Axial Torsion of Meckel’s Diverticulum: A Rare Case Report
Sandesh Vithal Parab1, Pramod Govindrao Salve2, Aruna Dahiphale3, Rupesh Thakare4, Amit Aiwale5
1 Resident, Department of General Surgery, SRTR Government Medical College, Ambajogai, Mumbai, Maharashtra, India.
2 Assistant Professor, Department of General Surgery, SRTR Government Medical College, Ambajogai, Mumbai, Maharashtra, India.
3 Resident, Department of General Surgery, SRTR Government Medical College, Ambajogai, Mumbai, Maharashtra, India.
4 Resident, Department of General Surgery, SRTR Government Medical College, Ambajogai, Mumbai, Maharashtra, India.
5 Resident, Department of General Surgery, SRTR Government Medical College, Ambajogai, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sandesh Vithal Parab, D/606, Sai Asha CHS, Gavanpada, Mulund East, Mumbai-400081, Maharashtra, India.
E-mail: sandy17187@yahoo.co.in
Meckel’s Diverticulum (MD) is the most common congenital anomaly of gastrointestinal tract, occurring in 2% of the population. It is a true diverticulum and histologically all four intestinal layers are present within MD. There are various complications related to a Meckel’s diverticulum, including haemorrhage, intestinal obstruction, inflammation and perforation. Axial torsion followed by gangrene of MD is the rarest of the complications that have been reported. The exact mechanism for torsion is unclear. Preoperative diagnosis of torsion of MD is difficult and often confused with appendicitis as pain is usually localized to right lower quadrant. Radiological investigations do not provide much help in diagnosis. We report a case of axial torsion of MD presenting as acute abdomen in an 11-year-old female patient. The diagnostic laparoscopy was performed. Confirmatory diagnosis and further surgical management was done by exploratory laparotomy under general anaesthesia.
Acute abdomen, Exploratory laparotomy, Intestinal obstruction
Case Report
An 11-year-old female child presented in emergency room with acute, severe abdominal pain. An examination of the patient revealed that she had a distended abdomen with rebound tenderness in hypogastrium and right iliac fossa. Her rectal examination was unremarkable. Her blood test revealed raised leukocytes count (15,000/μl), normal renal function and a normal haemoglobin level. An abdominal radiograph revealed dilated small bowel loops and a clinical diagnosis of perforated acute appendicitis was made. No other preoperative radiological investigations were carried out and following fluid resuscitation, laparoscopy was performed.
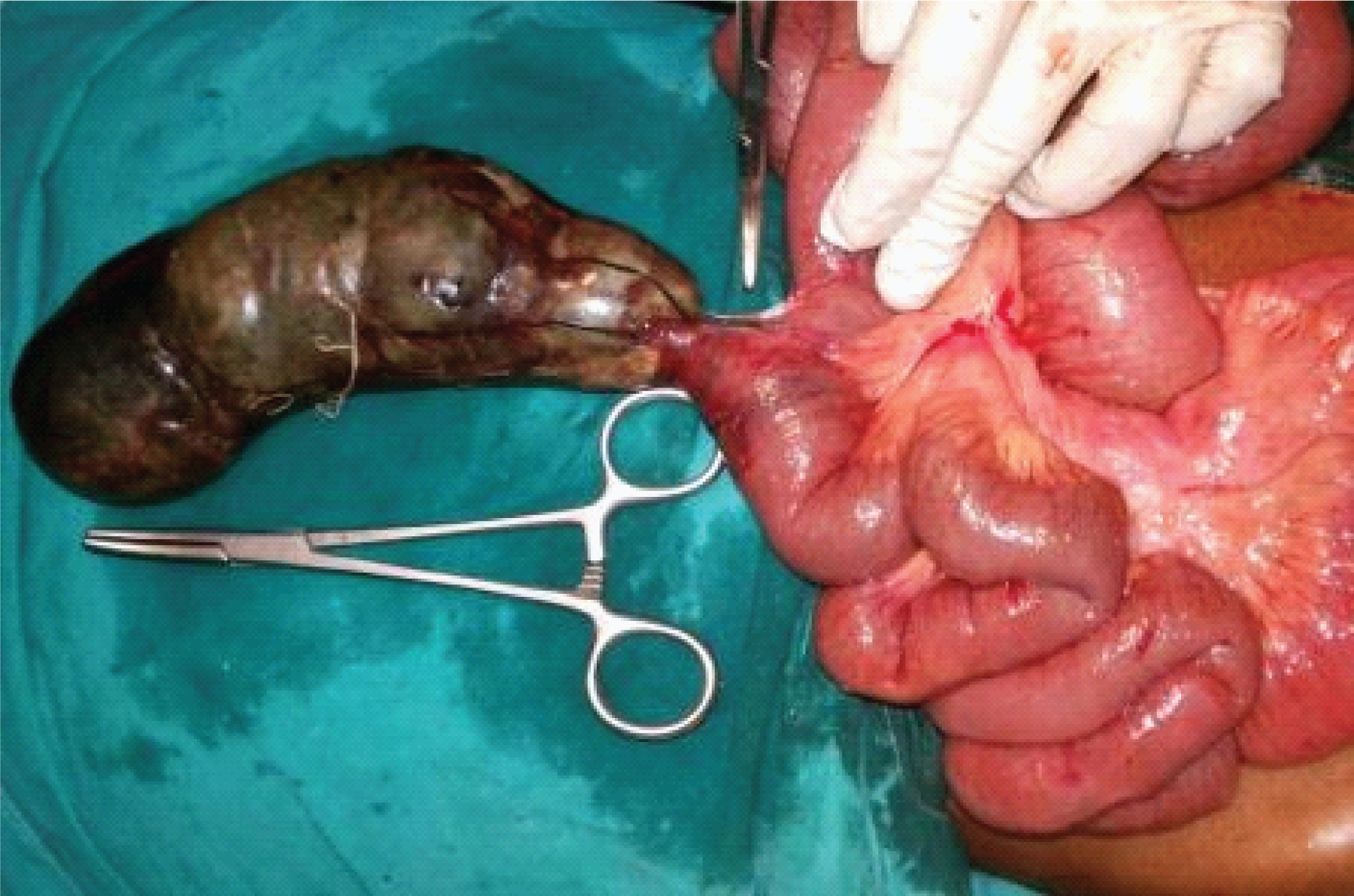
Laparoscopy revealed haemorrhagic fluid within the pelvis. The appendix could not be visualized, but gangrenous loop of intestine was visualized which was not handled laparoscopically then the laparoscopy was converted to a laparotomy. Surgical exploration revealed a torted and distended MD with gangrenous changes throughout its length [Table/Fig-1]. The appendix and the rest of the bowel appeared to be normal. The twisted MD was resected along with 10 cm length of ileum that was adjacent to base of gangrenous MD and end-to-end seromuscular, double layered anastomosis using a 3-0 non-absorbable suture was performed to restore the continuity of the small bowel. Thorough washout of the peritoneal cavity was performed and a pelvic drain was inserted. The patient’s recovery was uncomplicated and she was discharged on 10th postoperative day with routine follow up.
