Sharma GR, Maheshwari PN, Sharma AG, Maheshwari RP, Heda RS, Maheshwari SP, Fluoroscopy guided percutaneous renal access in prone positionWorld Journal of Clinical Cases: WJCC 2015 3(3):245-64. [Google Scholar]
[6]. Rais-Bahrami S, Friedlander JI, Duty BD, Okeke Z, Smith AD, Difficulties with access in percutaneous renal surgeryTherapeutic Advances in Urology 2011 3(2):59-68. [Google Scholar]
[7]. Murari SB, Gadepalli T, Rao VP, Ram R, Renal scintigraphy in diagnosis and management of nephroptosisIndian Journal of Nuclear Medicine 2012 27(1):52-54. [Google Scholar]
[8]. Barber NJ, Thompson PM, Nephroptosis and nephropexy--hung up on the past?Eur Urol 2004 46(4):428-33. [Google Scholar]
[9]. Hoenig DM, Hemal AK, Shalhav AL, Clayman RV, Nephroptosis: A "disparaged" condition revisitedUrology 1999 54(4):590-96. [Google Scholar]
[10]. Srirangam SJ, Pollard AJ, Adeyoju AAB, O’Reilly PH, Nephroptosis: seriously misunderstood?BJU International 2009 103:296-300. [Google Scholar]
[11]. Monga M, Rane A, Chapter 9. Instrumentation and Surgical TechniquePercutaneous Renal Surgery 2014 1st edOxfordJohn Wiley and Sons, Ltd:84-94. [Google Scholar]
[12]. Lezrek M, Bazine K, Asseban M, Ammani A, Moufid K, Beddouch A, Technique to overcome renal mobility during percutaneous tract dilatation: bi-prong forceps renal parenchyma dissectionBJU Int 2013 112:697-702. [Google Scholar]