Case Report
A 40 year-old-male with a history of road traffic accident one week back was admitted in Kempegowda Institute of Medical Science, Bengaluru, India, with a chief complaint of pain all over his face following trauma. There was no history of loss of consciousness, vomiting and seizures. Patient was conscious, cooperative and well oriented; with a Glasgow coma scale score of 15. Patient was referred to the Department of Oral and Maxillofacial Surgery, Vokkaligara Sangha Dental College, Bengaluru, India, for further evaluation. On clinical examination, the patient had gross facial edema, bilateral subconjunctival ecchymosis and severe chemosis in the left eye. Both pupils were equally reactive to light, extraocular movements were normal. Intraoral examination revealed mouth opening to be 1 cm, occlusion deranged and segmental mobility found in the anterior region. A faciomaxillary CT scan was done for better evaluation of the facial fracture [Table/Fig-1].
3D reconstruction CT, showing pan facial fracture involving upper, middle, and lower third of the face.
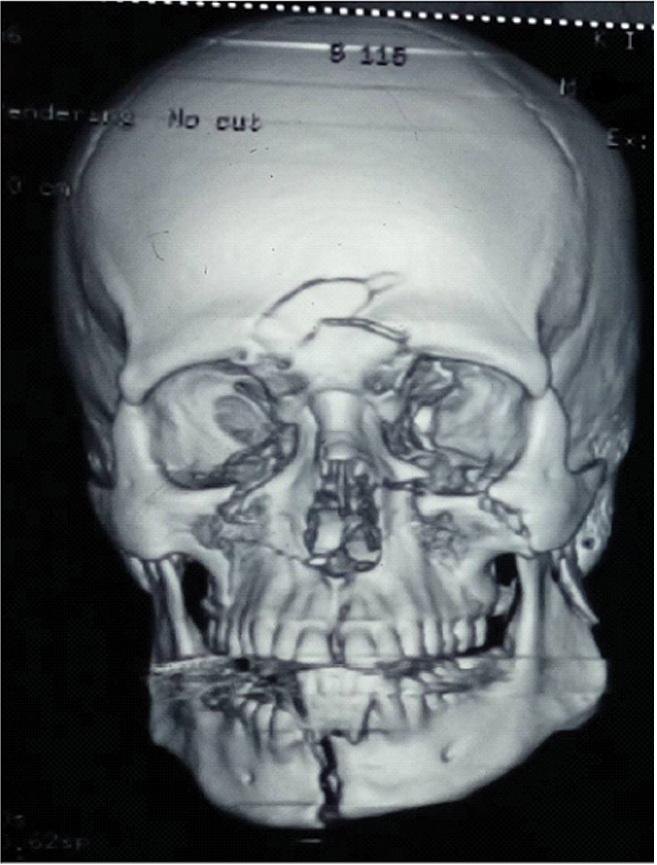
The patient was diagnosed with pan facial fracture as there were fractures involving upper, middle and lower third of the face. The patient had frontal bone fracture, bilateral zygomaticomaxillary orbital complex fracture and mandibular symphysis fracture. The treatment plan was open reduction and internal fixation with Stainless Steel (SS) miniplates under general anaesthesia. Written informed consent was taken from the patient. Preoperative routine blood investigations were within normal limits and physician, neurosurgeons and ophthalmologist clearance was also taken before surgery. General anesthesia was induced via IV route. The mandibular fracture was first reduced, stabilised and fixed with 2 mm plates (four hole with gap SS plates). Then the left orbital floor was addressed; a transconjuctival incision was given and after dissecting in layers, the floor was visualised. It was noticed that the fracture was not comminuted and hence was left as it is. The left infraorbital rim fracture and zygomaticomaxillary buttress were approached through intraoral Keen’s incision and were reduced and stabilized by 1.5 mm SS four hole with gap orbital miniplate, SS L plate and a SS two hole with gap miniplate. Left side nasomaxillary buttress fracture was undisplaced and fixed using a SS two-hole with gap straight miniplate. Right zygomaticomaxillary complex was approached through intraoral Keen’s incision as well; right zygomaticomaxillary buttress fracture was identified, reduced and fixed using a SS L - miniplate and a two-hole straight miniplate.
