Oral malodour is one of the oldest and most troublesome of social maladies and has been recorded in literature for thousands of years [1]. Understanding of this phenomenon has been seen to be lacking in the scientific community and also among the general society. ‘Halitosis’ is the general term used to describe any disagreeable odour in the expired air, regardless of whether the odouriferous substances originate from oral or non oral sources, while ‘oral malodour’ specifically refers to such odour originating from the oral cavity itself [2-4].
Halitosis can be internal (intraoral) or external (extraoral) or both in origin. A number of factors, both intraoral and extraoral, such as gingivitis, periodontitis, nasal inflammation, chronic sinusitis, diabetes mellitus, liver insufficiency, cirrhosis, uraemia, lung carcinoma, trimethylaminuria and postnasal drip have been identified for halitosis [5]. It has been documented in literature that around 87% of patients with bad breath had malodour of oral origin, whereas only 5%-8% had malodour of extraoral origin [6-8].
Oral malodour has been associated with both gingivitis and periodontitis; but it can be present in periodontal disease free individuals also. It originates in oral cavity because of degradation of proteins by bacteria producing VSCs hydrogen sulphide, methyl mercaptan and dimethyl sulphide are the major components in these VSCs. VSCs are found in saliva, gingival crevicular fluid produced as a result of proteolysis of protein substrates, mainly sulphur containing amino acids like cysteine and cystine [8]. Nonsulphur containing compounds like volatile aromatic compounds (indole, skatole), organic acids (acetic, propionic) and amines, i.e., cadaverine and putrescine also contribute to oral malodour [8].
Various methods have been used for detection of oral malodour. They are broadly classified as direct methods (organoleptic method, gas chromatography, sulphide monitoring - halimeter, breath alert) and indirect methods (BANA test, bacterial culture, direct bacterial smears, enzyme assay) [3]. In this study, a small hand held breath checking device ‘breath alert’ (Tanita®) was used. This portable monitor provides an objective reading which favours the organoleptic assessment [9].
Regular use of mouthwashes, supportive periodontal therapy and psychological counselling has been traditionally followed for the treatment of malodour. Mouthwashes have been consistently used in various studies reported in literature so far and CHX has been found to be effective in reducing oral malodour [10,11]. CHX being the most studied antimicrobial agent in the treatment of gingivitis has also been tested for its efficacy in the treatment of oral malodour. It has been shown to be successful in reducing bacterial activity in supragingival plaque as well as the bacterial load on the tongue, provides a significant reduction in VSCs levels because of its strong antibacterial effects and superior substantivity in the oral cavity, and thus is seen as potentially effective agent in controlling oral malodour [12,13]; but it has few disadvantages of increased tooth and tongue staining, dryness and altered taste sensation. Nevertheless, it is considered as a gold standard in the treatment of malodour [14].
Alternative medicines like ayurveda have been used in treatment of various disorders since centuries. G32 is a commercially available ayurvedic formulation available as tablet or solution, known to be antiseptic, anti-inflammatory, astringent, anodyne, styptic, deodorant, aromatic and healing agent. It contains harmless ayurvedic ingredients used traditionally since centuries; like bakula, chok, katho, laving, etc., [15,16].
Its main ingredient Mimusops elengi is known to contain chemicals like triterpenes and alkaloids and possesses antibacterial, antifungal, anticariogenic and free radical scavenging properties [17]. Other ingredients; namely Katha (Acacia catechu) [18], Laving (Myrtus caryophyllus) [18] and Vajradanti (Barleria prionitis) [19] are known for their antimicrobial and anti-inflammatory properties as reported in the literature. G32 is a combination of all these ingredients in varying proportions and has been widely used for ethnomedicinal purposes. Earlier studies have documented the use of G32 in treatment of oral malodour, gingivitis and other oral conditions [15,16]. However, there has been no study which has compared its effectiveness in treating malodour with that of CHX.
Therefore, this study was conducted with the aim to evaluate the effectiveness of G32 in controlling halitosis and comparing the effects with CHX; hypothesis being that G32 is as effective as CHX in treatment of halitosis.
Materials and Methods
Study design and participant characteristics: This single blind, parallel design randomized controlled trial (CTRI/2012/05/002695) was conducted on healthy volunteers of age group 17-35 years in TMA Pai hospital, Udupi Karnataka, India. The ethical approval to conduct the study was obtained from the Institutional Ethics Committee. The participants received detailed information about the study and signed an informed consent form. A total of 40 volunteers (20 males and 20 females) who fulfilled the inclusion and exclusion criteria were included in the study. Sample size of 40 was calculated based on effect size of 0.85, power of 80% and alpha error of 0.05 [20]. The recruitment of the study participants was conducted by one of the co-investigators not involved in group distribution and dispensing of the intervention medications. Allocation of subjects to either of the groups was done by a person not related to the researchers or subjects.
