Delayed Repair of Infected Ruptured Patellar Tendon using Suture Anchors
Himanshu Kataria1, Lakshay Goel2, Sahil Gaba3, Jatin Prakash4, Arvind Kumar5
1 Professor and Head, Department of Orthopaedics, Sports Injury Centre, New Delhi, India.
2 Postgraduate Student, Department of Orthopaedics, Lady Hardinge Medical College, New Delhi, India.
3 Senior Resident, Department of Orthopaedics, All India Institute of Medical Sciences, Chandigarh, India.
4 Associate Professor, Department of Orthopaedics, Sports Injury Centre, New Delhi, India.
5 Senior Resident, Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sahil Gaba, House Number 165, Sector 33 A, Chandigarh-160020, India.
E-mail: drsahilgaba@gmail.com
Patellar tendon rupture are rare injuries that are easily missed in acute phases if careful clinical examination is not carried out. The delayed condition is further difficult to treat and augmentation of end to end repair is generally required. However, literature presents no such case of delayed presentation with presence of infection. We here present one such case of delayed presentation of patellar tendon rupture at three weeks in a 52-year-old male patient. Usual techniques were not sufficient to allow early rehabilitation. Technique of suture anchors was planned for repair after thorough debridement. After this intervention, patient was put on aggressive rehabilitation protocol and he gained excellent range of motion. Patient was followed for one year and he showed no loss of movement or signs of infection. We thus recommend using anchor suture repair of patellar tendon that provides a stable and rigid fixation with possibility of early active rehabilitation even in delayed setting.
Tendon injury, Patellar ligament, Rupture, Knee injury
Case Report
A 52-year-old male patient presented to Out Patient Department three weeks after a road traffic accident wherein he suffered a glass cut injury over the right knee region. The patient was initially managed at another center with wound closure, antibiotics and cylinder slab. When slab was removed at three weeks, patient noticed inability to actively extend the knee and had overlying infection.
On examination, there was a 4 x 2 cm lacerated wound with purulent discharge near the inferior pole of patella. Knee movements were painful and patient was unable to actively extend the knee.
Wound culture revealed Methicillin Sensitive Staphylococcus aureus (MSSA). Radiographs of right knee showed an abnormal soft tissue shadow of patellar tendon and MRI right knee revealed ruptured patellar tendon with antero-superior displacement of patella [Table/Fig-1].
MRI right knee (sagittal section) showing ruptured patellar tendon with antero-superior displacement of patella.
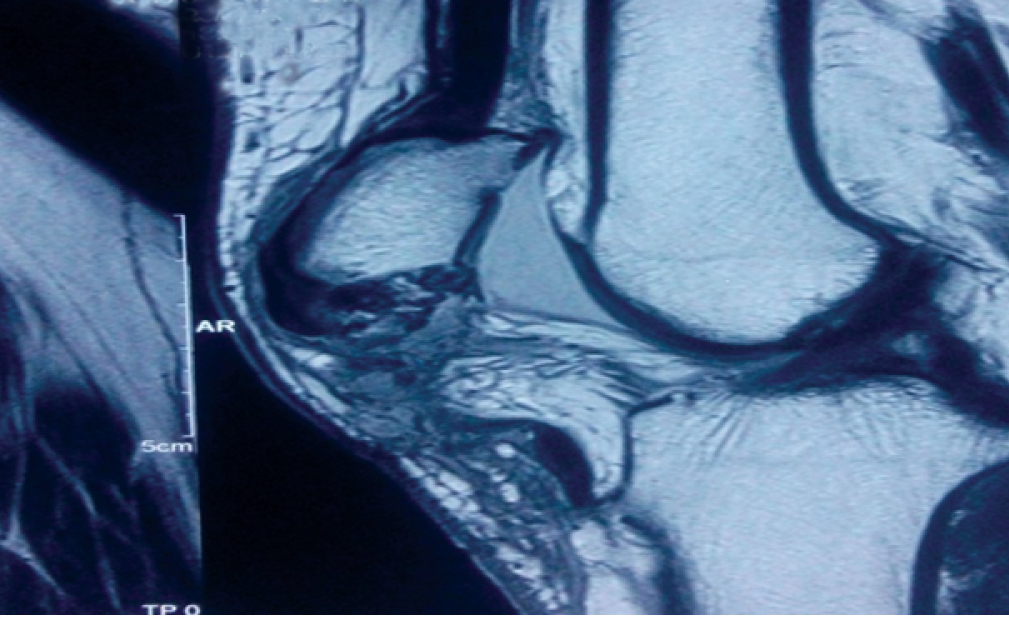
However, no intra-articular collection was seen. In presence of infection, the case presented a surgical dilemma. Due to the presence of infection, a staged management protocol was undertaken with initial debridement and later repair. However, usual treatment with end to end repair and encircle wire through patella and tibial tuberosity was difficult in the presence of infection. The ends of tendon were expected to be friable, which precluded end to end repair. Using wires for encerclage could have led to a resurgence of infection and also delay the rehabilitation. Thorough debridement of wound was done and intravenous antibiotics were administered. The infection subsided within the next few days. Five days later definitive repair was undertaken. A repair using suture anchors was planned.