While manipulating the left globe and ocular muscle, there was a sudden drop in heart rate of the patient upto 39 beats per minute. Manipulation was stopped for a while and atropine was injected intravenously, after few seconds the heart beat returned to normal and reduction, fixation and stabilization of inferior orbital rim was done. Then the left zygomaticomaxillary complex fracture was addressed. Intraoral incision was given to visualize the zygomaticomaxillary complex, while reducing the fractured fragments, again a drop of heart beat was seen. The time duration between the two episode was around 30 minutes. Manipulation was stopped and the heart rate returned to normal. Only stopping of manipulation was enough to bring the heart rate to normal, so administration of atropine was not required. Then left zygomaticomaxillay complex fracture was fixed. There are only handful of case reports on trigeminocardiac reflex occurring twice in a pan facial frature surgery. Postoperatively vitals of the patient were within normal limits.
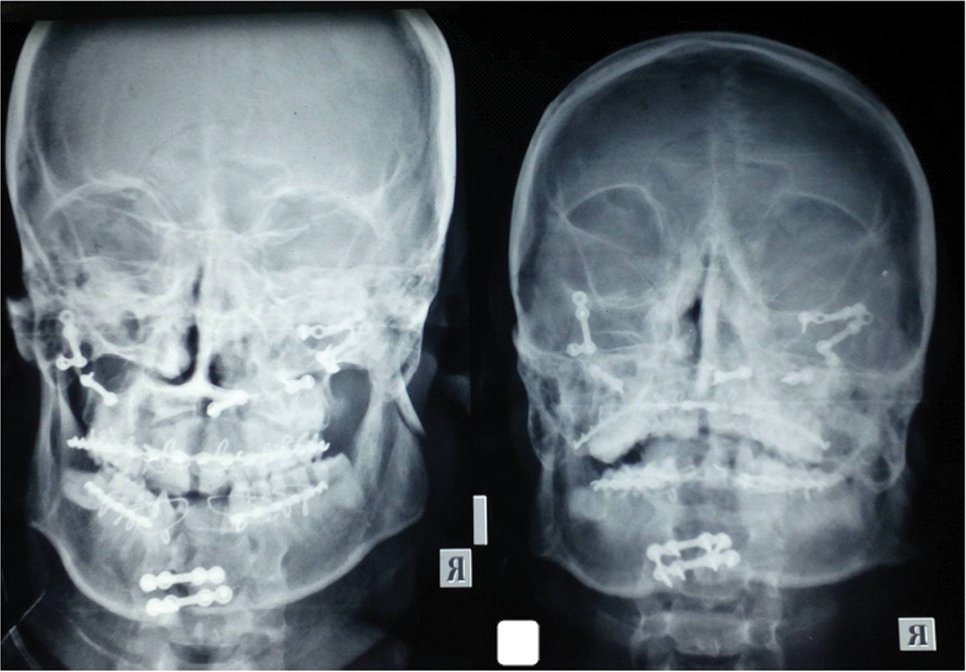
[Table/Fig-2] shows the postoperative posterioanterior view of mandible and paranasal sinus view depicts management of fractures with stainless steel plates.
Postoperative PA view of mandible and PNS view shows management of fractures with stainless steel plates.
