Presbyopia (literally, an old eye) is the most common ocular problem worldwide. Presbyopia is defined as progressive decrease in the accommodative amplitude leading to discomfort and difficulty for near work [1]. It is due to the progressive decrease in the accommodative amplitude [2]. The changes in accommodation are related to changes in the ciliary muscles, lens, and its capsule and/or changes in the vitreous. The onset of presbyopia varies between 40 and 45 years of age however, some individual and geographic variations are present [3,4]. Women from rural area are more likely to report difficulty with near tasks than men because they are more occupied with near work such as sewing and cleaning grains [2]. Symptoms of presbyopia are characterized by complaints of requiring more light to read, difficulty in reading fine print of newspaper and eyes taking too long to focus at near point. Uncorrected near vision will have negative impact on activities of daily living like reading newspaper, seeing mobile numbers and also upon self esteem [4, 5].
There exists a high prevalence of uncorrected refractive errors and presbyopia; especially in developing countries [5]. Even though presbyopia affects a large number of individuals and is treated easily, it has not gained recognition as a major cause of vision impairment. Those with refractive error in addition to presbyopia need bifocals which depends on the nature of his/her work [6].
The present study was conducted to assess the awareness among rural females regarding presbyopia. To the best of our knowledge, there is no past report on awareness of presbyopia among the community of rural female population from India.
Materials and Methods
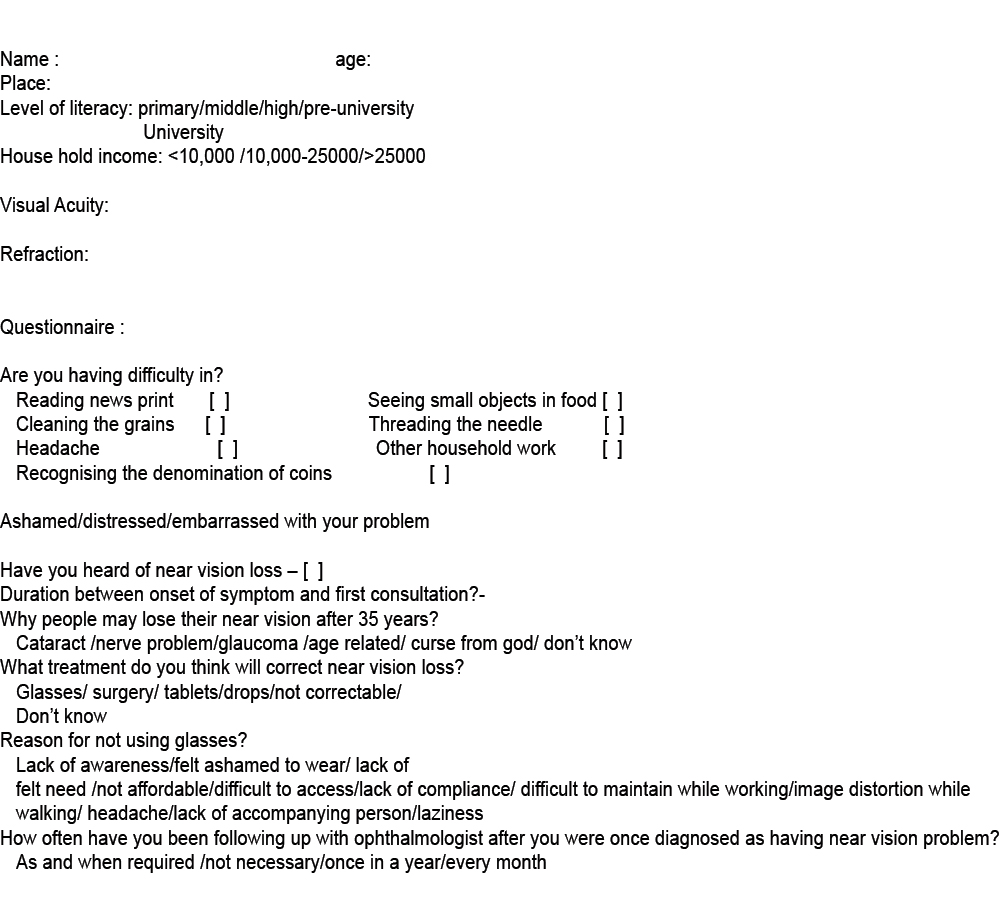
A hospital based cross-sectional study was conducted among female subjects aged 35 years and above. A total of 1000 subjects were examined. The study was conducted from April 2015 to May 2016. Written informed consent was obtained from each patient in their local language (Kannada). SDM Medical College Hospital Institutional Ethics Board approval was obtained before the conduct of the study, which adhered to the tenets of the Declaration of Helsinki. A questionnaire was used to capture all demographic data and assessment findings [Table/Fig-1].