Selection criteria: Subjects who were willing to participate in this trial and whose VSCs and hydrocarbon gas levels were more than 3 (Breath Alert Tanita®) and who had periodontal pockets ≤4 mm (after a comprehensive periodontal examination) were included in the study. Exclusion criteria included the subjects who were smokers, were undergoing antibiotic therapy, had any medically compromised conditions contraindicating the oral examination or had active periodontitis and multiple carious lesions. Similarly, patients with systemic diseases pertaining to renal systems, liver and endocrine systems, respiratory system problems, gastrointestinal disease, hepatic disease, hematological or endocrine system disorders and metabolic conditions can all be the non oral causes of halitosis, and hence were excluded from the study sample.
Clinical examination: At the initial visit, the subjects were interviewed for recording their medical history, drug history and oral hygiene practices by one of the principal investigators (SH). They were requested to refrain from consuming odourous food items like onion, garlic, spicy food, tobacco, mouth fresheners, chewing gums, etc., 24 hours prior and not to use scented perfumes on the day of next scheduled appointment.
The VSC levels of the subjects were measured using a portable sulphide meter ‘Breath Alert’ (Tanita®). This hand-held device measures the levels of VSCs and hydrocarbon gases in mouth air. As the monitor is turned on, it emits a beep, when second beep is heard the patient is requested to blow into the air flow passage. After the third beep, odour levels is measured by grading on the display of instrument; 1 (no odour), 2 (mild odour), 3 (moderate odour), 4 (strong odour) [21].
The VSC scores were measured after the routine oral hygiene procedures in the morning but before the first meal of the day. To standardize the distance from which patients blew air into the machine, single examiner placed thumb on the patient’s chin and held the machine in vertical position, in an enclosed room which was free of any obvious odour that could have affected the sensitivity of the machine. Patient was advised to close his mouth for 2 minute prior to blowing into the machine. Three continuous readings, at a gap of one minute each, were taken and a consistent reading was considered. For validation of ‘Breath alert’, it was compared with the organoleptic method (gold standard).
Organoleptic assessment was conducted by a single examiner on a group of 10 subjects having oral malodour. Subjects were instructed to keep mouth closed and breathe through the nose for 2-3 minutes duration. Followed by which they expired through mouth at a distance of 10 cm from examiner nose. The intensity ratings of 0 to 5 score (no odour to strong odour), as proposed by Rosenberg M and McCulloh CA was used [22].
Other parameters measured during this study were the scores of plaque and gingivitis in the subjects. Gingivitis was evaluated using Löe H and Silness J index (1963) [23] and plaque with Silness J and Löe H index (1964) [24].
These parameters were measured by same investigator on a dental chair under adequate illumination, using a three way syringe, mouth mirror and probe.
Tongue coating was measured using Winkel tongue coating index (2003) [25]. The dorsum of tongue was divided into six areas, i.e. three in the posterior and three in the anterior part of the tongue. The tongue coating in each sextant was scored as 0– no coating, 1– light coating and 2– severe coating. The tongue coating value was obtained by the addition of all six scores, range 0-12 [26].
Following these examinations, the participants were provided at random (coin flip method) with G32 (Alarsin pharmaceuticals) or Chlorhexidine – digluconate 1% (Hexigel, ICPA company) in a wrapped container by an investigator, who was not a part of the clinical examination.
No change in the routine oral hygiene practices or any change in dietary habits was advised during the study period. Subjects of G32 group (intervention group) were advised to crush 2-3 tablets and massage it on the gums and surrounding areas twice a day for five minutes, once in morning and once before going to bed at night followed by rinsing the mouth with water. Similarly, the subjects of CHX group (control group) were advised to use the gel twice daily and massage the gums and surrounding areas for five minutes, once in morning and once before going to bed at night followed by rinsing the mouth with water.
Postintervention visit: All the parameters such as the VSC levels, gingivitis, plaque and tongue coating were measured again after one week of intervention. The subjects were interviewed about any perceived side effects during the course of study. Single examiner carried out all the recordings on both the occasions. Intra-examiner agreement was assessed using kappa coefficient. Kappa values for gingival, plaque and tongue coating scores were 0.86, 0.78 and 0.86, respectively.
