Spindle Cell Liposarcoma – A Rare Tumour Occurring at a Rare Site?
Varuna Mallya1, Nita Khurana2, N.S. Hadke3
1 Assistant Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
2 Director Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
3 Director Professor, Department of Surgery, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Varuna Mallya, Assistant Professor, Department of Pathology, Room No-269, Maulana Azad Medical College, New Delhi-110002, India.
E-mail: varunamallya@gmail.com
Lipomatous tumours are the most common type of soft tissue neoplasms with liposarcomas being the most common soft tissue sarcomas. Spindle cell liposarcoma is the most recent addition to this group and is characterized by a lipocytic and spindled component both showing atypia. Lipoblasts with their characteristic scalloped nuclei are found in the spindled areas. These tumours show CD34 positivity. Arising in the head and neck and soft tissues of the extremities, this tumour was described for the first time in 1994. Very few cases are reported in the literature. The present case emphasizes the fact that this tumour should be considered as a possible diagnosis in tissues histologically showing a good admixture of adipocytic and spindled cells.
Adipocytes, Lipoma, Neoplasm recurrence, Sarcoma
Case Report
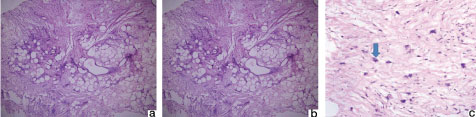
A 23-year-old lady came to the surgical OPD with a painless swelling on the dorsum on the foot since a year. On clinical examination it was a non tender, freely mobile, subcutaneous swelling that was not fixed to the overlying skin and measured 3 x 3 cm. The overlying skin was normal. A clinical diagnosis of lipoma was given; the lesion was excised and sent for histopathology in 10% formalin. Grossly, the resected specimen measured 3 x 3 cm, was well circumscribed and oval. The cut section was grey white, firm with some gelatinous areas [Table/Fig-1]. The specimen was processed and Haematoxylin and Eosin (H&E) stained sections were examined. On microscopy, the tumour was composed of adipocytic and spindle cell components [Table/Fig-2a]. The adipocytic component showed variation in cell size. The spindled component exhibited bizarre stromal cells, multivacuolated lipoblasts with scalloped nuclei [Table/Fig-2b], and multinucleated giant cells arranged in a “floret like pattern” [Table/Fig-2c]. Few thin walled vessels were seen. The spindled component was associated with thick ropy collagen bundles present in a myxoid background. There were no areas of haemorrhage or necrosis. Based on the clinical and histological features a diagnosis of atypical lipomatous tumour was made. Sections were selected for Immunohistochemistry (IHC). On IHC, the spindled cells and lipoblasts were positive for CD34 [Table/Fig-3] and benign adipocytes were faintly positive for S100. Based on the histopathology and IHC a diagnosis of spindle cell liposarcoma was made. The patient was disease free after two months of excision.
Gross image showing a firm, white and gelatinous lesion.

a) Photomicrograph showing admixed spindled and adipocytic areas (H and E, 10X); b) Photomicrograph showing a lipoblast with scalloped nucleus (Arrow) (H and E, X400); c) Photomicrograph showing multinucleated giant cells arranged in a floret like pattern (Arrow) (H&E, X100).
