Pelvic organ prolapse disorders are more common in elderly female population. Women who had vaginal delivery have a higher incidence of pelvic organ prolapse than women who have undergone caesarean delivery [1]. Sacral colpopexy is a surgical technique for repairing pelvic organ prolapse in women. A higher BMI have been associated with increased prevalence of pelvic floor disorders [2]. Some studies have demonstrated that with increase in age, aorta enlarges and elongates [3,4]. During sacral colpopexy, likelihood of a decreased APT distance in elderly and hypertensive patients require careful identification of aorta bifurcation and sacral promontory before dissection.
Surgeons should be familiar with proximity of nearby vessels to avoid complications to the iliac artery, veins and aorta bifurcation [5,6]. Presacral haemorrhage incurred during dissection of sacral promontory is one of the most feared complications of sacral colpopexy. Vascular variation in location of the level of the bifurcation and formation are important and evaluation before operation helps in planning of the anterior surgical approaches of the lumbar vertebrae. Overweight and obese patients require increased presacral dissection and have a higher risk of vessel injury. The number of anterior lumbar procedures are expected to increase significantly and so spinal surgeons should have a good knowledge about the occurrence of anatomic changes for prevention and treatment of vascular complications during surgical operations [7]. Therefore, this study was conducted to aid surgeons who operate for pelvic disorder in female patients for careful identification of aorta and sacral promontory before dissection to avoid complication. The objective of the study was to compare patient age and BMI with CT measured APT.
Materials and Methods
The study approval was obtained for this retrospective study by the Institutional Research Committee, School of Allied Health Sciences, and ethical committee of Kasturba Hospital, Manipal University, Manipal, Karnataka, India. The study was carried out within duration from October 2015 to March 2017 after obtaining informed consent. Sample size was obtained by taking estimation of mean formula, where the level of significance was set at 5% and power of study 80%. Considering the inclusion and exclusion criteria, 172 samples were selected by convenience sampling technique. Inclusion criteria consisted of female patients aged 18 years and above. Male patients, pregnant patients, patients with sacral injury and spinal diseases were excluded from study.
All the scans were performed on 64 slice and 16 slice MDCT scanners at Department of Radiodiagnosis and Imaging, Kasturba Hospital, Manipal. Study was performed on female patients who underwent CECT scans of abdomen. The CECT abdomen protocol includes the plain abdomen without contrast followed by contrast administration and arterial phase at 8 second and Porto venous phase at 45 second. The abdomen protocol used was 5 mm slice thickness, 5 mm increment, standard (C) filter, collimation of 64 X 0.625 with 0.984 pitch and 0.75 rotation time and matrix size of 512 X 512. Data such as age and BMI of female patients was collected from medical records of the patients.
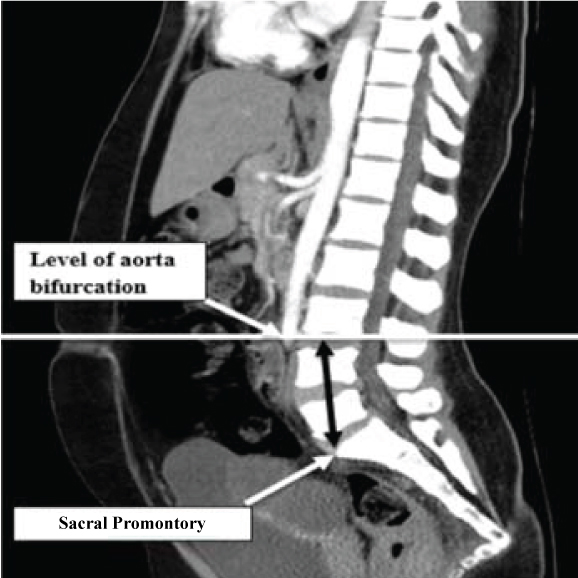
The aorta-sacral promontory distance was measured by reconstructing arterial phase of the abdomen for purpose of measuring. On sagittal 5 mm slice of arterial image, point of aortic bifurcation and sacral promontory were identified and then distance from level of aortic bifurcation to sacral promontory was measured. Vertical distance was represented as aorta-sacral promontory distance [Table/Fig-1].
Image showing aorta-sacral promontory distance.
Statistical Analysis
The collected data was statistically analyzed using multiple linear regression and Pearson’s correlation test utilizing Statistical Package for Science Software (SPSS, version 15.0).
Results
From total sample size of 172, data was collected from 147 subjects who underwent CECT scan for abdomen. Due to less time period, the number of female patients in BMI group >30 and also number of patients in age group >80 years was less. Female patients were categorized into four age groups of 18-38, 39-59, 60-80, 80 and above. The mean age was 56.5 years (range 18-95 years). Total number of patients in age groups of 18-38 years, 39-59 years, 60-80 years was 43 each and in age group of 80 years and above, number of patients was 18 [Table/Fig-2]. As the age group increased, there was a decrease in mean APT distance. The mean APT distance was longer among the age group of 18-38 years and overweight group. APT distance was short in elderly female patients and obese patients.