Questionnaire used for demographic data and assessment findings.
We included all the females >35 years of age, coming from rural area (around Dharwad), who attended Ophthalmology OPD. We excluded subjects with best corrected visual acuity less than 20/40 due to cataract or other causes.
Sample Size
There are no surveys in study population which give us an indication of the prevalence of knowledge of presbyopia among the general population.
We started with survey and analysed the proportion of awareness of presbyopia among the first 100 subjects in our study. We found 20% proportion of awareness of presbyopia.
The sample size for the proportion for a population survey was found out by CDC-statcalc software. The optimum sample size at alpha error of 5% and power of 80% works out to be 164 subjects at prevalence of 50% and 145 subjects at prevalence of 67% awareness.
We were comfortable in collecting data from a larger sample of out patients. Hence, we continued up to an arbitrary number of 1000 subjects which was much more than what we required for the parameter of awareness of presbyopia. There was an additional advantage of using a larger population sample in the analysis of the lesser important parameters like causes of presbyopia.
Ocular examination included measurement of Best Corrected Visual Acuity (BCVA) for distant vision with Snellen’s charts or illiterate E chart at 6 m in a well-lit room. Refraction was done on all subjects who presented with a visual acuity worse than 6/6 in either eye. Objective refraction was performed with a streak retinoscopy and further refined with subjective refraction. Near vision was assessed in all subjects using a Snellen’s near vision chart or illiterate E near chart at working distance of 33 cm after correcting their distance vision. Each person who could not read N8 vision after best distance correction was checked for improvement by adding appropriate increments. Slit lamp examination of anterior segment and posterior segment, pupillary reaction and Intraocular Pressures (IOP) was performed in all study subjects and was within normal limits in all the subjects.
Demographic details and literacy levels of all the subjects was obtained. A brief structured, open ended questionnaire was designed to record subjects’ awareness and knowledge about presbyopia [Table/Fig-1]. The questionnaire was initially developed in English and all the questions were translated into commonly used language in study area, that is Kannada. The questionnaire was administered by the interviewer.
Development of Questionnaire
knowledge Attitudes and Practices (KAP) questionnaire was developed and validated by Ophthalmologists colleagues, language and public health experts. None of the questions in final Kannada version were unacceptable by patients and no questions seemed to upset or distress any of the patients.
Reliability of Questionnaire
Initial 250 subject’s responses were analysed. Out of 250, 44 subjects said, they had knowledge of presbyopia. Among them, 40 knew that wearing glasses was the treatment of this condition and four subjects said, ‘they don’t know’ whereas, 206 had not heard of near vision loss.
Reliability of the questionnaire collected was tested by comparing the collected data by two readers. The initial data pertaining to 250 subjects was repeated in respect of question number 2 and 5 which pertained to the perception of what will cure the condition. The data collected was tabulated and Cohen’s Kappa coefficient was measured which is a measure of interrelated agreement of categorical questionnaire. The obtained kappa of 0.68, suggests a ‘substantial’ grade of agreement as per Cohen (0.61-0.80) [7].
Statistical Analysis
Social parameters related to presbyopia like age group, literacy were described in terms of rates and ratios. Refractive status was similarly described. Various symptoms of presbyopia were elucidated and tabulated according to responses and enumerated in terms of rates and percentages. Same questions changed into attitude and practice and the responses were classified according to questionnaire, elicitation of KAP.
The presence of awareness according to literacy status has been cross tabulated. The cross tabulations was analysed by Chi-square test for the association of the attributes.
Results
In this study, 1000 female subjects were examined. [Table/Fig-2] shows the demographic characteristics of the subjects. More than one third of subjects were in the age group of 40-44 years and 45-49 years, each with 373 subjects (37.3%) and 360 subjects (36%) respectively. The remaining age groups were 35-39, 50-54, 55-59 and 60-69 years, constitute 2.3%, 12.70%, 9.2%, and 2.5% cases respectively [Table/Fig-2].
Age group and level of literacy in study subjects.
| Age group in years | Number | Percentage% |
|---|
| 35-39 | 23 | 2.3 |
| 40-44 | 373 | 37.3 |
| 45-49 | 360 | 36.0 |
| 50-54 | 127 | 12.7 |
| 55-59 | 92 | 9.2 |
| 60-69 | 25 | 2.5 |
| Literacy status |
| Illiterate | 495 | 49.5 |
| Primary school | 115 | 11.5 |
| Middle school | 142 | 14.2 |
| High school | 155 | 15.5 |
| Pre university | 79 | 7.9 |
| University | 14 | 1.4 |
Level of literacy among the study subjects showed that illiterates constituted 495(49.5%) whereas literates constituted 505(50.5%) subjects [Table/Fig-2].