Statistical Analysis
The differences between the mean scores of VSC, plaque and gingivitis and tongue coating were compared within the intervention and control groups respectively using paired t-test. For the comparisons of the overall mean reduction of all the clinical parameters measured, across both the groups, independent t-test was used. All the analysis was carried out using the Statistical Package for Social Sciences (SPSS) version 16.0. The cut off level for statistical significance was taken as 0.05.
Results
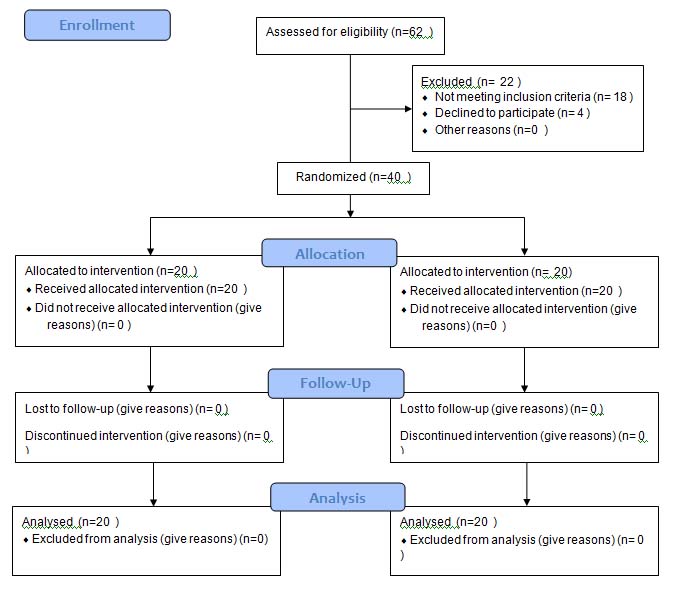
The present study constituted sample of 40 subjects (20 males and 20 females), 20 each in intervention (10 males and 10 females) and control groups (10 males and 10 females). There was no loss to follow up observed during the study period [Table/Fig-1]. There was no statistically significant difference in the participants in both CHX and G32 groups, according to the variables such as age of patient, sex of patient, plaque, gingival and halitosis scores at the baseline. Comparison between scores before and after intervention showed a trend towards a decrease in scores, with a statistically significant decrease for all plaque, gingival and halitosis scores in both the groups [Table/Fig-2].
Showing sequential methodology followed in the study.
Showing baseline characteristics and mean difference between pre and post intervention scores between CHX and G32 group.
| Clinical examinations | Baseline characteristics | Post-intervention scores | G32 group (intervention) | Chlorhexidine group (control) | p value |
|---|
| Chlorh-exidine (Mean ± SD) | G32(Mean ± SD) | Chlorh-exidine (Mean ± SD) | G32 (Mean ± SD) | Mean diffe-rence ± SD | Mean diffe-rence ± SD |
|---|
| Plaque scores | 1.52 ±0.64 | 1.79 ±0.54 | 0.56± 0.15 | 0.688± 0.05 | 0.85 ± 0.49* | 0.90± 0.59* | 0.02* |
| Gingival scores | 2.13 ±0.53 | 1.79 ±0.46 | 1.1± 0.09 | 0.974± 0.03 | 0.98 ± 0.44* | 1.13± 0.49* | 0.02* |
| Halitosis scores | 3.1 | 3 | 1.4 | 1.4 | 1.63± 0.49* | 1.68± 0.58* | 0.01 |
*p < 0.05 – considered as statistically significant
Paired t-test
The scores of ‘Breath alert’ were correlated with the scores of organoleptic assessment (gold standard) and the Spearman’s correlation coefficient was found to be 0.72 [Table/Fig-3]. The comparison of plaque, gingival and halitosis scores in intervention and control groups after one week follow up showed no statistically significant difference. (Mean difference being 0.04±0.17, 0.05±0.12, 0.05±0.17)
Shows the spearman correlation between the organoleptic assessment and breath alert scores.
The tongue coating scores before and after intervention, were 5.5 (±1.51) and 5.1 (± 1.3) for G32 group and 5.5 (± 1.3) and 5.3 (± 1.2) for CHX group, respectively. There was no statistically significant difference between the pre and post intervention tongue coating scores for both the groups. (p= 0.54 for intervention and p= 0.344 for control group).
Discussion
This controlled trial was designed to test the efficacy of G32 and CHX in reducing malodour of oral origin. Subjects with moderate to severe oral malodour were included in this study, as in such participants the baseline VSC levels would be high enough to evaluate the effects of formulations.