Comparison of Mean aorta-sacral promontory distance with age and Body Mass Index.
| Age (in years) | Number of Patients | Aorta-sacral promontory distance (mm) Mean±standard error |
|---|
| 18-38 | 43 | 39.83±0.61 |
| 39-59 | 43 | 29.51±0.76 |
| 60-80 | 43 | 25.44±0.96 |
| 80 and above | 18 | 17.06±0.19 |
| BMI |
| Underweight (<18.5) | 64 | 30.27±1.14 |
| Normal (18.5 to <25) | 55 | 29.15±1.25 |
| Overweight (25 to <30) | 21 | 30.43±1.73 |
| Obese (30 and above) | 7 | 29.08±2.68 |
Mean BMI was 23.25 (range 10.8-35.7). The number of patients in underweight group (BMI <18.5) was 64, normal BMI group (18-25) was 55, in overweight group (25-30) was 21 and in the obese group (30 and above) there were seven patients. As BMI increased in patients, there was no significant increase or decrease in mean APT.
Overall, there is a strong, negative correlation between APT and age. Increase in age is correlated with decrease in APT (Pearson’s correlation coefficient (r) is - 0.795 between age and APT, p<0.01). There is a weak, negative and no correlation between BMI and APT (Pearson’s correlation coefficient (r) is - 0.005 between BMI and APT, p>0.01) [Table/Fig-3]. Multivariate linear regression was performed to find relation between APT with age and BMI which showed that with the unit increase in age, there was an exponential decrease of 0.371 and for unit increase in BMI, there was an exponential increase of 0.085. Hence, age and BMI is responsible for 63% of variation in APT distance. Therefore, there is an overall significant relation between APT with age and BMI.
Univariate linear regression models for predictors of aorta-sacral promontory distance.
| Variables | r-value | p-value |
|---|
| Age | -0.795 | <0.001 |
| Body Mass Index | -0.005 | 0.307 |
The bifurcation of the aorta into right and left iliac arteries with reference to the lumber vertebra was also observed and it was found out that out of 147 subjects, 133 subjects (90%) bifurcation was found to be at the level of L4 vertebra (43 at upper end plate of L4 and 90 at the mid L4 region) and 14 subjects it was at the level of L3-L4 intervertebral space.
Discussion
The number of elderly patients undergoing surgeries for pelvic floor disorders is increasing gradually in recent years [3]. As more patients are seeking surgical treatment for pelvic prolapse, surgeons should be familiar with proximity of nearby vessels to avoid complications to the iliac artery, iliac veins and aortic bifurcation. Before a surgery, it will be beneficial for surgeons if APT is measured using CT scans which can prevent intraoperative complications like injury to vessels, haemorrhage, ureteral injury and enterotomy.
The present study was performed to compare aorta-sacral promontory distance with patient age and BMI in female patients undergoing CT, this study shows that as the age group increases, there is a significant decrease in mean APT. However, as BMI increases in patients, there is no significant increase or decrease in mean of APT. The mean APT was longer among the age group of 18-38 years and overweight group. APT distance was short in elderly female patients and in obese patients.
In the study conducted by Forbang NI et al., to find the association between cardiovascular disease and aortoiliac bifurcation in 1711 participants, the bifurcation position was determined using CT by measuring Aorto-Iliac Bifurcation Distance (AIBD) [8]. The mean AIBD was found to be 26±15 mm and the mean age was 62±10 years. The present study showed similar results with Forbang NI et al., study with the mean distance of 27.96±0.63 mm and mean age of 56.5±8 years. Agrawal A et al., performed a study to correlate patient age with APT [3]. Mean age was 56.6 years old (range 14.3-55.8) and mean APT measured on CT which was 63.11±1.02 mm. There is a big difference noted in the mean APT distance which may be due to geographical variations in morphology of human body.
The knowledge of aortic bifurcation with reference to lumbar vertebra has a significant role in surgery. In a study conducted by Korneich L et al., the average level of aortic bifurcation was found to be at the upper L4 in males and lower parts of L4 in females [4]. In Forbang et al., study too; almost two third of patients had aorta bifurcation at the level of L4 [9]. Also, in Lee CH et al., and Voboril R et al., study, the results of the common site of aortic bifurcation was at L4 vertebra which was same as present study [10,11].
Limitation
Less sample size. Due to less time period, the number of female patients in BMI group >30 and also number of patients in age group <80 years was quite less. Further, CT/MRI studies can be done based on different geographical areas using larger sample size.
Conclusion
During abdominal sacral colpopexy, the possibility of decreased APT in the elder female patients should be considered so that surgeon can carefully perform dissection. The BMI of the patient must be assessed before the surgery mainly in overweight and obese patients since those patients require increased presacral dissection. This study can be helpful for surgeons in avoiding complications.