In modern dentistry, it has been recognised that no cavity design or restorative material will cure caries [1]. Therefore there has been a paradigm shift in caries management from surgical intervention to minimally invasive dentistry, that is, from “extension for prevention” to “prevention of extension” [2]. In this paradigm, surgical interference is required only in that part of the tooth surface that is irreversibly broken down, while surrounding demineralised tooth surfaces which are amenable are either remineralised or lesion progression is halted.
For caries detection, most of the visual changes and radiographic changes contributing to the diagnosis come from the body of the lesion. In the incipient lesion, substantial mineral loss occurs in the underlying lesion body while the pseudo-intact enamel surface remains relatively unaltered. This is clinically significant as diagnosis is usually delayed and is typically made only after substantial mineral loss, necessitating operative intervention with significant hard tissue removal. Clinically, such active non-cavitated demineralized areas appear chalky and ‘whitish’ and are called “White Spot Lesions” (WSL) [3,4]. In theory, WSL can regress and disappear due to mechanical removal of the affected enamel or due to remineralisation procedures. However, as the cycle of demineralization and remineralization is confined to the surface and does not involve the subsurface body lesion, the WSL typically become less obvious but scarcely disappear completely [3].
A recently developed addition to the gamut of minimally invasive operative techniques is the microinvasive technique of caries resin-infiltration. It is unique in a way that unlike other minimally-invasive operative techniques, no hard tissue removal is attempted. In this technique, the body of the caries lesion is infiltrated with low-viscosity light-curing resin methyl-methacrylate. The resin occludes the pores within the lesion body, which otherwise act as diffusion pathways for acids and dissolves minerals. By impeding the internal fluid mechanics contributing to lesion progression and preventing cavitation by strengthening the enamel structure, this approach bridges the gap between non-invasive and invasive treatment options and removes the necessity of the restorative intervention or the delay and uncertainty while waiting for an active WSL to stabilize [5,6].
Deciduous and permanent teeth differ structurally in the outermost surface of enamel vis a vis the presence of an aprismatic layer and differences in the degree of mineralization [7]. It is unclear whether the penetration of resin-infiltrant in deciduous teeth would be similar to those of permanent teeth. The present study attempted to evaluate the extent of penetration of resin-infiltrants in natural WSL in deciduous molars.
Materials and Methods
This in vitro evaluation study was conducted between April 2014 and June 2014 in the Department of Paedodontics and Preventive Dentistry, Coorg Institute of Dental Sciences, Karnataka, India, after obtaining the necessary clearance from the Institutional Ethical Review Committee. Non carious deciduous molars extracted for therapeutic reasons such as space management and serial extraction were used in this study. The teeth were carefully cleaned of soft tissues and stored in saline until use. The teeth were examined under a stereomicroscope (20x, Stemi SV 11, Carl Zeiss, Oberkochen, Germany) to check for an intact superficial layer on the surface of the lesion. Teeth having macroscopic defects such as cracks, fractures, wear facets and cavitated lesions were excluded from this study at this stage. From the remaining, teeth having active WSL {non cavitated dull surface with chalky opacity, scored as ICDAS 2 (International Caries Detection and Assessment System)} on any smooth or proximal surface were selected [8]. Teeth were sectioned (Band Saw 300cl; Exakt Apparatebau, Norderstedt, Germany) across the WSL perpendicular to the tooth surface, providing two halves of each lesion. The cut surfaces were examined under stereomicroscope and lesions were sorted into four grades C1–C4 (as given by Marthaler and Germann) [9]: lesion extension confined to outer half of enamel (C1), lesion extension confined to inner half of enamel (C2), lesion extension confined to outer half of dentine (C3), lesion extension confined to inner half of dentine (C4). Lesions graded as C4 were discarded and only lesions with C1-C3 grading, with same grading in corresponding lesion halves were allocated to be treated either with infiltrant or to serve as untreated controls. A total of 50 lesion halves were allocated to two equal groups; experimental group or control group (n = 25 for each group), with respect to treatment with caries resin-infiltrant for the purpose of the study. Thereafter, cut surfaces were covered with nail varnish (Lakme, India), leaving an exposed half of the WSL surface in each sample.
