Non Traumatic Fracture of Pedunculated Osteochondroma: Conservative Management of a Rare Case
Ahmet Senel1, Erhan Sukur2, Huseyin Nevzat Topcu3
1 Orthopaedic Surgeon, Department of Orthopaedics and Traumatology, Istanbul Training and Research Hospital, Istanbul, Istanbul, Turkey.
2 Orthopaedic Surgeon, Department of Orthopaedics and Traumatology, Sakarya Training and Research Hospital, Sakarya, Sakarya, Turkey.
3 Orthopaedic Surgeon, Department of Orthopaedics and Traumatology, Sakarya Training and Research Hospital, Sakarya, Sakarya, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ahmet Senel, Istanbul Training and Research Hospital Department of Orthopaedics. Kasap Ilyas Mah Org. Abdurrahman Nafiz Gurman Cad, Fatih Istanbul, Istanbul, Turkey.
E-mail: ahmetsenel23@gmail.com
Fracture of a pedunculated osteochondroma is a rare complication for which surgical treatment is usually advocated. In this report, we present the functional and radiological outcomes of a case of a conservatively treated fracture of a pedunculated osteochondroma. A 26-year-old man with no history of trauma presented with acute onset of left knee pain, oedema, and limited range of motion. Radiological assessment revealed a fracture of a pedunculated osteochondroma. It was treated conservatively with an elastic bandage and non-steroidal anti-inflammatory drugs, and union was achieved by the 12-week follow-up, with no complications. Although surgical treatment is usually advocated for a pedunculated osteochondroma fracture, conservative treatment should be the first approach to avoid complications of surgical intervention.
Bone neoplasms, Conservative treatment, Fracture
Case Report
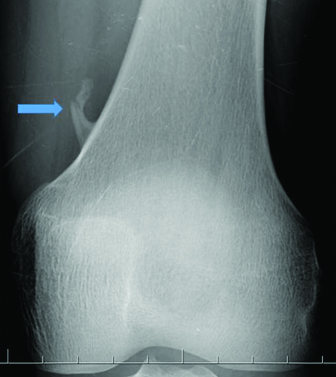
A 26-year-old male patient presented with acute pain and swelling over distal and anteromedial aspect of his left thigh, while he was jogging, about 12 hours before his presentation to us. On physical examination, there was a tender and palpable mild swelling over anteromedial aspect of his left thigh. The range of motion was limited, with 80° flexion. Neurovascular examination revealed no abnormality. Radiological evaluation revealed that a fracture through the stalk of a pedunculated osteochondroma which located on the left femur adductor tubercle [Table/Fig-1]. Based on the patient’s medical history, the osteochondroma had been incidentally diagnosed six years back. Further imaging with Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) performed to confirm the clinical suspicions of a fractured osteocondroma [Table/Fig-2]. The patient was fully informed regarding the findings of the imaging studies. Patient was offered with different treatment options, and he elected and consented to conservative management. An external elastic compression band was provided to avoid difficulties with mobilization. Non steroidal anti inflammatory drugs were prescribed for pain control. He was followed weekly in Orthopedics Outpatient department. Symptoms began to decrease after three weeks. At the eighth week, he was without pain and had full range of motion. At the last follow up at 12 weeks, radiography confirmed bone union [Table/Fig-3].
Direct radiography demonstrated a fracture through the stalk of a pedunculated osteochondroma, which originated from the adductor tubercle of the left femur;
Three-dimensional computed tomographic view of the osteochondroma.

Imaging shows bone union after 12 weeks.

Discussion
Osteochondromas account for 10% of all bone tumours and, among these, 35% (20%–50%) of the benign tumours. [1]. They are most often diagnosed in long bones, particularly distal femur and proximal tibia. Most of time, osteochondromas are symptomless and often found incidentally, when plain radiographic imaging is performed for an unrelated reason [2]. Surgical treatment is considered when they become symptomatic as a result of complications. Mechanical irritation or neurovascular compromise due to mass effects exerted by the anomaly is the most frequent complication and reason for surgical treatment. Moreover, there is a small but important risk of malignant transformation to an osteochondrosarcoma [3]. Finally, fracture of an osteochondroma is a very rare complication that is intensely uncomfortable for the patient and is therefore symptomatic [4]. Osteochondromas are abnormal growths in the bone, thought to be developmental lesions, unlike true neoplasms [5]. Non-traumatic fractures of osteochondromas rarely occur, but they are symptomatic [5-7]. Such fractures usually occur spontaneously from friction caused by muscles or tendons that insert close to the lesion. As in this case, they are usually pedunculated, with the fracture occurring through the stalk [8,9]. As the patient, in this case could not remember any trauma history, we concluded that indirect muscle contraction was the cause of the fracture. Currently, given their rarity, there is no consensus on the management of these lesions, and controversy over treatment is also prevalent in the literature [2,5,6]. Some authors have recommended excision of fractured osteochondromas, especially in young people, since they are likely to experience recurrent fractures due to their high physical activity and also because they tend to be good candidates for surgery, as their post-operative recovery is more favourable [5,9]. However, other authors suggest non-operative treatment [4]. Our patient did not have any symptoms before fracture, so we decided to treat him conservatively. At the four weeks follow up, the patient was symptom free and appeared to have made a full recovery. Non traumatic fracture is a very rare complication and could be the first symptom of a pedunculated osteochondroma.
Conclusion
Although surgical excision is recommended by some authors, for fractures of pedunculated osteochondromas, invasive surgery should be avoided where possible. Additionally, conservative treatment should be the first treatment approach in order to avoid risks associated with surgical intervention.
[1]. De Souza AMG, Bispo Júnior RZ, Osteochondroma: ignore or investigate?Rev Bras Ortop 2014 49:555-64. [Google Scholar]
[2]. Mishra PK, Gupta A, Gaur SC, Dwivedi R, Non-traumatic fracture of pedunculated osteochondroma. A case report and brief review of literatureJ Orthop Case Rep 2013 3(4):46-48. [Google Scholar]
[3]. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, Osteochondromas: review of the clinical, radiological and pathological featuresIn Vivo 2008 22(5):633-46. [Google Scholar]
[4]. Errania C, Vanelb D, Donatic D, Piccid P, Faldinia C, Spontaneous healing of an osteochondroma fractureDiagn Interv Imaging 2015 96(3):283-85. [Google Scholar]
[5]. Kose O, Ertas A, Celiktas M, Kisin B, Fracture of an osteochondroma treated successfully with total excision: two case reportsCases J 2009 2:8062 [Google Scholar]
[6]. Davids JR, Glancy GL, Eilert RE, Fracture through the stalk of pedunculated osteochondromas: a report of three casesClin Orthop 1991 271:258-64. [Google Scholar]
[7]. Prakash U, Court-Brown CM, Fracture through an osteochondromaInjury 1996 27(5):357-58. [Google Scholar]
[8]. Woertler K, Lindner N, Gosheger G, Osteochondroma: imaging of tumour-related complicationsEuropean Radiology 2000 10:832-40. [Google Scholar]
[9]. Carpintero P, León F, Zafra M, Montero M, Berral FJ, Fractures of osteochondroma during physical exerciseAm J Sports Med 2003 31(6):1003-06. [Google Scholar]