Resilient liners are considered as boon to the geriatric dental practice as they are most widely used and are constantly explored for the scope of more improvement in the physical properties, to increase their clinical longevity. Soft liners are day by day becoming an indispensable material for clinically challenging situations and treating the patients with removable, maxillofacial or implant supported rehabilitations. They are classified into plasticized acrylic resins and silicone elastomers [1] and are present in auto and heat polymerized forms [2].
Resilient denture liners do have certain limitations in the clinical applications, as they become hard, get deformed, absorb fluids, encourages growth of Candida albicans and show debonding between soft liners and denture bases thus requiring frequent replacements [1,3-6].
According to an update on advances in the soft liners, the soft liners surface sealer protects them against the environmental pressures due to mechanical and chemical factors [7].
Recent in vivo study done by Ogawa A et al., on the effect of patient characteristics on maxillary dentures lined with acrylic soft liners, they concluded that smoking, night wearing of denture, denture cleanser practice, type of denture and resting saliva pH play an important role in deterioration of acrylic soft liners [8].
Soft liners are still considered as temporary expedients because no liners have durability comparable to resin denture base. Enhanced strength, lasting resiliency, better bond to the denture bases, the ability to prevent microbial growth, and chemical permanence till date, are the main highlights of ongoing researches [9].
According to an in vitro study done by Kutlu IU et al., acrylic based soft liners demonstrated rougher surfaces and sealer coatings used in that study had no substantial effect on the surface roughness [10].
The effect of coating agents have been evaluated previously with both positive and negative results in various studies on tissue conditioners, but no in vivo studies have been conducted till date that assess the effects of Varnish, Monopoly and Kregard surface coating agents together on the soft liners. The null hypothesis proposed was that there exists no difference between the effectiveness of three types of surface coating agents when applied on acrylic based soft liner.
Materials and Methods
Patients who reported to the Department of Prosthodontics and Crown and Bridge, KM Shah Dental College and Hospital, Sumandeep Vidyapeeth, Gujarat, India having edentulism were selected in the study according to the inclusion and exclusion criteria of the study. Ethical approval for the study was granted by the Institutional Ethics Committee No. SVIEC/ON/DENT/BVPG-13/D14213. Each participant was provided the basic information about the study through the patient information sheet and a signed informed consent form was obtained.
An edentulous patient who required complete maxillary and mandibular dentures was selected as inclusion criteria of the study. These participants however were not clinically indicated cases for soft liners. The exclusion criteria was patients who either had or were prone to oral candidal infection, mental, physical disability or psychological disorders, palatal defects, small arches, poor foundation and patients who refused to give informed consent for the study.
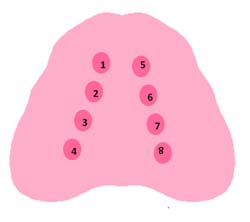
According to previously done similar studies [11,12] with 80% power, 95% CI and SD=1.09, a minimum of 31 patients were required for the study. However considering a 20% dropout in the study, the sample size was calculated as 37. Every maxillary denture had eight palatal recesses [Table/Fig-1], hence a total of 296 samples were obtained from the 37 participants. Palatal recesses of 5 mm diameter x 3 mm depth were prepared on denture bearing surface to receive soft liner. This procedure was conducted by incorporating eight metal dies (5 mm diameter x 3 mm depth) during dough packing stage (Heat cure acrylic resin - DPI, Batch No.-1081, 1083, Mumbai, India) of complete denture processing. These metal dies were removed after denture processing, thus eight recesses of same size were obtained. Postinsertion denture adjustments were carried out during follow up visits. Once the patient was satisfied with the existing denture, application of the acrylic based soft liner Permasoft (Dentsply Austenal) was carried out according to the manufacturer’s instructions. It was placed inside all eight recesses that were prepared before and was kept in patient’s mouth for a total setting time of 10 minutes. Later the denture was cured in the pressure pot (TTK Prestige Limited, Bengaluru, India) between 50°C to 74°C at 20 psi for 10 minutes as recommended by the manufacturer of the soft liner (Permasoft - DentsplyAustenal).