In the experimental group, the targeted surfaces were treated with Icon® caries-infiltrant (DMG, Hamburg, Germany) following the manufacturer’s instructions, whereas in the control group, samples were subjected to no treatment [10]. Icon® usage involved application of Icon®-Etch syringe (15% Hydrochloric acid) for 2 minutes, followed by rinsing with water for 30 seconds and drying with oil-free and water-free air. The lesion was then desiccated using the Icon®-Dry syringe (99% ethanol) for 30 seconds followed by drying with oil-free and water free air. Icon®-Infiltrant syringe was placed on the targeted surface and caries resin-infiltrant was dispensed. After three minutes, excess infiltrant was wiped using a cotton roll and the surface was light-cured (430-490 nm, 600 mW/Cm2, LEDition, Ivoclar Vivadent, Liechtenstein) for 40 seconds. Lastly, the infiltrant was reapplied for one minute and light cured for 40 seconds.
Nail varnish was carefully removed and the treated samples were prepared to observe the penetration of resin-infiltration by fixing on object holders and parallelized (Mikroschleif system 400cs, Abrasive Paper 1200, 2400, 4000; Exakt Apparatebau, Norderstedt, Germany). Specimens were cut (Exakt 300 CL) and polished (Exakt Mikroschleifsystem 400 CS) to a uniform thickness of 100 µm and observed with cross-polarized light microscopy (Compact Polarizing Microscope CX31-P, Olympus, Tokyo, Japan). Measurements were made in micrometer using ImageJ software (National Institutes of Health, Bethesda, Maryland) measured from the enamel surface to measure LD and PD. LD was defined as the maximum linear distance from the enamel surface to the deepest front of negative birefringence indicative of the advancing front of WSL demineralization, PD was defined as the maximum linear distance from the enamel surface to the deepest front of positive birefringence indicative of reduction in pore volume by occlusion with resin.
Statistical Analysis
SPSS (SPSS Inc., Released 2009. PASW Statistics for Windows, Version 18.0. Chicago, IL, USA) was used for computing means (with standard deviation) of LD and PD.
Results
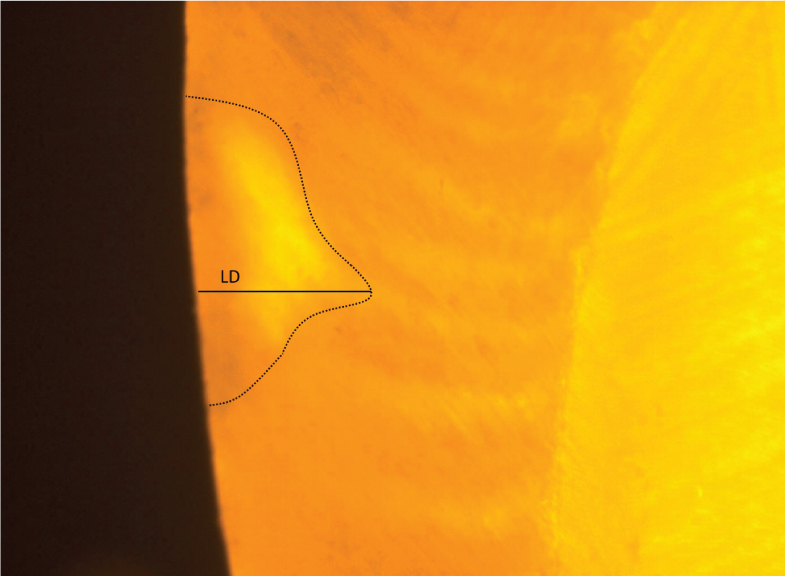
Images were analysed based on the optical characteristics of the specimens. Samples displayed varying refringence under cross-polarized light between infiltrated and un-infiltrated areas due to differences in refractivity owing to the imbibition of the resin. Mean LD (± standard deviation) for all samples (n=50) was 367 (±182) µm. PD varied within the experimental group (n=25) and mean PD (± standard deviation) was 352 (±141) µm. In the control group consisting of untreated samples (n=25), no acid-etching or resin penetration was attempted. WSL with typical pseudointact surface layer with variable degree of subsurface demineralization were seen [Table/Fig-1].
