Brugada Syndrome with Spontaneous Fluctuation in ECG Pattern
Abhishek Goyal1, Varun Loomba2, Naved Aslam3, Bishav Mohan4, Gurpreet Singh Wander5
1 Assistant Professor, Department of Cardiology, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana, Punjab, India.
2 Resident, Department of Cardiology, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana, Punjab, India.
3 Professor, Department of Cardiology, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana, Punjab, India.
4 Professor, Department of Cardiology, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana, Punjab, India.
5 Professor, Department of Cardiology, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhishek Goyal, Dayanand Medical College and Hospital Unit Hero DMC Heart Institute, Ludhiana-141001, Punjab, India.
E-mail: drabhishekgoyal11@yahoo.in
Brugada ECG types, Hereditary channelopathies, Spontaneous variation
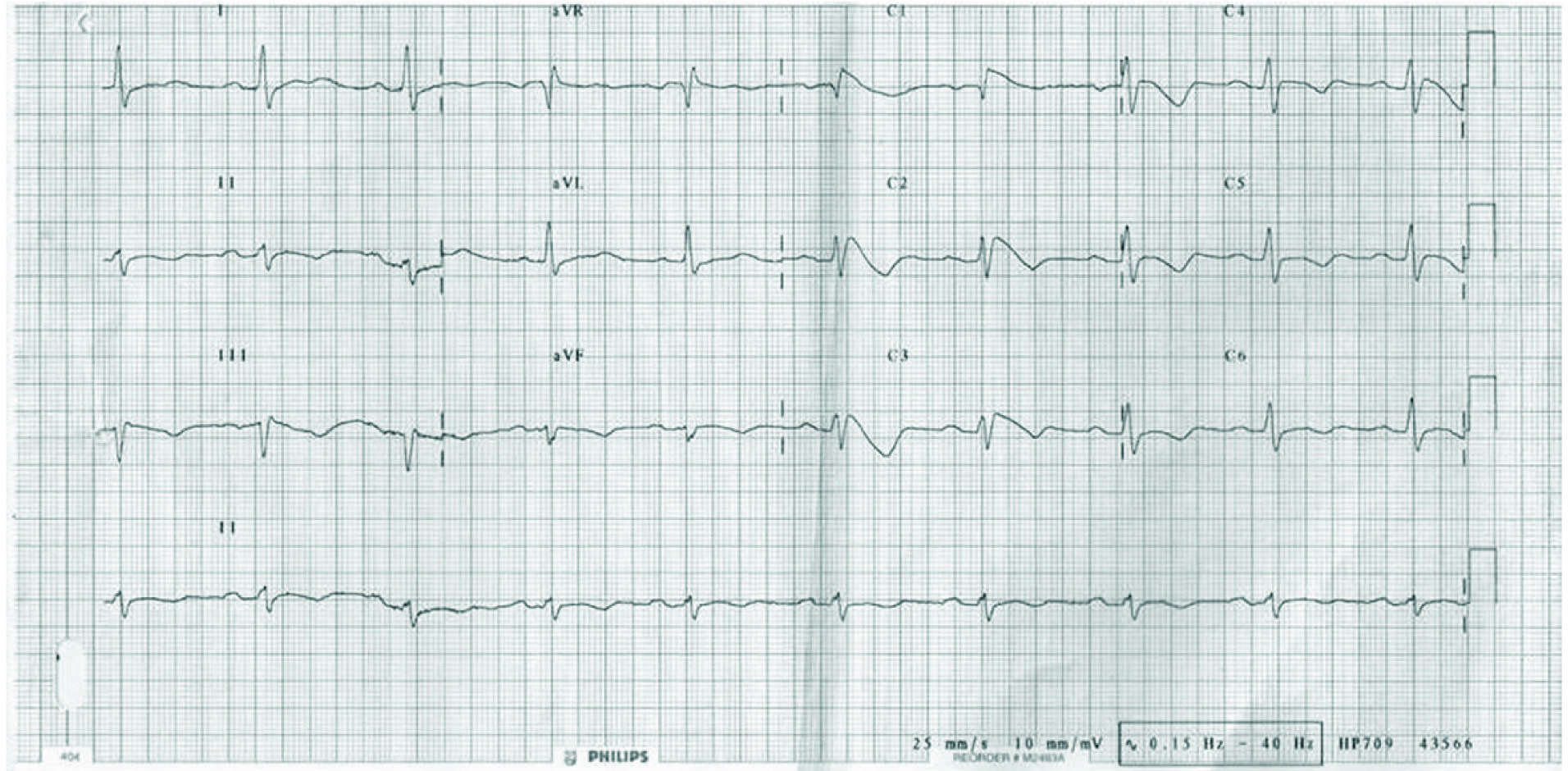
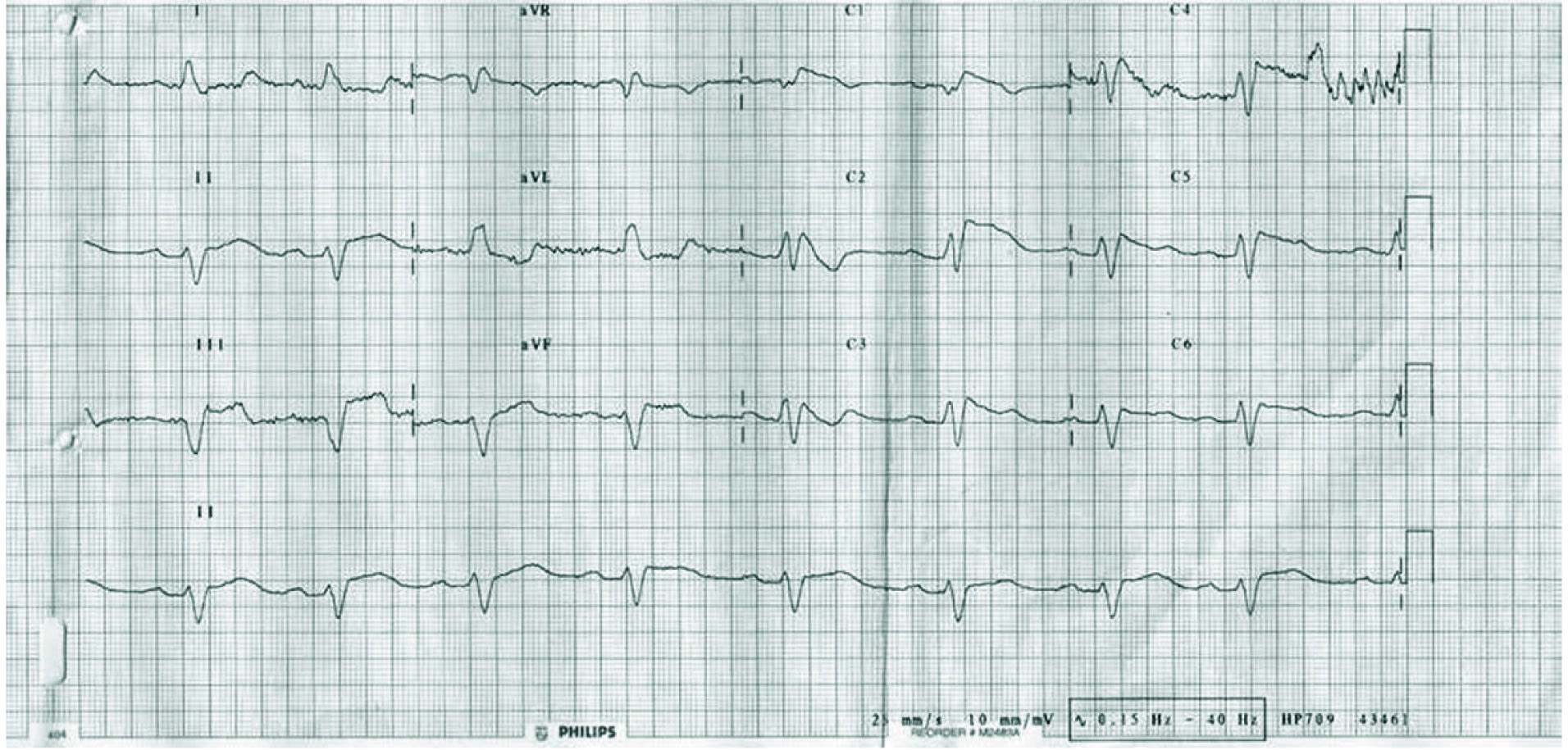
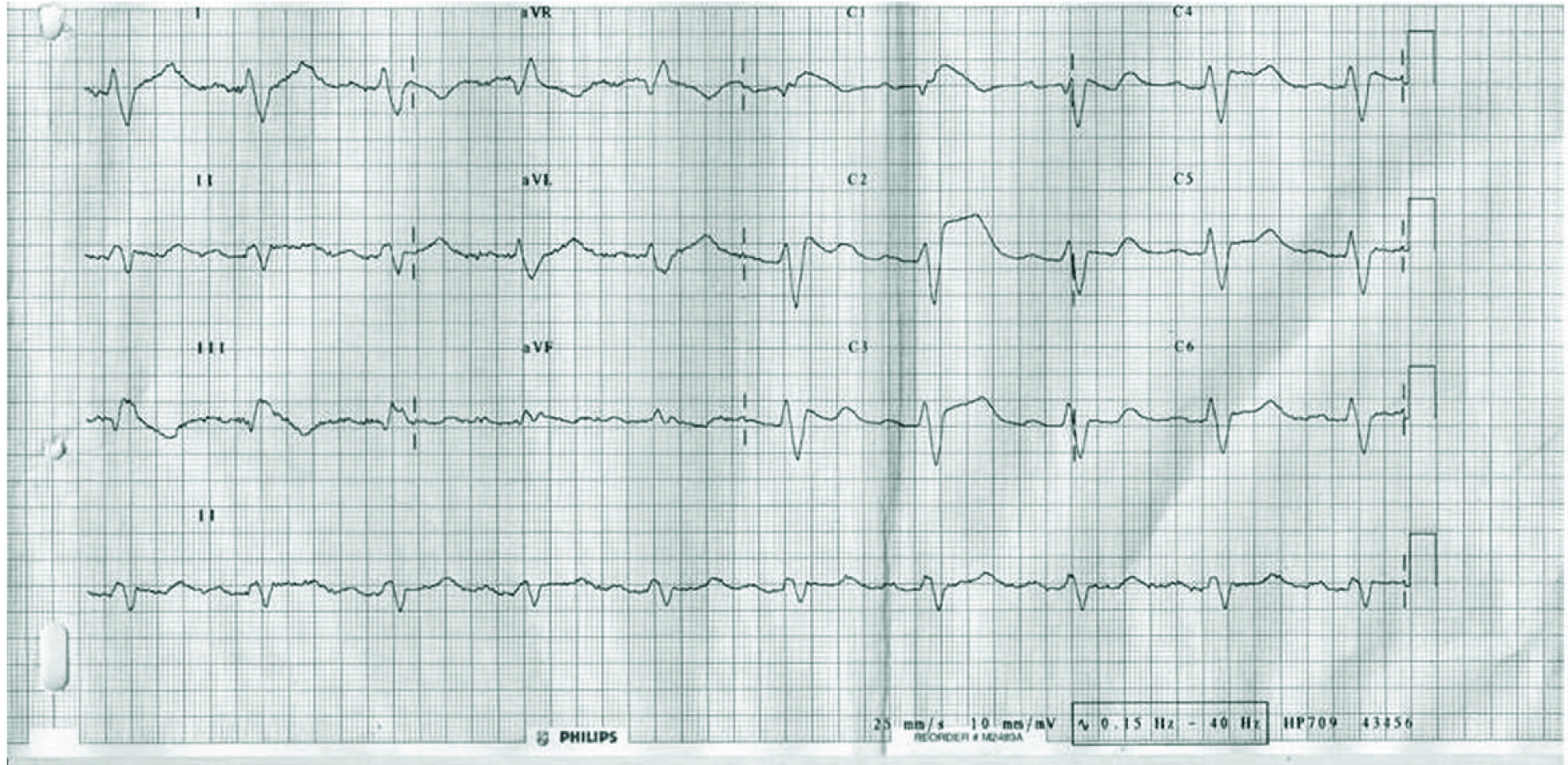