Eight recesses in palatal concavity of maxillary complete denture - Diagramatic representation
1, 5 - Control group (Uncoated) soft liner filled recesses;
2, 6 - Surface treatment of Varnish to soft liner filled recesses;
3, 7 - Surface treatment of Monopoly to soft liner filled recesses;
4, 8 - Surface treatment of Kregard to soft liner filled recesses.
The protocol for preparation and application of different surface coating agents like Varnish (resin based) [13], Monopoly (one part of clear acrylic resin polymer by weight to 10 parts of heat-cured acrylic resin monomer) [11,12,14,15] and Kregard (an ethyl acetate solution that contains 8% fluorinated copolymers composed of 50% vinylidene fluoride, 30% chlorotrifluoroethylene, and 20% tetrafluoroethylene by weight) [16] was followed according to the previous done studies.
After this, soft lined recess no. 2 and 6 were coated with Varnish, 3 and 7 with Monopoly, 4 and 8 with Kregard and 1 and 5 were left uncoated as control groups [Table/Fig-1]. Patients were instructed to maintain the daily hygiene routine of dentures and to use wet gauze on the tissue surface of liner for cleaning purpose.
Surface integrity of soft liner was later analysed with a Scanning Electron Microscope (SEM - JSM-5610LV) by three independent observers [Table/Fig-2] and scored on a calibrated scale of 0 to 3 [Table/Fig-3]. A Durometer (Model 411, ASTM Type 00) [17] was used for evaluation of softness of soft liner. Higher value indicated more hardness.
Comparative SEM observations.
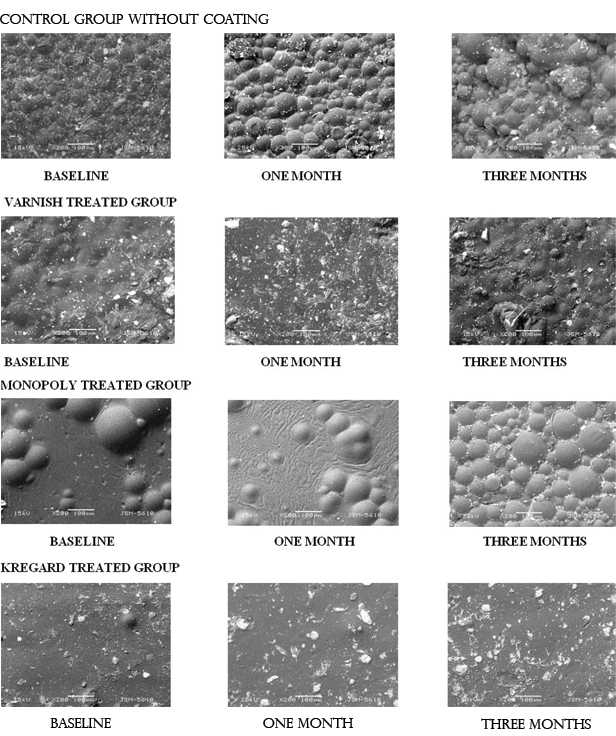
Scoring scale for SEM analysis [11,12].
| Score | Description |
|---|
| 0 | Surface intact (glass like appearance). |
| 1 | Surface intact with minor irregularities. |
| 2 | Severe wear with generalized pits and holes. |
| 3 | Severe wear with exposure of subsurface air bubbles. |
Surface integrity and hardness of soft liner was evaluated at baseline with different surface treatments in recess numbers 1, 2, 3, 4 by removing it from recess on day 1 itself. These recess numbers 1, 2, 3, 4 were again refilled with acrylic based Permasoft soft liner, surface coated with respective agents as previously described. Patient was recalled after one month for evaluation of hardness and surface integrity of the soft liner with different surface treatments of samples retrieved from trough numbers 1,2,3,4. These were then filled with self cure acrylic resin (DPI, RR, Mumbai, India). Participant was then recalled after two months. Thus, the samples in recess numbers 5, 6, 7 and 8 were exposed to a total use of three months. The soft liners from recess numbers 5, 6, 7, 8 were removed and evaluated after three months for hardness and surface integrity. The recesses were later filled with self cured acrylic resin and patient was kept on regular follow up as per prosthodontics protocols.