Out of 1000 study subjects as many as 820 subjects had diminution of vision. Near vision was diminished in 68.4% (684) subjects while both near vision and distant vision were impaired in 13.6% (136) subjects. Remaining 180 subjects were emmetropic [Table/Fig-3].
| Visual acuity | Number | Percentage |
|---|
| Near vision, N8 | 684 | 68.4 |
| Reduced near and distant vision | 136 | 13.6 |
| Normal distance and near vision | 180 | 18 |
Barriers limit rural females to access the spectacles. Accordingly, the KAP questionnaire was employed to know the level of KAP about presbyopia of our subjects and also to improve our basic understanding of some of the barriers. Our cohorts had problems in threading the needle (69%), the cleaning the grains (57%), seeing digits in mobile phone (60.4%), recognizing denomination of coins (24.5%) and other household work (31.8%) whereas, 24.2% were ashamed or distressed with the problem [Table/Fig-4].
Response of the questionnaire eliciting response symptoms of presbyopia.
| Questions | Responses |
|---|
| Yes | No | Sometimes |
|---|
| Number | % | Number | % | Number | % |
|---|
| Reading news print | 492 | 49.2 | 430 | 43 | 77 | 7.7 |
| Small font in mobile | 604 | 60.4 | 306 | 30.6 | 90 | 9.0 |
| Cleaning the grains | 570 | 57 | 250 | 25 | 180 | 18 |
| Threading the needle | 690 | 69 | 231 | 23.1 | 79 | 7.9 |
| Recognizing the denomination of coins | 245 | 24.5 | 605 | 60.5 | 150 | 15 |
| Head ache | 330 | 33 | 318 | 31.8 | 352 | 35.2 |
| Other household work | 318 | 31.8 | 491 | 49.1 | 191 | 19.1 |
| Distressed/embarrassed with your problem | 242 | 24.2 | 637 | 63.7 | 121 | 12.1 |
Among our cohorts, 66.7% subjects had not heard about near vision loss, however, 86.5% of individuals thought loss of vision was age related. They approached an ophthalmologist in 7-24 months of commencement of the symptoms. Although, they thought glasses were the treatment for this condition (92.9%), while 60.2% did not prefer to use spectacles because they felt spectacles were difficult to maintain while doing household chores [Table/Fig-5].
Response of the questionnaire regarding Knowledge, Attitude and Practice (KAP) of presbyopia.
| KAP | Questions | Responses |
|---|
| Number | Percent % |
|---|
| Knowledge | Have you heard of near vision Loss? |
| Yes | 323 | 32.3 |
| No | 677 | 67.7 |
| Practice | Duration between onset of symptoms and first consultation in Months |
| 1-6 months | 111 | 11.1 |
| 7-12 months | 237 | 23.7 |
| 13-18 months | 320 | 32.0 |
| 19-24 months | 235 | 23.5 |
| 25-30 months | 22 | 2.2 |
| 31-36 months | 75 | 7.5 |
| Knowledge | Why people may lose near vision after 35 years |
| Cataract | 15 | 1.5 |
| Nerve problem | 28 | 2.8 |
| Age related | 865 | 86.5 |
| Curse of god | 1 | 1 |
| Don’t know | 91 | 9.1 |
| Knowledge | What treatment do you think will correct near vision loss? |
| Glasses | 929 | 92.9 |
| Surgery | 10 | 1 |
| Tablets | 2 | 0.2 |
| Eye drops | 2 | 0.2 |
| Not correctable | 13 | 1.3 |
| Don’t know | 44 | 4.4 |
| Attitude | Reason for not wearing glasses? |
| Lack of awareness | 101 | 10.1 |
| Felt ashamed to wear | 30 | 3 |
| Lack of felt need | 109 | 10.9 |
| Not affordable | 23 | 2.3 |
| Difficult to access | 5 | 0.5 |
| Lack of compliance/ image distortion while walking | 83 | 8.3 |
| Difficult to maintain while working | 602 | 60.2 |
| Headache | 7 | 0.7 |
| Laziness | 30 | 3 |
| Attitude | How often do you recheck once diagnosed as having near vision problem? |
| As and when required | 541 | 54.1 |
| Not necessary | 125 | 12.5 |
| Once in a year | 322 | 32.2 |
| Every month | 12 | 1.2 |
Willingness to Wear Spectacles
Among our cohorts, 86.5% knew that presbyopia is age related and 92.9% were aware that treatment of presbyopia is glasses. Despite this knowledge, they were not willing to wear the spectacles. The main reasons provided were embarrassment or feeling ashamed (3%), didn’t feel need (10.9%), distortion of images while walking (8.3%) due to glasses [Table/Fig-5].