Representative image of untreated lesion (sorted as C1) showing pseudointact surface and subsurface demineralization with lesion depth (LD – dotted line).
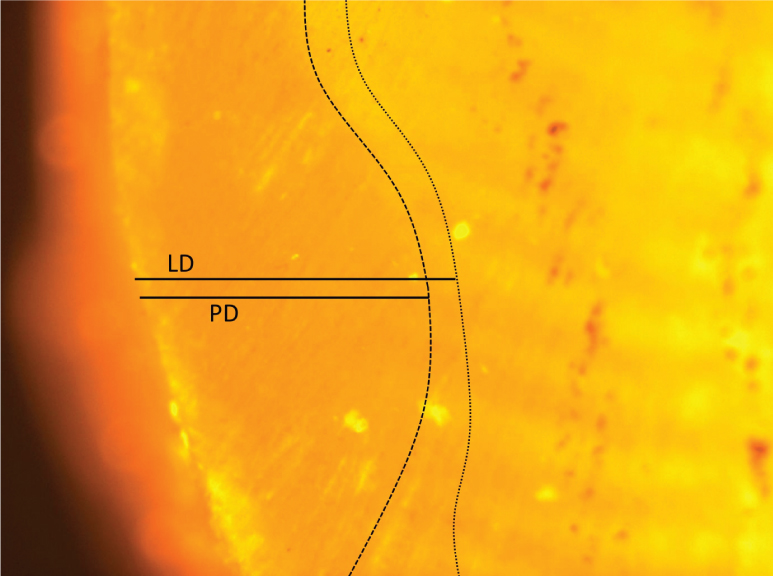
All samples of the experimental group showed resin penetration to varying degrees. Of these, 72% (n=18) of samples were observed to have resin penetrating nearly entire extent of the lesion [Table/Fig-2].
Representative image of lesion treated with infiltrant; lesion depth (LD – dotted line) and penetration depth (PD – dashed line) showing nearly complete resin penetration.
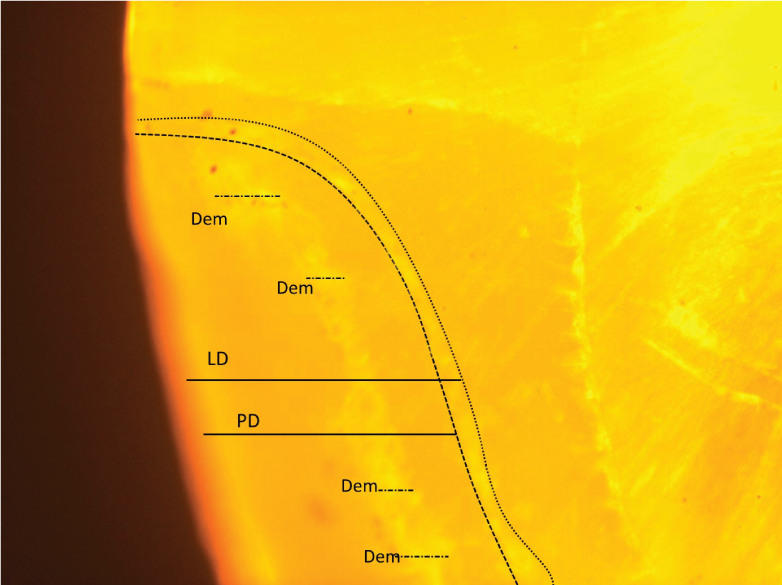
Whereas 28% (n=7), revealed resin penetration with scattered areas of demineralization [Table/Fig-3].
Representative image of lesion treated with infiltrant showing lesion depth (LD – dotted line) and penetration depth (PD – dashed line) with scattered areas of demineralization (Dem – dots and dash).
Discussion
A significant proportion of children show increased incidences of proximal decay and also faster progression following lesion initiation as these are plaque retentive sites [11,12].