Discussion
Trigeminocardiac reflex is defined as sudden onset of sinus bradycardia, heart rate less than 60 beats per minute and mean arterial blood pressure less than 20% of baseline. Few authors have also stated that reduction of 10% or more in the heart rate can be considered as positive trigeminocardiac reflex [1]. The occulocardiac reflex is a well established phenomenon that classically includes bradycardia along with nausea, bradypnoea, gastric hypermobility and syncope. Trigeminocardiac reflex is the sudden onset of relative bradycardia upon stimulation of any of the three branches of trigeminal nerve [2]. Trigeminocardiac reflex was previously called as oculocardiacreflex, a term given by Bernhard Aschner and Giuseppe Dagnini in the year 1908, so it is also called Aschner phenomenon [3]. This reflex, according to them, was elicited only as a result of physical stimulation of ocular and periocular structure innervated by the ophthalmic nerve, which is a division of trigeminal nerve. The accepted mechanism for occurrence of trigeminocardiac reflex is that when any mechanical manipulation, stretching, pressure effect happens on any of the three branches or peripheral branches, the sensory nerve endings of the trigeminal nerve send impulse via Gasserian ganglion to the sensory nucleus of the trigeminal nerve forming the efferent pathway [3]. The afferent arm is connected to the efferent arm via short internuncial fibers in the reticular formation and connecting the visceral motor nuclei of the vagus nerve [1]. After this, the signal passes through the rostral ventral lateral and intermediate ventral lateral region of the medulla and onto the dorsolateral pons. The impulse proceeds through the intermediolateral cell column of the spinal cord, delivering the signal via nerve of vagus origin to the active end organ like heart and stomach [4]. These impulses increase the parasympathetic activity of heart and gastrointestinal system [5]. The efferent pathway travels along the vagus nerve via cardiovascular centre of the medulla to sinoatrial node [6]. The efferent pathway travels and ends in the 2muscuranic receptor of the heart causing vagus mediated negative chronotrophic and ionotrophic effects of the heart. The efferent limb also connects to the stomach which increases the gastric motility [7]. Trigeminocardiac reflex is internal process of the body to prevent oxygen desaturation of the brain [2]. Sympathetic nerves are stimulated which leads to increased blood flow, but it can lead to decreased blood flow in the heart leading to asysytole and ventricular arrhythmia [7]. Stimulation of this reflex can precipitate sudden onset sinus bradycardia, bradycardia terminating as systole, asystole with no preceding bradycardia and hypotension [3]. There are two types of trigeminocardiac reflex, central and peripheral. The central type is induced by stimulation of the Gasserian ganglion, which causes bradycardia, apnoea and hypotension. The peripheral type has three subtypes, oculocardiacreflex, maxilla-mandibular cardiac reflex (both inducing bradycardia, apnoea and normotension) and the third type is a diving reflex stimulated by the anterior ethmoidal nerve inducing bradycardia, apnea and hypertension [2].
The predisposing and risk factors for trigeminocardiac reflex are children, males, high sympathetic activity, hypoxemia, hypercarbia, light anaesthesia, neuromuscular blocker, opioid, beta adrenergic blockers, strength and duration of stimulus likelihood through sympathetic inhibition and vagal augmentation, calcium channel blockers, clonidine, digoxin, anticonvulsants, lithium, other agents which may cause bradycardia [4,6,7]. Metabolic derangement such as hypoxia, hypothermia, acidosis, hyperkalemia, hypercalcemia, endocrinologic disturbances like hypothyroid state may instigate this reflex. Other causes for bradycardia could be due to traumatic head injury, one of the signs of cushings triad, during increase intracranial pressure, haemorrhage, compression of cerebellar vermis which may cause decrease sympathetic activity, in cervical spinal cord injury [4].