Statistical Analysis
For comparison of the surface integrity between groups Kruskal Wallis test and for comparison of the hardness between groups ANOVA and Tukey’s HSD post-hoc statistical tests were used. STATA/MP-13.0 statistical software was used for analysis and significance level was set at 5%. A p-value of <0.05 was considered statistically significant.
Results
The results of the Kruskal Wallis Test [Table/Fig-4] for Surface integrity shows that the Kregard Group had a statistically significant difference to other groups at each of the time intervals (p<0.001). Results of the one month observations also showed that the Varnish and Monopoly groups had a statistically significant difference when compared to the control group. Three month comparative results showed that the Varnish and Monopoly group had a non-significant difference when compared to the control group.
Comparison of median (inter quartile range) score of SEM at different time interval – Kruskal-Wallis test for Surface integrity.
| Groups | N | Median SEM score at baseline | Median SEM score at one month | Median SEM score at three months |
|---|
| Control | 37 | 1.0 (0) | 2.0 (0) | 2.0 (0) |
| Varnish | 37 | 1.0 (0) | 1.0 (0) | 2.0 (0) |
| Monopoly | 37 | 1.0 (0) | 1.0 (0) | 2.0 (0) |
| Kregard | 37 | 0.0 (0) | 0.0 (0) | 1.0 (0) |
| Chi - square | 147.00 | 135.28 | 147.00 |
| df* | 3 | 3 | 3 |
| p-value | <0.001 | <0.001 | <0.001 |
*df = Degree of Freedom
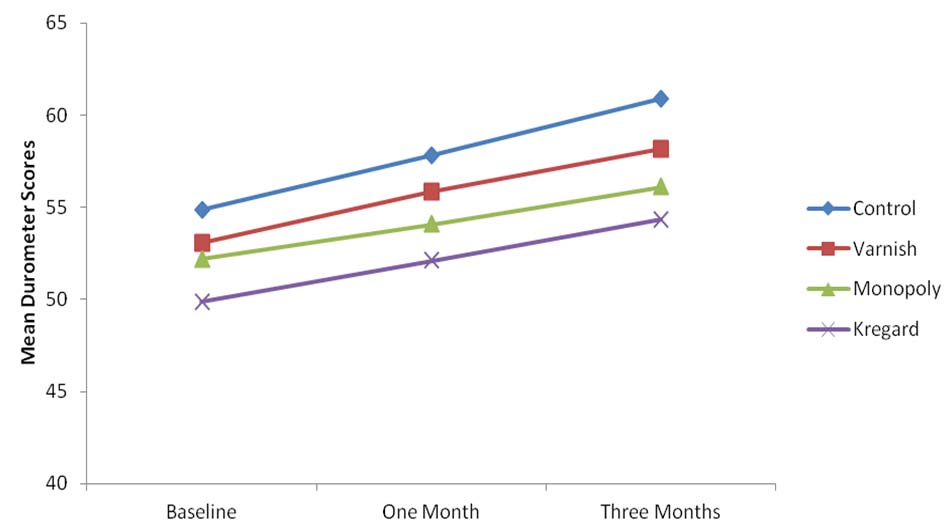
For hardness of soft liners, ANOVA [Table/Fig-5] was performed. [Table/Fig-6] shows that all the surface treatments improved softness of soft liner in comparison to untreated control group. Between all surface treated groups, less change in hardness was found for the Kregard treated group. Thus, surface treatment by the Kregard group showed better softness of acrylic based soft liner at baseline, at one month and at three months in comparison to Varnish and Monopoly treated groups at all the time intervals (p<0.001).