Axially Torted MD with Gangrenous changes.
Discussion
MD results from incomplete obliteration of the most proximal portion of the vitelline duct [1]. Though MD is the most common anomaly of GI tract, its axial torsion is one of the rare complications. It occurs due to its twisting around its axis [2]. It is defined as rotation of MD along its axis at its base without involvement of attached ileal loop or ileal mesentery, which may lead to compromise of its vascular supply and eventually leading to its gangrene. In this case report, we are discussing such rare case of axial torsion of MD.
There are many factors associated with axial torsion of MD but the mechanisms underlying isolated torsion of MD is still elusive. Attachment of distal end of MD to umbilicus due to retained fibrous vitelline band increases the chances of MD torsion [3]. MD may be attached to ileal mesentery. The anatomical specifications of MD such as length and breadth of MD and base diameter of MD are important predisposing factors. Risk of torsion increases with longer and larger MD with its narrow base [1,4,5]. In our patient, axial torsion of MD occurred around its narrow base and length of MD was 15 cm. Another potential risk factor is primary neoplasm arising within MD, which is very rare situation [6].
Pain mostly localized to right lower quadrant of abdomen is a common presenting symptom in case of torsion of MD. Duration of pain may vary [7]. If torted MD becomes gangrenous or gets perforated, signs of peritonitis as well as sepsis may be present. Hence, in such cases, provisional diagnosis as complication of MD is usually missed. Appendicitis, small bowel obstruction, cholecystitis and amoebic liver abscess are some of the incorrect provisional diagnoses. Mobility of MD could be the reason of such misdiagnoses. In our case, provisional diagnosis was acute appendicitis.
Abdominal radiograph may be normal or may show signs of bowel obstruction or sometimes perforation. The patient’s radiograph in our case report had features of bowel obstruction. When there is torsion of MD on Ultrasonography (USG), it appears as cystic, tube like non peristaltic structure [8]. USG is mainly useful for excluding other pathology. CT scan abdomen could be misleading in cases of torsion of MD.
In our case, we ruled out other pathologies with the help of diagnostic laparoscopy and performed exploratory laparotomy and resected ileal loop with gangrenous MD followed by primary anastomosis. Diagnostic laparoscopy is also useful to avoid delayed surgery carrying substantial risk.
Conclusion
Torsion of MD is an extremely rare complication. An enlarged MD along with its narrow base could be risk factor for torsion of MD. It is difficult to diagnose torsion of MD with the help of imaging alone. Hence, it is important to have high clinical suspicion for involvement of MD and to confirm the diagnosis by doing exploratory laparotomy. Treatment of choice for such cases is surgical excision of diseased MD.
[1]. Limas C, Seretis K, Soultanidis C, Anagnostoulis S, Axial torsion and gangrene of a giant Meckel’s diverticulumJ Gastrointestin Liver Dis 2006 15:67-68. [Google Scholar]
[2]. Guss DA, Hoyt DB, Axial volvulus of Meckel’s diverticulum: a rare cause of acute abdominal painAnn Emerg Med 1987 16:811-12. [Google Scholar]
[3]. Moore GP, Burkle FM, Isolated axial volvulus of a Meckel’s diverticulumAm J Emerg Med 1988 6:137-42. [Google Scholar]
[4]. Tan YM, Zheng ZX, Recurrent torsion of a giant Meckel’s diverticulumDig Dis Sci 2005 50:1285-87. [Google Scholar]
[5]. Toshihiko W, Hirofumi O, Two cases of Meckel’s diverticulum torsionJpn J Gastroenterol Surg 2002 35:180-83. [Google Scholar]
[6]. Almagro UA, Erickson L Jr, Fibroma in Meckel’s diverticulum: a case associated with axial and ileal volvulusAm J Gastroenterol 1982 77:477-80. [Google Scholar]
[7]. Mackey WC, Dineen P, A fifty year experience with Meckel’s diverticulumSurg Gynecol Obstet 1983 156:56-64. [Google Scholar]
[8]. Gallego-Herrero C, del Pozo-Garcia G, Marín-Rodriguez C, Ibarrola de Andrés C, Torsion of a Meckel’s diverticulum: sonographic findingsPediatr Radiol 1998 28:599-601. [Google Scholar]