A 32-year-old male, presented with one month history of recurrent episodes of syncope. General physical examination and 2D Echocardiography (ECG) were normal. ECG was suggestive of Brugada Syndrome with spontaneous occurrence of Type I pattern [Table/Fig-1] which is defined as ST elevation ≥2 mm in ≥1 of right precordial leads V1, V2 and is diagnostic of Brugada syndrome according to the HRS/EHRA/APHRS Expert Consensus Statement [1]. The most remarkable finding was a beat to beat fluctuation in Brugada pattern [Table/Fig-2,3]. Type I pattern spontaneously changed to Type II pattern which is seen in 1st and 2nd QRS complex of lead V2 [Table/Fig-2] and is defined as saddle-back pattern with a least 2 mm J-point elevation and at least 1 mm ST elevation. Spontaneously changing ST segment was quite frequently seen in another ECG also [Table/Fig-3]. Such changing ST segment morphology, both daily and circadian fluctuation are well known in Brugada Syndrome specially in symptomatic individuals and confers higher risk of arrhythmia [2]. There was significant and spontaneous variation in QRS duration which varied from 120 msec [Table/Fig-1] to 200 msec [Table/Fig-2,3]. Spontaneous variation in QRS duration is well known and more common seen in symptomatic individuals [3]. This is a unique case which demonstrates myriad ECG manifestations of Brugada Syndrome.
Type I ECG pattern diagnostic of Brugada Syndrome.
Beat to beat change in ECG pattern from Type I to Type II.
Spontaneously changing ST segment morphology.
The patient was treated with implantable cardioverter defibrillator and is on follow up for the last two years, during which he has had one episode of ventricular tachycardia, which was successfully terminated by the device.
[1]. Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, HRS/EHRA/APHRS Expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromesHeart Rhythm 2013 10(12):1932-63. [Google Scholar]
[2]. Tatsumi H, Takagi M, Nakagawa E, Yamashita H, Yoshiyama M, Risk stratification in patients with brugada syndrome: analysis of daily fluctuations in 12-Lead Electrocardiogram (ECG) and Signal-Averaged Electrocardiogram (SAECG)J Cardiovasc Electrophysiol 2006 17(7):705-11. [Google Scholar]
[3]. Junttila MJ, Brugada P, Hong K, Lizotte E, DE Zutter M, Sarkozy A, Differences in 12-lead electrocardiogram between symptomatic and asymptomatic brugada syndrome patientsJ Cardiovasc Electrophysiol 2008 19(4):380-83. [Google Scholar]