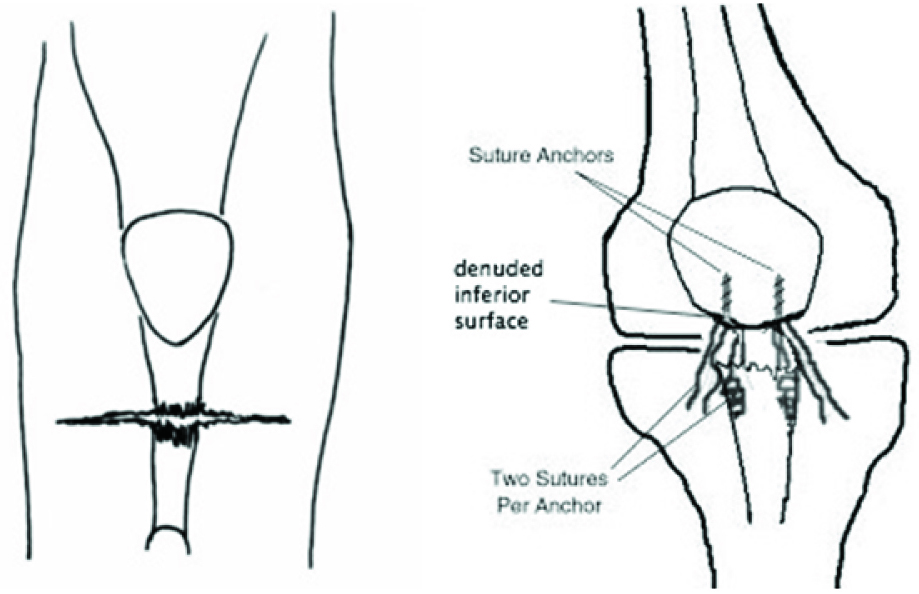
The lacerated wound was extended both proximally and distally and site of rupture and distal stump of patellar tendon were identified. Inferior pole of patella was denuded and freshened, and two double loaded suture anchors (locally manufactured; 4.0 mm) were inserted into patella. Krackow sutures were passed through distal end, tied to suture anchors [Table/Fig-2].
Diagrammatic representation showing two suture anchors in patella and suture threads passed (Krackow technique) through patellar tendon.
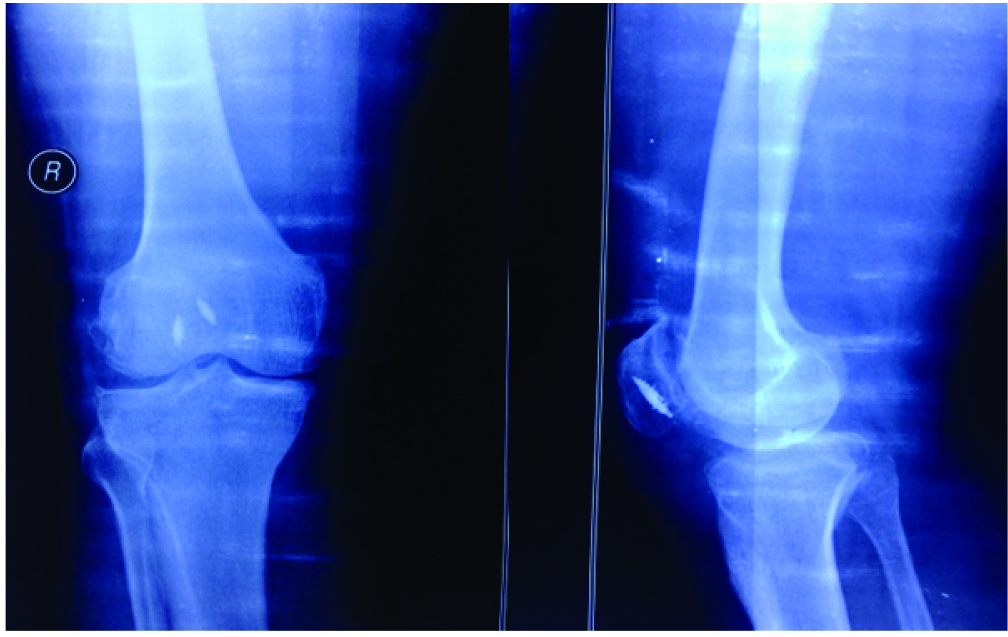
Intraoperatively, flexion to around 90 degrees was done to assess integrity of repair. Further flexion was not done due to fear of sutures giving way. Grossly the tendon appeared healthy without any sign of tendinopathy or degeneration. The retinaculum was repaired and skin was closed. Postoperative radiographs showed optimal positioning of the anchors [Table/Fig-3].