Classification of facial surgeries, according to their rate of incidence of trigeminocardiac reflex was classified by Lubbers HT et al., into low risk (temporo-mandibular joint surgeries, Le fort I osteotomy, elevation of zygoma), medium risk (skull base surgeries), high risk surgeries (ophthalmic surgeries, orbital exenteration and orbit fracture in children with cardiac disease [8]. Incidence of trigeminocardiac reflex may also occur with any oral surgical procedure and hence its importance should not be under estimated. Arasho B et al., had summarised the management of trigeminocardiac reflex as follows: 1. Risk factor identification, 2. Pre-emptive therapy with vagolytic/ or peripheral nerve blocks in procedures involving manipulation of trigeminal nerve, 3. Cardiovascular monitoring during anaesthesia [1]. According to a retrospective study of five years conducted by Shanab HG and Albargi HH, to evaluate the incidence of trigeminocardiac reflex during maxillofacial surgery, it was found in 20% of all maxillofacial surgery and was mostly seen mild facial trauma repair followed by upper face reconstruction surgeries [2]. Langs S et al., in a case series described the maxillary and mandibular variant of trigeminocardiac reflex [9]. Another variant of trigeminocardiac reflex described in a case report by Haldar R et al., is a nasocardiac reflex which was elicited after placement of nasogastric tube, the heart rate decreased drastically from 94 to 42 beats per minutes [10]. Arakeri G et al., proposed a hypothesis, that trigeminocardiac reflex may mediate syncope (vagal reaction) during extraction of maxillary first molar under local anesthesia and named this relex as dentocardiac reflex, which points towards the site of trigger [11]. In a study, it was seen that there was a decrease in heart rate in mid-face trauma during the initial examination and also during the surgical correction, although the condition got corrected after termination of the treatment in most patients but in two patients bradycardia progressed to asystole in whom atropine was administered [3]. In a case report documented by Cha ST et al., two episodes of trigeminocardiac reflex was seen during operating procedure of intracranial hemangioma, these episodes were seen during transection of the sensory root of trigeminal nerve [12].
Maxillofacial surgeons should be abreast in the signs of trigeminocardiac reflex, which may be disastrous at times. So a proper management should be done [3]. Sudden and prolonged traction of craniofacial structures should be refrained [1]. Regional nerve block should be given in the operating site, mostly in cases where hypotensive anesthesia is planned. Administration of vagolytic agents like atropine and local anesthetics like lignocaine can be prophylactically administered. Adequate oxygenation, watching for additional CO2 waves and constant cardiac monitoring should be done. If trigeminocardiac reflex is found to be activated, abstainence of the stimulus and administration of anticholinergics like glycopyrolate should be done. If trigeminocardiac reflex is not managed with vagolytic drugs then epinephrine should be administered. Cardiac massage is reserved for cases who does not respond satisfactorily with the above treatment [7]. In a case reported by Prabhakar H et al., severe cardiac depression and hypotension was noted during craniotomy for parietal convexity meningioma in a 48 year old female patient. Atropine was not useful in this case and hence epineprine was administered which acts on alpha 1 adrenoceptors, causing vasoconstriction thus increasing the heart rate and cardiac output thereby reducing blood supply [13].
Transphenoidal surgery [2], cerebropontine angle tumor surgeries [1], skull base lesions [1,2,12], giant chronic subdural hematoma removal [2], transection of sensory root of the trigeminal nerve (rhizotomy), craniofacial reconstruction (craniofacial reconstruction with mandibulofacial disostosis) [2], trauma (mid face disimpactions, elevation of zygomatic arch fracture, nasoethmoid fracture reduction, pan facial fracture [2], orbital floor trapdoor fracture with incarcerated orbital soft tissue in the maxillary sinus and or entrapment of inferior rectus muscle, periorbital laceration manipulation, zygomaticomaxillary complex fracture with temporal artery laceration), orthognatic surgeries, temperomandibular surgeries, cosmetic surgeries (blepharoplasty, orbital reconstruction, endoscopic forehead lift surgeries), dentoalveolar procedure (extraction of maxillary molars, mesiodens removal, mandibular exostosis), iatrogenic cause like insertion of balloon nasal catheter cause elicited oculocardiac reflex by direct compression of eye ball [1,2,5,11,14].
Various complications may occur following trigeminocardiac reflex. Outcome from the reflex can sometime be dreadful and may lead to lifelong disabilities due to ischemic complications, in patients with poor vascularity due to atherosclerosis or tumour encasement which may lead to subsequent cardiac and cerebral infarctions mainly due to rapid drop in arterial blood pressure [1,2]. It has also been shown that patient developing this reflex has higher chances of having hearing function deficit who are operated for vestibular schwannoma which occurs mostly due to decrease in blood pressure [1]. One report indicated that there were 60 deaths from trigeminocardiac reflex [2].
