Case Report-1 (CR-1)
A 55-year-old female patient reported to the Outpatient Department of Conservative Dentistry and Endodontics with chief complaint of pain in lower right back tooth since three days. Pain was moderate in intensity, non-radiating and arose on chewing. She gave history of severe, continuous, radiating pain in the region two months back, that subsided after few weeks. Medical history was non-contributory.
Oral examination revealed Class II (mesio-occlusal) deep caries in relation to 47. Tooth was tender on percussion and pulp sensitivity tests {cold, Electric Pulp Test (EPT)} revealed no response compared to adjacent and contralateral teeth. Radiograph revealed mesio-occlusal radiolucency of 47 approximating the pulp chamber space, with widening of Periodontal Ligament (PDL) and loss of lamina dura.
Case REPORT-2 (CR-2)
A 38-year-old female patient reported with chief complaint of pain in lower right back tooth since 10 days. There was a history of dull, persistent pain several months back that subsided after few weeks. Medical history was non-contributory.
Oral examination revealed tooth-coloured restoration (class II disto-occlusal) in relation to 47. Tooth was tender on percussion and pulp sensitivity tests (cold, EPT) revealed no response. Radiograph revealed disto-occlusal radioopacity with underlying radiolucency approximating pulp chamber space, with widening of PDL and loss of lamina dura.
For both CR-1 and 2, based on clinical and radiographic findings, provisional diagnoses of necrotic pulp with symptomatic apical periodontitis were made. Informed consent was obtained.
Categorization and management: Preoperative radiographs revealed fused roots in CR-1; and closely-placed roots in CR-2. On clinical inspection of pulp chamber floor, the two cases were classified as given in [Table/Fig-1].
Categorization of C-shaped anatomy in the two cases [3-6].
| Classification based on: | Pre-operative Radiograph | Finding after Access opening | Finding after Access opening | Finding after Access opening | WL Radiograph | Obturation Radiograph |
|---|
| ClassificationType: | Radiographic (Fan-2004) | Anatomic (Melton-1991) | Modified Anatomic (Fan-2004) | Types of pulpal floors (Min & Fan-2006) | Radiographic(Fan-2004) | Radiographic (Fan-2004) |
| Case Report–1 (CR-1) | Square & Fused roots; Type-II | Category-III; Subdivision-III | C2 | Type-III | Type-II | Type-II |
| Case Report–2 (CR-2) | Closely-placed roots; Type-I | Category-II | C1 - C3(afterorificeenlargement) | Type-II | Type-I | Type-I |
Gates-Glidden (GG) drills (#1-3) were used to enlarge orifices. CR-2 revealed closely-placed Mesiobuccal (MB) and Mesiolingual (ML) orifices with an indiscernible isthmus between them [Table/Fig-2a,b].
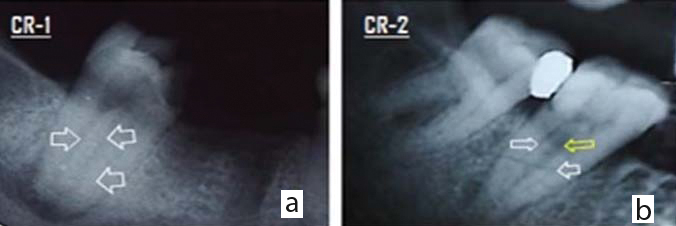
Assessment of pre-operative radiographs. a) CR-1 show three canals arsing from pulp chamber floor (white arrow); b) CR-2 shows two canals arising from pulp chamber floor (white arrow), with radiolucent line of inter-radicular area (yellow arrow).
Under local anaesthesia, caries was excavated. Access opening was done, pulp chamber floor was examined [Table/Fig-3a-c].
Application of Fan’s (modified anatomic) classification to clinical apperance of pulp chamber floor. a) In CR-1, angle a is more than 60° (C2); b) CR-2 prior to orifice enlargment; c) In CR-2, both angle a and b are less than 60° (C3).

Working Length (WL) was established with radiograph and apex locator (Propex®II, DENTSPLY). Assessment of radiograph of CR-2 led one to a similar conclusion as mentioned before: MB- and ML-canals in close proximity merging at apical-third. WL radiograph for both cases revealed the appearance of files exiting via furcation [Table/Fig-4a,b].
Assessment of working length radiographs. a) CR-1 shows three separate canals; b) CR-2 shows narrow isthmus between MB and ML-canal.