Postoperative anteroposterior and lateral radiographs showing placement of anchors in inferior half of patella.
A knee brace locked in extension was given in postoperative period for two week and patient was encouraged to do isometric knee exercises from first postoperative day.
After two weeks, sutures were removed and patient was given range of motion brace and allowed 0-90 degree of motion. Weight bearing was allowed with brace locked in extension. Range of motion was increased to 120 degrees at the end of six weeks. The rehabilitation protocol was maintained till three months post-surgery. Patient was followed for one year.
At final follow-up of one year, there was no extensor lag with range of motion 0-120 degree. Patient was able to squat and had reached his pre-injury work capacity. There was no evidence of infection in postoperative period [Table/Fig-4].
Clinical pictures showing healed wound and acceptable range of motion of knee.

Discussion
Although, it is the third most common cause of extensor mechanism injury after patella fracture and quadriceps rupture, still patellar tendon rupture is a rare occurrence [1]. The ruptures are usually confined to the inferior pole of patella at the bone-tendon junction, and it is not uncommon to miss these injuries during preliminary examination. A retrospective series by Siwek CW and Rao JP found that 27% of patellar tendon ruptures were chronic [2]. Most reports share some common features–patients younger than 40 years, rupture mostly at inferior pole of patella and management by end to end suture with additional cerclage wiring to fix the knee in extension during healing phase [3–5]. This case of a 52-year-old male presented to us with a missed patellar tendon rupture of three weeks duration with an infected overlying wound. The case depicted a surgical dilemma as the overlying infection and delayed presentation made usual method of treatment difficult.
Patellar tendon is a ligament connecting inferior pole of patella to tibial tubercle [6]. Acute ruptures have classically been described to occur at osseotendinous junction causing a complete derangement of knee extensor mechanism [1–4]. If the tendon does not heal at the correct length and tension, knee range of motion and strength can be altered significantly, leading to early fatigue, patellofemoral pain, and instability [7].
Unilateral traumatic patellar tendon ruptures occur as a result of sudden violent quadriceps contraction in resisted flexed knee and are estimated to require a force close to 17.5 times the body weight [8]. Given the considerable force needed to rupture a healthy tendon, it is likely that ruptures occur in areas of pre-existing disease and tendon weakening. Repetitive microtrauma or a systemic condition may precede the actual disruption. In our case there was no history of any previous pain in patellar region nor did MRI suggested any degeneration in tendon.
Owing to the debilitating nature of rupture, an acute repair with end to end suture has been suggested in the past. It was frequently weak and augmentation was often required. Cerclage wires or autografts have been tried in past with good results [3]. However, due to risk of infection and prolonged immobilization of above techniques, we preferred a more stable fixation using suture anchors. Use of this technique in ruptures three to four week-old has not been described. Furthermore, end-to-end suture with cerclage wiring requires a six weeks postoperative cast in full extension for tendon healing. On the contrary, early movement can be started with suture anchors by two to three weeks. Other literature have also shown that active rehabilitation has good results with no deleterious effect on tendon healing [9].
Suture anchors have also been proven to be biomechanically superior to transosseous sutures [10], and their use has been shown to yield good results [11].
The main surgical concern is to prevent patella alta and to bring down the high ridden patella during surgery [6,12]. Authors have described pre-operative patellar traction for this problem. Also, intraoperatively sectioning of patellar retinaculum and supra-patellar bursa by arthrolysis may help to bring patella distally. Failing this, the proximal tendon of the rectus femoris can be sectioned, through a Hueter approach, to provide additional release [6]. However, in our case patella was not grossly over-ridden probably because the knee was immobilized in full extension for three weeks and no muscle strengthening exercises were performed
The usual technique of patellar tendon to bone repair involves drilling trans osseous tunnels and passing non-absorbable sutures via beath pins and then finally tying the sutures after taking multiple bites in the patellar tendon. However, disadvantages include penetration of articular cartilage by beath pins, drilling oblique tunnels which can cause patellar tilting and alter the direction of force vectors, and risk of tunnel loosening [13]. The use of suture anchors can help circumvent all these problems while providing a strong fixation utilizing the Krackow technique. [Table/Fig-5] summarizes the details of previous studies which have used a similar technique. All previous reports have been in acute ruptures [8,9,13-15]. Our report is the first description of this technique in chronic infected tear.