Conclusion
It is essential for a prudent maxillofacial surgeons to know about this sudden physiologic response, which may occur from a minor or major surgical procedure. A good knowledge about trigeminocardiac reflex is essential for proper management and correct initiatives can prevent untoward complications and morbidities. Whenever trigeminocardiac reflex is anticipated during any maxillofacial surgery a collaborative effort of maxillofacial surgeons and anaesthesiologists is mandatory and life-saving.
[1]. Arasho B, Sandu N, Spiriev T, Prabhakar H, Schaller B, Management of the trigeminocardiac reflex: Facts and own experienceNeurology India 2009 57(4):375-80. [Google Scholar]
[2]. Shanab HG, Albargi HH, Incidence of trigeminocardiac reflex in maxillofacial surgery: A retrospective studyJ Health Spec 2016 4(2):151-56. [Google Scholar]
[3]. Joshi UM, Munnangi A, Shah K, Patil SG, Thakur N, Trigemino-cardiac reflex: A phenomenon neglected in maxillofacial surgery?Journal of Maxillofacial and Oral Surgery 2017 16(2):181-85. [Google Scholar]
[4]. Jackson BF, Orbital trauma, bradycardia, and vomiting: trapdoor fracture and the oculocardiac reflex: a case reportPediatric Emergency Care 2010 26(2):143-45. [Google Scholar]
[5]. Joseph JM, Rosenberg C, Zoumalan CI, Zoumalan RA, White M, Lisman RD, Oculocardiac reflex associated with a large orbital floor fractureOphthal Plast Reconstr Surg 2009 25(6):496-97. [Google Scholar]
[6]. Van Noord BA, Zhao M, Asystole during vitrectomy secondary to increasing intraocular infusion pressure transmitted via sclerotomy infusion cannulaJ Anesthe Clinic Res 2012 3(3):198 [Google Scholar]
[7]. Devakumari S, Vijhayapriya T, Trigemino cardiac reflex and its importance in maxillofacial surgery- a reviewIOSR Journal of Dental and Medical Sciences 2013 2(2):07-11. [Google Scholar]
[8]. Lubbers HT, Zweifel D, Gratz KW, Kruse A, Classification of potential risk factors for trigeminocardiac reflex in craniomaxillofacial surgeryJ Oral Maxillofac Surg 2010 68(6):1317-21. [Google Scholar]
[9]. Lang S, Lanigan DT, van der Wal M, Trigeminocardiac reflexes: maxillary and mandibular variants of the oculocardiac reflexCan J Anaesth 1991 Sep38(6):757-60. [Google Scholar]
[10]. Haldar R, Kaur J, Bajwa SJ, Nasocardiac reflex during aspiration and injection through a nasogastric tube: An infrequent occurrenceIndian J Crit Care Med 2015 19:237-39. [Google Scholar]
[11]. Arakeri G, Raghuram CG, Reddy S, Arali V, Arakeri’s reflex: An alternative pathway for dento-cardiac reflex mediated syncopeDent Hypotheses 2010 1:09-12. [Google Scholar]
[12]. Cha ST, Eby JB, Katzen JT, Shahinian HK, Trigeminocardiac reflex: a unique case of recurrent asystole during bilateral trigeminal sensory root rhizotomyJ Craniomaxillofac Surg 2002 30(2):108-11. [Google Scholar]
[13]. Prabhakar H, Ali Z, Rath GP, Trigemino-cardiac reflex may be refractory to conventional management in adultsActa Neurochir (Wien) 2008 May150(5):509-10. [Google Scholar]
[14]. Stathopoulos P, Mezitis M, Kostakis G, Rallis G, Iatrogenic oculocardiac reflex in a patient with head injuryCraniomaxillofac Trauma Reconstruction 2012 5:235-38. [Google Scholar]