Cleaning and shaping was done by ProTaper® Universal rotary (DENTSPLY) upto F3 (buccal) and F4 (distal canals) in both cases. Throughout instrumentation, 2.5% NaOCl was used as irrigant. EndoActivator® (DENTSPLY) was used to agitate NaOCl in the root canal. After saline flush, 17% EDTA was retained in root canals for one minute. Final flush of saline was used to neutralize all irrigants.
Calcium hydroxide intracanal medicament in glycerine vehicle was inserted by lentulo-spiral (#30,40). Closed dressing was given with temporary restoration (CavitTM, 3M ESPE).
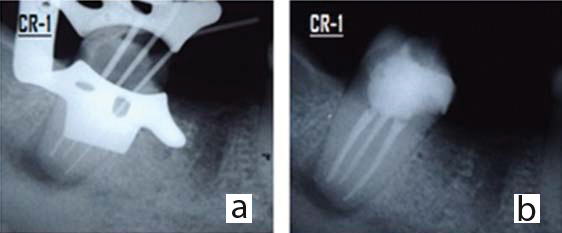
After one-week, since patients were asymptomatic, obturation was done. CR-1master cone radiographs revealed separate root canals below pulp chamber floor. Hence, they were obturated by cold lateral compaction with master cone (#30-4% taper-buccal canals; #40-4%-distal canal) and sealer (AH Plus®, DENTSPLY) [Table/Fig-5a,b].
Obturation in CR-1. a) Master cone radiograph; b) Obturation
In CR-2, a modified obturation technique was used: first, a master Gutta-Percha (GP) cone (#30-4% taper) was coated in sealer, inserted to WL into MB-canal, sheared off at canal orifice and a spreader (#25) was inserted upto 1 mm short of WL. This spreader was left in place. Next, cold lateral compaction was carried out in ML-canal (master-GP#30-4% taper) [Table/Fig-6a].
Obturation in CR-2. a) Schematic diagram of modified cold lateral obturation used in CR-2; b) Master cone radiograph; c) Radiograph shows obturation of isthmus between MB and ML canal.
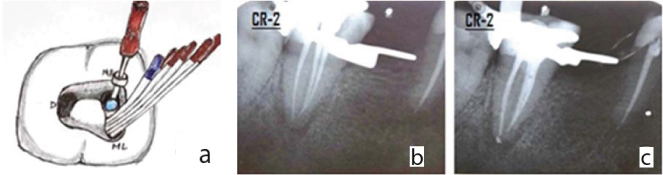
Finally, obturation of MB-canal, followed by distal canal (master-GP #40-4%) was completed by cold lateral technique [Table/Fig-6b,c].
Discussion
For root canal systems to be named “C-shaped”, the general consensus it that they have to exhibit all the following three features: fused roots, longitudinal groove on lingual and/or buccal root surface and at least one cross-section of canal belongs to C1, C2, or C3 configuration [1].
The C-shaped canal variation of morphology is unusual and can lead to difficulties during treatment [2]. Proper diagnosis, as well as categorization based on the classification systems is mandatory before treatment. Predicting the possible anatomical C-shaped variations helps one to effectively confer root canal treatment.
Attaching a name to the anomalous C-shaped canals led to its widespread recognition by researchers. This led to various classification systems, notable of which were the ones developed by Melton DC et al., Fan B et al., and Min Y et al., [1,3-5].
The classification systems depict the complexity of C-shaped anatomy and aid in predicting their anatomy, thus enabling instrumentation and obturation. The two cases treated were classified based on preoperative radiograph, clinical appearance after access cavity preparation and WL and obturation radiographs.
Radiographic interpretation is effective when based on film combinations [6]. Preoperative radiographs show either closely-placed/ fused roots, or two distinct roots when the dentin fin connecting them is thin and thus, not visible on radiograph [7-9]. The two cases showed these characteristic signs.
The high resolution of CBCT confers many advantages [10], but it should be used only when the situation does not permit adequate diagnosis using conventional dental radiography [11].
Cemento-Enamel Junction (CEJ) is reliable landmark and ‘principles of colour change and orifice location’ can be successfully applied in C-shaped roots [12]. Deep-orifice preparation is needed to characterize C-shaped category more accurately [9]. After GG-drills were used to enlarge orifices, CR-2 revealed a narrow isthmus between MB- and ML-canal.
WL radiograph for both cases revealed files exiting via furcation. Also, MB- and ML-canals were in close proximity and merging at apical-third. These are characteristic findings [9]. Since a file could not be passed through the isthmus on pulpal floor, a narrow dentin fin was speculated to be present, with canals merging below isthmus [12].
