Surgical Removal of Fractured Endodontic Instrument Extending Beyond the Periapex of Mesiobuccal Root of Maxillary Second Molar through the Maxillary Sinus
Kiezhekke Veedu Sheethi1, Kitu Sheoran2, Thakur Veerandar Singh3
1 Senior Lecturer, Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India.
2 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India.
3 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kiezhekke Veedu Sheethi, Senior Lecturer, Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad-501101, Telangana, India.
E-mail: sheethi11@gmail.com
Procedural accidents during endodontic treatment often complicate the overall treatment plan of the patient. One of the most frequently encountered procedural accidents is fracture of endodontic instrument. Removal of fractured instrument from root canal is often a difficult procedure especially, when the fractured instrument extends beyond apex. This case report presents the management of a case involving the surgical removal of a broken endodontic file from the periapical region of the mesiobuccal root of a maxillary second molar.
Fractured endodontic instrument, Maxillary second molar, Maxillary sinus mesiobuccal root, Periapical surgery
Case Report
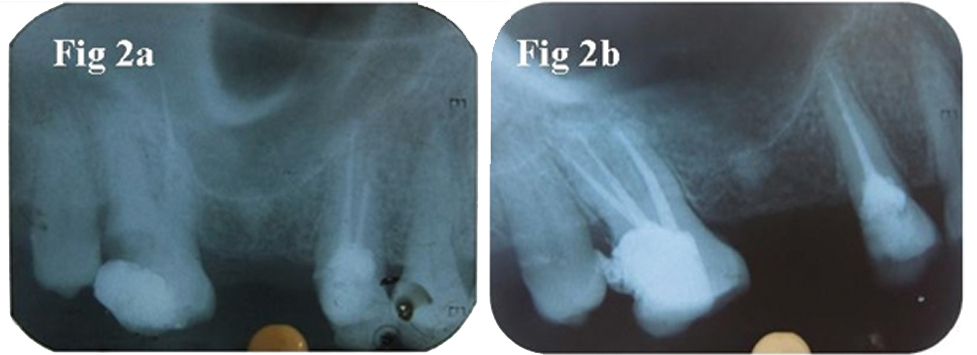
A 45-year-old female patient reported to Army College of Dental Sciences, Secunderabad, Telangana with a chief complaint of dull intermittent pain in her right upper back tooth. Patient gave a history of root canal treatment which was initiated about 3 months back. Clinical examination was done which showed the presence of class II cavity (disto-occlusal) in relation to maxillary right second molar [Table/Fig-1a]. There was associated Grade I tooth mobility but no presence of any gingival inflammation. Maxillary first molar was missing and maxillary second premolar was root canal treated. On radiographic examination, it was revealed that there was the presence of a fractured endodontic file near the apex of the mesiobuccal root of maxillary second molar [Table/Fig-2a]. The fractured fragment was 6 mm long, of which 1 mm was into the mesiobuccal root apex and 5 mm was penetrating into the maxillary sinus. The decision was made to retrieve the fragment.
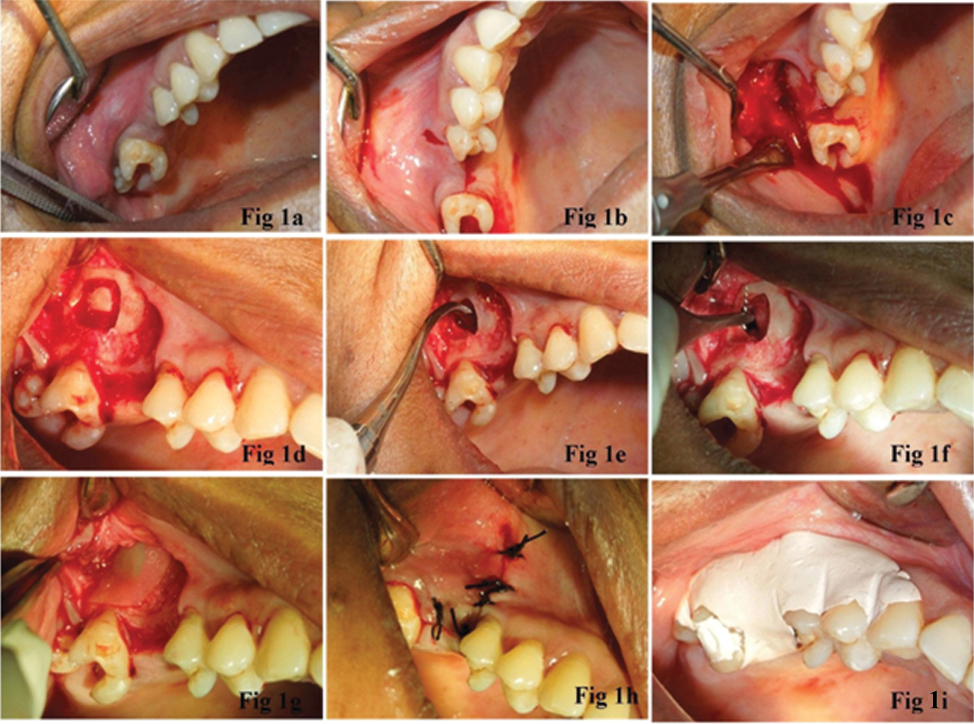
a) Preoperative photograph, b) Mid crestal incison followed by vertical incison, c) Flap reflection, d) Lateral window preparation to gain access to mesiobuccal root apex, e) Elevation of sinus membrane f) Fractured instrument retrieval using Adsons tissue holding forceps, g) GTR membrane placement over window preparation, h) Suture placement, i) Placement of protective periodontal pack.
a) Preoperative rdiograph showing fractured instrument external beyond apex of mesiobuccal root of maxillary second molar, b) Postoperative radiograph during follow up.