Plaque control, fluorides, pit and fissure sealants and remineralizing agents have been recommended to arrest the caries process in the non cavitated lesion. However, dental compliance is a known issue with children and adolescents, often leading to lesion cavitation. Once cavitated, minimal intervention restorative strategies are recommended but these still may introduce the tooth to the restorative spiral. Caries infiltration is a novel strategy that improves on the minimal intervention concept, since the intervention is on the microinvasive scale. The technique delays restorative intervention, reduces the risk of postoperative sensitivity and pulpal inflammation and improves aesthetic outcomes when used as a masking resin on demineralised labial surfaces such as those seen in orthodontic patients [1,13,14]. Compared to its closest predecessor amongst preventive restorative techniques i.e. pit and fissure sealing, the resin layer is established on the superficial layer of enamel of the pit and fissures, whereas in the infiltration technique a low viscosity resin-infiltrant is soaked into the porous lesion body, in the proximal or cervical surfaces, replacing the lost mineral with resin [2,15-18]. This technique has advantages such as the absence of margins on the tooth surface that could enhance plaque accumulation and cause periodontal inflammation and also strengthens the lesion mechanically thereby preventing further destruction [17].
Our study showed that Icon® infiltrant is capable of penetrating several hundred micrometres into natural carious lesions, when employed as per manufacturer’s instructions on deciduous teeth making the Icon® system a valuable tool over other non invasive modalities to deal with WSL. Such results are in agreement with the literature available utilizing resin-infiltrants in WSL on permanent teeth, which describe the considerable variation in penetration depths [18].
Paris S et al., evaluated the effect of phosphoric acid and hydrochloric acid gels on the surface layer reduction of natural lesions of deciduous teeth [19]. This step to effectively degrade the highly mineralized surface layer was deemed important to achieve high penetration depths by the resin-infiltrant. They were of the opinion that the effects of prismless enamel were of subordinate importance when pretreating enamel surface with 15% hydrochloric acid gel. In our study, all experimental group samples showed penetration, with PD comparable to those found by other investigators working with WSL on permanent teeth [5,15,16,20] and deciduous teeth [19,21-23]. suggesting that etching and penetration is unhampered by structural differences between deciduous and permanent teeth enamel.
Paris et al., in a study comparing the penetration of Icon® infiltrant into natural WSL of deciduous molars after different infiltrant application times concluded that one minute application was sufficient but three minute application time should be recommended to infiltrate deep proximal WSL in deciduous molars [23]. A similar study by Paris et al., with experimental infiltrants found five minute application to infiltrate WSL in deciduous molars nearly completely [21]. A study by Soviero VM et al., found one minute application to give penetration similar to five minute applications [22]. In the present study, three minute application yielded varying depths of penetration which may be due to the variation in the depth of the lesion in the teeth selected. The resin-infiltration system Icon® thus provides an effective ‘bridge’ between non LD invasive and minimally invasive treatment. It was found to be effective in deciduous teeth, in addition to its established use in permanent teeth.
Limitation
The present study is a modest approach examining the performance of resin-infiltrants in deciduous teeth. An in vitro design utilizing ‘naturally occurring’ WSL was the closest to approximate the intraoral conditions. However, it is prudent to note that the in vitro design is the major limitation as the material’s performance may vary from actual in vivo performance. This is due to the dynamic cycle of remineralization and demineralization occurring in vivo condition continuously at the highly mineralised pseudointact surface layer, which in turn influences the initial penetration of resin. Also, the pores of WSL in vivo would be continuously contaminated with organic materials resulting in lower pore-volume hampering resin penetration. Also, we were constrained by the availability of fluorescence imaging techniques which would have enabled differential staining of areas. Future investigators may beneficially employ such techniques.
Conclusion
The resin-infiltration system Icon® was found to be effective under in vitro conditions in deeply and predictably infiltrating the enamel porosities of natural WSL on smooth or proximal surfaces of deciduous molars. Icon® can be useful as a valuable tool for the restorative dentist to arrest and restore incipient lesions.