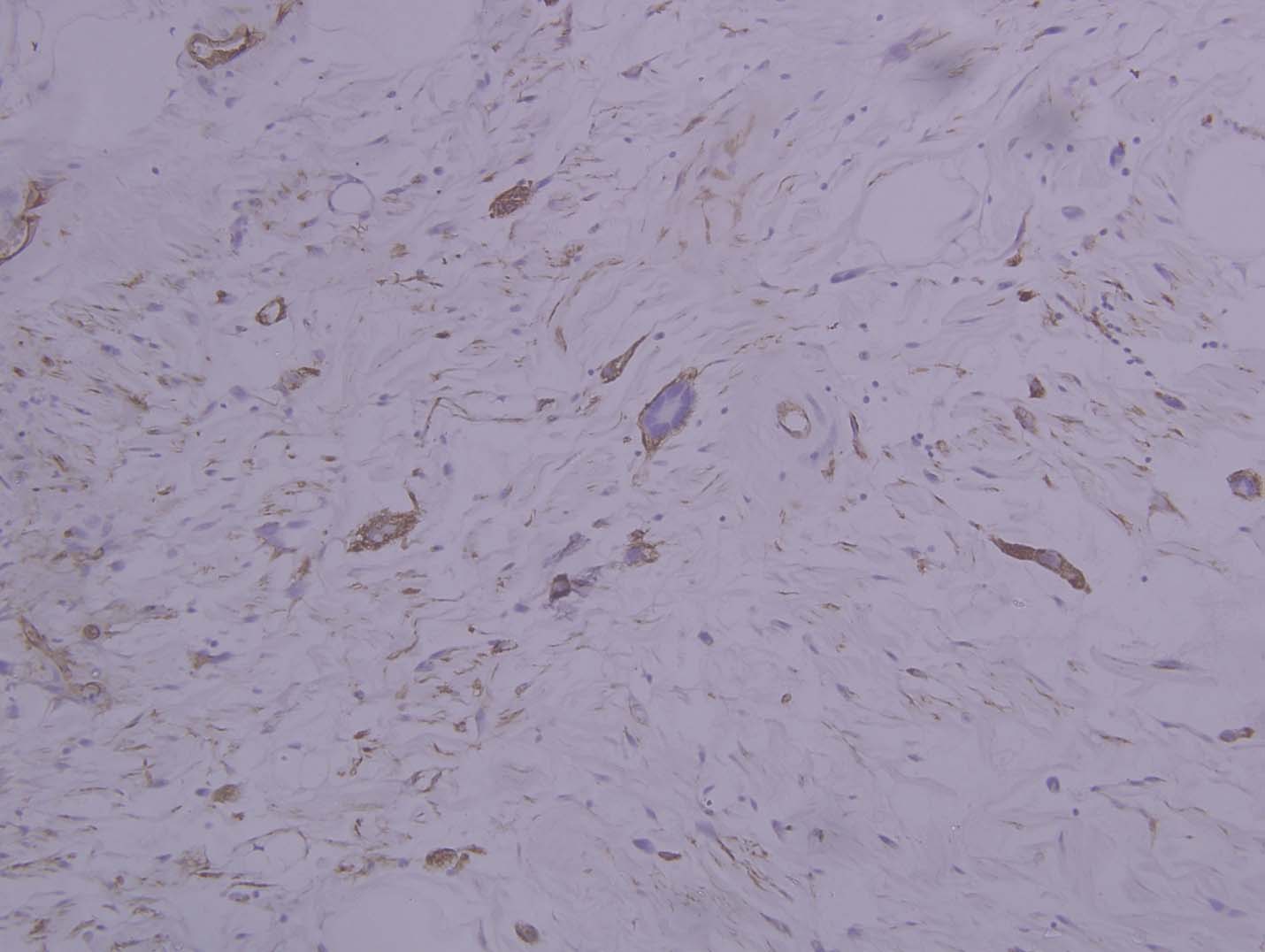
Photomicrograph showing a positive CD34 staining in spindled cells (IHC, 4X).
Discussion
Lipomatous tumours are the most common mesenchymal tumours. Liposarcoma is the most common adult soft tissue sarcoma and constitutes 20% of all soft tissue malignancies [1]. The hallmark of liposarcoma is the lipoblast, the multivacuolated cell containing a scalloped nucleus. With peak incidence in the sixth decade seldom seen in children and young adults, they arise mostly in the head and neck, trunk, retroperitoneum and mesentry, present as painless enlarging masses [2]. Liposarcomas are classified into well differentiated, myxoid, round cell, pleomorphic and the dedifferentiated types. The well differentiated liposarcoma or atypical lipomatous tumour, the most common type is further classified into lipomatous, sclerosing, inflammatory and the most recently described spindled cell type which was described for the first time in 1994 by Des Tos AP et al., Seen in adults, it arises in the subcutaneous tissue of the shoulder, extremities and the head and neck [3]. It is histologically composed of adipocytic component that shows variation in cell size along with the presence of multinucleated lipoblasts showing scalloped nucleus [4,5]. The stromal cells show nuclear hyperchromasia. The lipoblasts are positive for S100 on IHS [4]. The term well differentiated liposarcoma is used when the tumour arises in the retroperitoneum and mesentry and is not amenable to surgical resection. Atypical lipomatous tumour is used for lesions of limbs and trunk that can be surgically resected, though both are morphologically and karyotypically identical [2].