The area of interest was anesthetized. A mid crestal incision was made at the maxillary first molar region which was extended into the gingival sulcus of maxillary second molar buccally. A vertical incision was also given at the distobuccal line angle of maxillary second premolar, extending beyond the mucogingival junction [Table/Fig-1b]. Flap was adequately reflected to obtain good access [Table/Fig-1c].
A lateral window was made for gaining access to the mesiobuccal root apex. Through radiographic findings, the apex was determined to be 9mm from the bone margin. Hence, the lateral window was made with that distance as the center using a round carbide drill [Table/Fig-1d]. A paintbrush stroke was used to outline the lateral window until a bluish hue was observed. The bone of the lateral access window was gently removed. The sinus membrane was gently lifted off the antral walls using sinus membrane elevators (Salvin sinus kit) [Table/Fig-1e]. The fractured fragment was firmly embedded in the mesiobuccal root apex. The sinus membrane, which was penetrated by the instrument, was carefully lifted over root apex in which the fragment was embedded. The retrograde removal of fractured instrument was successfully achieved using Adsons tissue forceps. As major portion of the broken instrument was beyond the root apex it could be easily removed using forceps only [Table/Fig-1f].
A Guided tissue regeneration (GTR) membrane (Healiguide, Advanced Biotech Products Ltd., Alathur, India) was placed over the lateral sinus window to provide a barrier to epithelisation at the site [Table/Fig-1g]. The flap was sutured [Table/Fig-1h]. A protective periodontal pack (Coe-Pak, GC America Inc) was placed over the site to avoid discomfort to the patient and to avoid any post-operative contamination [Table/Fig-1i]. A temporary restoration was done in relation to maxillary right second molar. Postoperative instructions were given which included rest, ice, pressure and elevation of the head. Patient was also asked not to blow the nose or create negative pressure while sucking through a straw. Patient was asked to cough with the mouth open, if it occurred, to relieve the pressure within the sinus.
When suture removal was done after 10 days, gingival healing was found to be good with no bleeding from the site and only mild inflammation. After the follow up period of two weeks, cleaning and shaping of the canals was done with Protaper rotary files (Dentsply) followed by obturation with respective guttapercha points (Dentsply). Clinical and radiographic evaluation [Table/Fig-2b] was done after 4 weeks and patient was found to be asymptomatic.
Discussion
Unforeseen circumstances like procedural accidents are unavoidable and are often encountered during endodontic treatment. Most frequently encountered endodontic mishap is fracture of endodontic instrument. The risk of fracture of endodontic instrument increases in complicated root canal morphology. Apical third carries a higher risk of instrument fracture as compared to coronal and middle third [1,2]. Retrieval of fractured fragment from apical third mostly requires an apicoectomy procedure. Whenever the fractured fragment extends beyond the apex, it is imperative to retrieve the fragment. Hence, in such cases, retrograde removal is attempted [3]. However, various anatomic landmarks have to be carefully considered during retrieval in such cases. Literature reveals previous case reports where the fractured instrument is removed surgically from the periapex in mandibular teeth through various approaches [4,5]. Retrieval of the fractured fragment from the root apex of maxillary molars is difficult due to proximity to maxillary sinus.
In the present case, we have described the management of a patient with fractured endodontic instrument beyond apex of mesiobuccal root of maxillary second molar through maxillary sinus. An endodontic procedural error led to instrument fracture at the apex of mesiobuccal root of maxillary second molar. This caused low grade periapical inflammation leading to dull constant pain in the patient. It was imperative to retrieve the fractured fragment as it had perforated the sinus membrane to reach the sinus. The retrieval of fragment was achieved by gentle lifting of the sinus membrane. As the perforation was only a pinpoint perforation by the instrument so no membrane perforation repair was considered necessary.
It is essential to have the knowledge of anatomical and clinical significance of surrounding structures like maxillary sinus or inferior alveolar canal and its implications in endodontic treatment. Management of the procedural error is not a simple task but can be achieved if the correct treatment plan is laid out.
[1]. Iqbal MK, Kohli MR, Kim JS, A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: A PennEndo database studyJ Endod 2006 32(11):1048-52. [Google Scholar]
[2]. Hülsmann M, Schinkel I, Influence of several factors on the success or failure of removal of fractured instruments from the root canalEndod Dent Traumatol 1999 15(6):252-58. [Google Scholar]
[3]. Yeo JF, Loh FC, Retrograde removal of fractured endodontic instrumentsAnn Acad Med Singapore 1989 18(5):594-98. [Google Scholar]
[4]. Gandevivala A, Parekh B, Poplai G, Sayed A, Surgical Removal of Fractured Endodontic Instrument in the Periapex of Mandibular First MolarJ Int Oral Health 2014 6(4):85-88. [Google Scholar]
[5]. Shenoy A, Mandava P, Bolla N, Vemuri S, A novel technique for removal of broken instrument from root canal in mandibular second molarIndian J Dent Res 2014 25:107-10. [Google Scholar]