Cost of spectacles was a factor for only 2.3% of the individuals.
In our study population, literacy was not found to be associated with the awareness of presbyopia (p=0.46) [Table/Fig-6].
Level of awareness of presbyopia with literacy status.
| Literacy status | Awareness |
|---|
| Present | Absent | Total |
|---|
| Number | % | Number | % | Number | % |
|---|
| Illiterates | 131 | 13.1 | 364 | 36.4 | 495 | 49.5 |
| Literates | 144 | 14.4 | 361 | 36.1 | 505 | 50.5 |
| Total | 275 | 27.5 | 725 | 72.5 | 1000 | 100 |
Chi sq = 0.53, DF=1, p= 0.46 > 0.05 Not Significant
Literacy has not affected the knowledge of Presbyopia
Discussion
In rural female population, presbyopia affects near work like sewing, picking rice and winnowing grain. Presently in rural areas there is an increase in use of mobiles. According to recent studies, presbyopia affects women more than men, both in prevalence and severity due to the differences in tasks performed and viewing distances [8,9]. Literacy levels among the subjects did not have significant influence on the awareness of presbyopia. Similar findings were observed in studies conducted at Ghana [10], Zanzibar [11] and Indonesia [12] among high school teachers. In their study, the major barriers for the use of glasses were poor quality of glasses [10,11,13], cost of spectacles and perception that their vision was normal. The barriers that contributed to not wearing spectacles were mainly due to lack of awareness and the modality of correction in the form of glasses as reported by Ramke J et al., from Timor Leste [8]. Lack of felt need to wear spectacles was the cause in one study from South India for not wearing spectacles [14]. Whereas spectacles was not a priority for the people from Zanzibar [11], even though spectacles are the simplest and cheapest way to correct presbyopia [15,16]. In our study, 10.9% subjects felt lack of need to wear glasses whereas 3% were ashamed of wearing glasses. Prevalence of presbyopia in our study is 82% which is higher than in African study by (63.4%) Patel IP et al., and Marmamula S et al., (63.7%) [3,14]. The higher prevalence may be attributed to the fact that our cohorts are from tertiary eye care hospital unlike the other two studies which were examined in the community.
Presentation of presbyopia is higher in 40-50 years age group, which is comparable to other studies like Andhra Pradesh Eye disease study [5] and African studies [3].
In our study, average time taken to consult an ophthalmologist was 7-24 months. The time taken to consult an ophthalmologist was delayed because of the poor literacy among females and subjects did not feel it was necessary to treat such a trivial condition. Awareness of presbyopia will ensure availability of treatment which will have a positive impact on the quality of life and productivity. It is important to educate females about the need for re-examination of visual acuity in the future even after obtaining a pair of spectacles. This would also reduce the burden of uncorrected presbyopia and promote the realization of the objectives of Vision 2020; ‘The Right to Sight’.
Marmamula S et al., from South India reports that lack of awareness and lack of need were the reasons that contributed for not wearing glasses which is similar to our study [14]. In our study, 10.9 % individuals felt lack of need to wear spectacles, however only 2.3% were unable to afford to buy spectacles. Hence, there is a need to increase the level of awareness by increasing the literacy levels and provision of affordable and high quality spectacles at the nearest place i.e., primary vision centers.
In our study, the major reason for not wearing spectacles was difficulty in maintaining glasses while working (60.2%) which is similar to a study done at Timor-Leste [8]. In other studies (African and Andhra Pradesh Eye Disease Study) [3,14], the barriers were high cost, low priority and lack of awareness. Nowadays, mobile phone is increasingly used in rural India and it requires good near vision to use them. Among our cohorts, there was statistically not significant effect of literacy and awareness of presbyopia (p=0.46). Provision of low cost, high quality reading glasses, with education about their use can be given during our regular cataract screening camps [3,10,16].
Limitation
In the present study, we have done visual acuity testing and refraction, later we employed the questionnaire before prescribing spectacles. We have not checked for the compliance and compatibility among the subjects.
Here we have only performed a questionnaire based study.
Conclusion
Prevalence of presbyopia is high among rural females. Most of the women do not wear spectacles because of poor quality glasses and difficulty in maintaining spectacles while working. There is a need for health education among rural female population about presbyopia and also provision for high quality, low cost spectacles.
Recommendations
There is a need to create health awareness in the community about presbyopia which is easily corrected by spectacles. Optometrists/Ophthalmic Technicians need to examine and correct presbyopia among population in their mid-30’s and older age groups. Additionaly, policy makers should actively include detection and management of presbyopia as a part of national eye care programmes with the provision of durable and affordable reading glasses.