In our study, a hand-held device ‘Breath alert’, a sulphide monitor, was used as a method of oral malodour detection. Previous studies have shown this device to be effective in assessment of malodour. It is based on the same principle of measurement (Sulphide monitors) like Halimeter and provides objective reading which favours organoleptic assessment [9]. This monitor is easily available and has high reproducibility. They do not require skilled personnel to operate nor do they have high acquisition costs like gas chromatography or Halimeter. They are also devoid of the subjectivity and influence of other factors like age, gender, time of day, etc., which are the drawbacks of organoleptic method [26-28]. Few studies reported in the literature, till this date, have used Breath alert as an assessment tool for oral malodour [9,29,30].
Hence, as a confirmation, this machine was validated with the organoleptic method and was found to be well correlated with the results of organoleptic method. The reproducibility of the device was assessed by using three continuous readings and steady readings were observed and considered.
Oral microorganisms play an important role in the production of malodour. In the absence of microorganisms, the odouriferous compounds are not released. A predominance of Gram negative organisms like Peptostreptococcus, Eubacterium, Selenomonas, Centipeda, Bacteroides and Fusobacterium is found in the mouth of patients with oral malodour as these species are capable of producing VSCs [31-34]. Hence, CHX and G32 were used as chemical agents as they are known to have a bactericidal property.
In this study, there was a significant reduction in the mean VSC, plaque and gingival scores among the participants of G32 group. These findings were similar to the findings of the previous study in which self reported halitosis was measured [15]. CHX was used in this study as it is a gold standard in treatment of halitosis [32-36]. It was used in a gel form, as this form has been shown to be as effective as the mouthwash and spray [37-39]. There was a significant reduction in the mean VSC, plaque and gingival scores among all the participants of CHX group. Similar findings have been reported in a previously conducted study [6].
In this study, no significant difference between the preintervention and postintervention tongue coating scores were observed, yet a substantial reduction in VSCs scores was achieved. This interesting finding disregards the conventional belief that dorsum of tongue is the primary source of VSCs in oral malodour patients and stresses on the fact that the composition of tongue coating might be a better indicator than its extent [8].
To eliminate any bias, the participants were asked to follow their routine oral hygiene practices and were matched for their sociodemographics, VSCs, plaque and gingival scores at baseline. Examination by the dentist might have introduced some bias in the study, as the participants might get over cautious and start following meticulous oral hygiene practices. But such a phenomenon might have occurred in both the groups, and hence would have nullified the effect.
None of the subjects in G32 group complained of burning mucosa, altered taste sensation, dryness of mouth or other adverse effects during the course of the study, similar to earlier study [14]. On the contrary, few subjects of CHX group complained of burning mucosa and drying of mouth on subsequent visit. The occurrence of such effects can influence the compliance of patients, which forms the basis of long term management of chronic conditions like oral malodour [37-40]. This study was conducted for a short duration of time, yet it can be considered that the results of G32 were pointing in the favourable direction.
During the course of the study, it was observed that G32 was more economical compared to CHX. This seems to be a key issue for two reasons. Firstly, when chronic disorder like halitosis is being considered, the cost of treatment matters and secondly, in country like India, where people are reluctant to spend more money on oral health, cost will definitely have a major influence on treatment choice and might affect the compliance of patients.
Few studies reported in the literature have induced halitosis using ‘morning breath model’ for assessment of efficacy of various preparations [41,42].
Such a model has a drawback that oral malodour is induced in healthy volunteers by instructing them to abstain from any routine oral hygiene practice for few days [6]. But in this study, only oral malodour cases were included and measurement of VSCs was done after the oral hygiene procedure in the morning but before the first meal of the day. This allowed the actual assessment of the VSCs scores as the influence of the food and morning breath was eliminated.
Limitation
The major drawbacks of this study can be the short duration of follow up, a relatively smaller sample size. Nevertheless, this study provided evidence that G32 is an effective alternative to conventional therapy, in treating oral malodour in periodontally healthy individuals.
Future studies can be conducted using G32 for treating oral malodour in subjects of various age groups and various grades of periodontal involvement. Reduction in levels of oral malodour can also be assessed using G32 in conjunction with other mechanical oral hygiene aids. Long term studies should be conducted to assess the stability of the VSCs scores reduction. Microbiological changes brought about by the application of G32 can be assessed in other studies using samples from plaque and GCF.
Conclusion
Hence, it can be concluded that G32, with its lack of side effects, can be an effective tool to deal with oral malodour. It was found to be as effective as CHX in dealing with oral malodour. It can prove to be useful in various special groups who have difficulty in mechanical oral hygiene practices.
*p < 0.05 – considered as statistically significant
Paired t-test