Atypical lipomatous tumour, spindle cell lipoma, myxoid liposarcoma and spindle cell liposarcoma, the lesions composed of an adipocytic and spindle cell component were considered the as the histological differentials. Atypical lipomatous tumour shows variation in the adipocyte size with atypia, lipoblasts and hyperchromatic stromal cells. The present case had similar histomorphology but the lipoblasts did not show positivity for S100 and hence atypical lipomatous tumour was excluded [2].
Spindle cell lipoma is composed of mature adipocytes and spindled cells having a bland appearance, the spindle cells are CD34 positive. It does not contain lipoblasts. Presence of lipoblasts and atypia in the spindle cells ruled out spindle cell lipoma [2,4]. Histologically no chicken wire vessels were identified in the present case and hence myxoid liposarcoma was excluded [2].
Spindle cell liposarcoma is a distinct entity characterized by deletion of Rb-1 gene, it is composed of atypical spindled cells admixed with variable sized adipocytes. Multivacoulated lipoblasts can be seen in a myxoid background. The present case showed similar histological picture. Mentzel T et al., reported CD34 staining in the spindled cells which was also appreciated in our case [1,4]. These lesions are treated by simple excision and most of them have a good prognosis.
Conclusion
To conclude, there are still many unanswered questions regarding this entity like- Is spindle cell liposarcoma a distinct entity or is a hybrid of atypical lipomatous and spindle cell lipoma as it combines their histological and immunohistiochemical features repectively? Is spindle cell lipoma a precursor of spindle cell liposarcoma as both the tumours show Rb-1 deletion and this could be an early event in the pathogenesis of the tumour with additional hits required for the development of spindle cell liposarcoma? Is it time we classify soft tissue sarcomas as denovo or secondary? These questions need to be answered to reach a correct diagnosis. This calls for a joint effort on part of the surgeon and the pathologist. This is a rare entity and hence presence of lipoblasts warrants a careful search for atypical spindled cells to make sure that this entity is not missed.
[1]. Gaurish SKS, Sanjay D, Vandana PG, Amruta BJ, Vaishya H, A spindle cell well differentiated liposarcoma/atypical lipomatous tumor of the neck: a rare case with immunohistochemical studySarcoma Res Int 2014 1(1):3 [Google Scholar]
[2]. World Health Organization Classification of TumoursPathology and genetics. In: Fletcher CDM, Unni KK, Mertens F (eds)Tumours of Soft Tissue and Bone 2002 LyonIARC Press [Google Scholar]
[3]. Dei Tos AP, Mentzel T, Newman PL, Fletcher CD, Spindle cell liposarcoma, a hitherto unrecognized variant of liposarcoma. Analysis of six casesAm J Surg Pathol 1994 18:913-21. [Google Scholar]
[4]. Mentzel T, Palmedo G, Kuhnen C, Well-differentiated spindle cell liposarcoma (‘atypical spindle cell lipomatous tumor’) does not belong to the spectrum of atypical lipomatous tumor but has a close relationship to spindle cell lipoma: clinicopatholossgic, immunohistochemical, and molecular analysis of six casesMod Pathol 2010 23:729-36. [Google Scholar]
[5]. Nascimento AF, Fletcher CDM, Spindle cell liposarcoma/atypical lipomatous tumor. A clinicopathologic study of 120 casesMod Pathol 2005 18:70A [Google Scholar]