A list of previous studies which have used a similar technique.
| S. No. | Author (Year of study) | No. of cases | Method | Outcome | Follow-up |
|---|
| 1 | Ho HM et al., [8] | 1 (bilateral rupture) | 2 suture anchors | Excellent | 2 years |
| 4 | Gaines RJ et al., [9] | 4 | 2 suture anchors | Excellent | 6 Months |
| 3 | Capiola D et al., [13] | 2 | 3 suture anchors | Excellent | 3 Months |
| 2 | Bushnell BD et al., [14] | Biomechanical study on six pairs of cadaveric knees | 2 suture anchors vs Trans-patellar tunnel suture repair | No difference in load to failure. Hence both are equally strong constructs. | |
| 5 | Kim JR et al., [15] | 1 (bilateral rupture in a pre-adolescent child) | 2 suture anchors | Excellent | 1 year |
Conclusion
Anchor suture repair of patellar tendon provides a stable and rigid fixation with possibility of early active rehabilitation. The method can be tried even for delayed repairs up till three weeks.
[1]. Lewis PB, Rue J-P, Bach BR, Chronic patellar tendon rupture: surgical reconstruction technique using 2 Achilles tendon allograftsJ Knee Surg 2008 21(2):130-35. [Google Scholar]
[2]. Siwek CW, Rao JP, Ruptures of the extensor mechanism of the knee jointJ Bone Joint Surg Am 1981 63(6):932-37. [Google Scholar]
[3]. Jabłoński JJ, Jarmuziewicz P, Drużbicki M, Reconstruction of chronic patellar tendon rupture with semitendinosus tendon: case reportOrtop Traumatol Rehabil 2011 13(6):607-15. [Google Scholar]
[4]. Krackow KA, Thomas SC, Jones LC, A new stitch for ligament-tendon fixation. Brief noteJ Bone Joint Surg Am 1986 68(5):764-66. [Google Scholar]
[5]. Marder RA, Timmerman LA, Primary repair of patellar tendon rupture without augmentationAm J Sports Med 1999 27(3):304-07. [Google Scholar]
[6]. Milankov MZ, Miljkovic N, Stankovic M, Reconstruction of chronic patellar tendon rupture with contralateral BTB autograft: a case reportKnee Surg Sports Traumatol Arthrosc 2007 15(12):1445-48. [Google Scholar]
[7]. Andarawis-Puri N, Sereysky JB, Sun HB, Jepsen KJ, Flatow EL, Molecular response of the patellar tendon to fatigue loading explained in the context of the initial induced damage and number of fatigue loading cyclesJ Orthop Res 2012 30(8):1327-34. [Google Scholar]
[8]. Ho HM, Lee W-KE, Traumatic bilateral concurrent patellar tendon rupture: an alternative fixation methodKnee Surg Sports Traumatol Arthrosc 2003 11(2):105-11. [Google Scholar]
[9]. Gaines RJ, Grabill SE, DeMaio M, Carr D, Patellar tendon repair with suture anchors using a combined suture technique of a Krackow-Bunnell weaveJ Orthop Trauma 2009 23(1):68-71. [Google Scholar]
[10]. Petri M, Dratzidis A, Brand S, Calliess T, Hurschler C, Krettek C, Suture anchor repair yields better biomechanical properties than transosseous sutures in ruptured quadriceps tendonsKnee Surg Sports Traumatol Arthrosc 2015 23(4):1039-45. [Google Scholar]
[11]. Bushnell BD, Whitener GB, Rubright JH, Creighton RA, Logel KJ, Wood ML, The use of suture anchors to repair the ruptured quadriceps tendonJ Orthop Trauma 2007 21(6):407-13. [Google Scholar]
[12]. Falconiero RP, Pallis MP, Chronic rupture of a patellar tendon: a technique for reconstruction with Achilles allograftArthroscopy 1996 12(5):623-26. [Google Scholar]
[13]. Capiola D, Re L, Repair of patellar tendon rupture with suture anchorsArthroscopy 2007 23(8):906.e1-4. [Google Scholar]
[14]. Bushnell BD, Byram IR, Weinhold PS, Creighton RA, The use of suture anchors in repair of the ruptured patellar tendon: a biomechanical studyAm J Sports Med 2006 34(9):1492-99. [Google Scholar]
[15]. Kim JR, Park H, Roh S-G, Shin SJ, Concurrent bilateral patellar tendon rupture in a preadolescent athlete: a case report and review of the literatureJ Pediatr Orthop B 2010 19(6):511-14. [Google Scholar]