Analysis of variance - durometer comparison for different groups at different time interval.
| Durometer | Group | N | Mean value | Std. deviation | Std. error | 95% Confidence interval for mean | Source of variation | Sum of squares | df* | F | p-value |
|---|
| Lower bound | Upper bound |
|---|
| Durometer at baseline | Control | 37 | 54.84 SH | 0.374 | 0.061 | 54.71 | 54.96 | Between groups | 469.973 | 3 | 1.325x103 | <0.001 |
| Varnish | 37 | 53.08 SH | 0.277 | 0.045 | 52.99 | 53.17 |
| Monopoly | 37 | 52.19 SH | 0.397 | 0.065 | 52.06 | 52.32 | Within groups | 17.027 | 144 |
| Kregard | 37 | 49.89 SH | 0.315 | 0.052 | 49.79 | 50.00 |
| Total | 148 | 52.50 SH | 1.820 | 0.150 | 52.20 | 52.80 | 487.000 | 147 |
| Durometer at one month | Control | 37 | 57.81 SH | 0.397 | 0.065 | 57.68 | 57.94 | Between groups | 658.730 | 3 | 1.857 x103 | <0.001 |
| Varnish | 37 | 55.84 SH | 0.374 | 0.061 | 55.71 | 55.96 |
| Monopoly | 37 | 54.08 SH | 0.277 | 0.045 | 53.99 | 54.17 | Within groups | 17.027 | 144 |
| Kregard | 37 | 52.11 SH | 0.315 | 0.052 | 52.00 | 52.21 |
| Total | 148 | 54.96 SH | 2.144 | 0.176 | 54.61 | 55.31 | 675.757 | 147 |
| Durometer at three months | Control | 37 | 60.89 SH | 0.315 | 0.052 | 60.79 | 61.00 | Between groups | 885.892 | 3 | 2.033 x103 | <0.001 |
| Varnish | 37 | 58.19 SH | 0.397 | 0.065 | 58.06 | 58.32 |
| Monopoly | 37 | 56.11 SH | 0.315 | 0.052 | 56.00 | 56.21 | Within groups | 20.919 | 144 |
| Kregard | 37 | 54.32 SH | 0.475 | 0.078 | 54.17 | 54.48 |
| Total | 148 | 57.38 SH | 2.484 | 0.204 | 56.97 | 57.78 | | 906.811 | 147 | | |
*df = Degree of Freedom
Mean durometer scores at baseline, one month and after three months of time interval for all four groups.
Tukey’s post-hoc test [Table/Fig-7] shows multiple comparisons of four groups at different time intervals. All the groups showed statistically significant differences in their means when compared at each of the time intervals (p<0.001).
Tukey’s Post-Hoc test for comparison between different groups at different time interval for hardness.
| Dependent variable | Group | Mean Difference | Std. Error | p-value | 95% Confidence interval |
|---|
| Lower bound | Upper bound |
|---|
| Durometer at baseline | Control | Varnish | 1.757 | 0.080 | <0.001 | 1.55 | 1.96 |
| Monopoly | 2.649 | 0.080 | <0.001 | 2.44 | 2.86 |
| Kregard | 4.946 | 0.080 | <0.001 | 4.74 | 5.15 |
| Varnish | Monopoly | 0.892 | 0.080 | <0.001 | 0.68 | 1.10 |
| Kregard | 3.189 | 0.080 | <0.001 | 2.98 | 3.40 |
| Monopoly | Kregard | 2.297 | 0.080 | <0.001 | 2.09 | 2.51 |
| Durometer at one month | Control | Varnish | 1.973 | 0.080 | <0.001 | 1.77 | 2.18 |
| Monopoly | 3.730 | 0.080 | <0.001 | 3.52 | 3.94 |
| Kregard | 5.703 | 0.080 | <0.001 | 5.49 | 5.91 |
| Varnish | Monopoly | 1.757 | 0.080 | <0.001 | 1.55 | 1.96 |
| Kregard | 3.730 | 0.080 | <0.001 | 3.52 | 3.94 |
| Monopoly | Kregard | 1.973 | 0.080 | <0.001 | 1.77 | 2.18 |
| Durometer at three months | Control | Varnish | 2.703 | 0.089 | <0.001 | 2.47 | 2.93 |
| Monopoly | 4.784 | 0.089 | <0.001 | 4.55 | 5.01 |
| Kregard | 6.568 | 0.089 | <0.001 | 6.34 | 6.80 |
| Varnish | Monopoly | 2.081 | 0.089 | <0.001 | 1.85 | 2.31 |
| Kregard | 3.865 | 0.089 | <0.001 | 3.63 | 4.10 |
| Monopoly | Kregard | 1.784 | 0.089 | <0.001 | 1.55 | 2.01 |
Discussion
Most frequent problems seen in acrylic based soft liners are their deterioration of surface integrity, loss of softness, short durability, water absorption, adherence of microorganisms, foul odour and fungal infection. At present all the available acrylic based soft liners have short longevity and thus need replacement very frequently [15]. This adds to the financial burden of the patient and wastage of precious clinical chairside time.