Care was taken to perform anti-curvature filing using rotary to preserve thin dentin isthmus, i.e., the mandated “brushing motion” was preferentially carried out away from furcation [12]. Because of large area of canal space, it is doubtful that instruments can debride effectively, making irrigation more significant [2]. Sonic agitation system, EndoActivator® was used to agitate NaOCl in the root canals to enable better irrigant penetration.
The selected obturation procedure should predictably move gutta-percha and sealer into root canal aberrations. But in C-shaped canals, conditions are different: divergent areas offer resistance to obturating material flow and communications between main canals prevent attainment of obturation density [2]. However, a meta-analysis of ten clinical studies showed no significant difference in long-term outcome between warm gutta-percha and cold lateral condensation [13].
Since the operative radiographs of CR-1 revealed separate root canals below pulp chamber floor, they were obturated by cold lateral compaction. In CR-2, an isthmus of dentin was suspected below pulp chamber floor, with buccal canals merging at apical-third. The obturation technique described by Walid N (utilizing two pluggers simultaneously to downpack two canals) [14] was modified for use with cold lateral compaction. A spreader was used to wedge the master GP against the isthmus and act as temporary wall (matrix) between MB- and ML-canal while obturation was carried out in ML-canal.
Conclusion
The various classification systems proposed over the years depict the complexity of C-shaped root canal morphology. At the same time, these classification systems serve as a guide to predicting their anatomy, thus aiding in effectively providing root canal treatment. Modifications of well-established treatment protocols are required when managing such anomalous root canal systems.
[1]. Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z, C-shaped canal system in mandibular second molars: Part I–Anatomical featuresJ Endod 2004 30:899-903. [Google Scholar]
[2]. Kato A, Ziegler A, Higuchi N, Nakata K, Nakamura H, Ohno N, Aetiology, incidence and morphology of the C-shaped root canal system and its impact on clinical endodonticsInt Endod J 2014 47(11):1012-33. [Google Scholar]
[3]. Melton DC, Krell KV, Fuller MW, Anatomical and histological features of C-shaped canals in mandibular second molarsJ Endod 1991 17(8):384-88. [Google Scholar]
[4]. Fan B, Cheung GS, Fan M, Gutmann JL, Fan W, C-shaped canal system inmandibular second molars: Part II-Radiographic featuresJ Endod 2004 30(12):904-08. [Google Scholar]
[5]. Min Y, Fan B, Cheung GS, Gutmann JL, Fan M, C-shaped canal system in mandibular second molars: Part III - The morphology of the pulp chamber floorJ Endod 2006 32(12):1155-59. [Google Scholar]
[6]. Lambrianidis T, Lyroudia K, Pandelidou O, Nicolaou A, Evaluation of periapical radiographs in the recognition of C-shaped mandibular second molarsInt Endod J 2001 34:458-62. [Google Scholar]
[7]. Barril I, Cochet JY, Ricci C, Treatment of a canal with a “C” configurationRev Fr Endod 1989 8:47-58. [Google Scholar]
[8]. Haddad GY, Nehme WB, Ounsi HF, Diagnosis, classification and frequency of C-shaped canals in mandibular second molars in Lebanese populationJ Endod 1999 25:268-71. [Google Scholar]
[9]. Jafarzadeh H, Wu YN, The C-shaped root canal configuration: a reviewJ Endod 2007 33(5):517-23. [Google Scholar]
[10]. Kottoor J, Velmurugan N, Ballal S, Roy A, Four-rooted maxillary first molar having C-shaped palatal root canal morphology evaluated using cone-beam computerized tomography: a case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod 2011 111:e41-45. [Google Scholar]
[11]. Special Committee to Revise the Joint AAE/AAOMR Position Statement on use of CBCT in EndodonticsAAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 UpdateOral Surg Oral Med Oral Pathol Oral Radiol 2015 120(4):508-12. [Google Scholar]
[12]. Hargreaves KM, Cohen P, Cohen’s pathway of pulp 2011 10th edMissouriMosby Elsevier [Google Scholar]
[13]. Peng L, Ye L, Tan H, Zhou X, Outcome of root canal obturation by warm gutta-percha versus cold lateral condensation: a meta-analysisJ Endod 2007 33:106-09. [Google Scholar]
[14]. Walid N, The use of two pluggers for the obturation of an uncommon C-shaped canalJ Endod 2000 26:422-24. [Google Scholar]