Another limitation of acrylic based soft liners is the effect of the oral conditions on their physical properties, which leads to regular replacement [16]. Hence, there is a justifiable need to improve the clinical applicability of acrylic soft liner.
According to Singh K et al., Casey DM et al., Gronet PM et al., Malmstrom HS et al., and Dominguez NE et al., both plasticizers and alcohol leached out from the soft liner and was partially replaced by water [11,12,14,15,18].
To prevent the hardening of soft liners, various surface coating treatments were recommended by Singh K et al., [11]. The application of surface coatings helps to prevent absorption of salivary inorganic salts by acting as mechanical barrier [11]. To improve the surface integrity and clinical longevity, many authors have also recommended the use of a Varnish to reduce surface degradation. This leads to a decrease in the formation of wrinkles and porosities [16], thereby less biofilm formation and Candida albicans colonization [19,20]. Singh K et al., also concluded that Monopoly reduced the loss of softness of a tissue conditioner [21]. However, till date no study attempted to test all the agents together in an in vivo condition on the acrylic based soft liner.
The suggested null hypothesis for the study was rejected because the statistical test showed a significant difference between various surface treatments for both parameters and indicates that surface coating agents maintain surface integrity and hardness of soft liner (p<0.001).
In this study, among the three surface treated groups, Kregard showed a statistical significant result in comparison to Varnish, Monopoly and control groups. For surface integrity of soft liners, Kregard showed significant value and improved the surface with glass like appearance. The main reason for maintenance of softness by various coating agents was that it reduced the loss of plasticizer from the material. The leaching of the plasticizers was reduced because of the maintenance of surface integrity [11].
The result of this study supports the findings of other authors [11,16], regarding the application of surface coating agents, though they had worked on tissue conditioners. Dayrell A et al., Also advocated the usage of surface sealers however, they recommended the reapplication of sealers every three months to prevent the detachment of sealer from denture [22]. Rahal JS et al., also supported the use of surface glaze and varnish for the reduction in biofilm formation [23].
Limitation
One of the limitations of this study is usage of single brand of acrylic soft liner. The different soft liners having varying composition can show different results with the coating agents used in this study. In future, more studies having different types of soft liners can be undertaken to evaluate their clinical effectiveness and longevity with surface treatments. Keeping in mind the clinical longevity of acrylic soft liners this study had time period of only three months, future studies should be encouraged with increased time interval of around six months or more in patients with different systemic conditions and in patients with clinically indicated case of soft liners.
Research can be done in the areas such as, whether the use of surface coating agents help towards maintaining bonding between silicone based liners and denture base resins, as bonding seen between silicone liners and denture base resin is comparatively weak. The effect of surface coating agents used in the present study on biofilm formation on soft liner can also be an area of interest for researchers.
Conclusion
Within the limitations of this in vivo study, it was concluded that, amongst the three surface agents studied, Kregard was the best surface coating agent to maintain surface integrity and softness of acrylic based soft liner. Thus, it can improve the longevity and clinical effectiveness of chair side acrylic based soft liner.
*df = Degree of Freedom
*df = Degree of Freedom