Introduction
Oil pulling, has been extensively used as traditional Indian folk remedy since many years to prevent dental diseases and for strengthening teeth and gums.
Aim
To compare and evaluate antiplaque efficacy of coconut oil pulling with a placebo among dental students, in Hyderabad city of India.
Materials and Methods
A randomized controlled study was carried out among 40 dental students. Out of 40, 20 subjects were randomly assigned to study group and other 20 to control group. Subjects in the study group were given the coconut oil and control group a placebo, and advised to rinse for 10 minutes, once daily in the morning for a period of seven days. Plaque levels were assessed on day zero, third and seventh day using Turesky-Gilmore-Glickman Modification of the Quigley-Hein Plaque Index (1970) for both the groups.
Results
The mean plaque scores showed a significant difference at baseline, third day and seventh day among both study (p<0.001) and control groups (p<0.001). Group wise comparison revealed, though the mean plaque scores were low among study group on third day and seventh day on comparison with the control group, significant difference was noticed only on the seventh day. Furthermore, the mean percentage reduction of plaque scores were also significant only on the seventh day with a high mean plaque reduction among study groups (p<0.001).
Conclusion
Oil pulling is effective in controlling plaque levels.
Introduction
Oral health is a fundamental and integral part of the general health and is considered as a prime importance to all individuals [1].World Health Organization (WHO) defined oral health as a state of being free from chronic mouth and facial pain, oral and throat cancer, oral sores, birth defects such as cleft lip and palate, periodontal (gum) disease, tooth decay and tooth loss, and other diseases and disorders that affect the oral cavity [2].
There are several risk factors for oral diseases like poor oral hygiene, unhealthy diet, tobacco use and alcohol use [3]. Inadequate oral hygiene contributes to the development of dental plaque. Dental plaque is a specific, highly variable structural entity consisting of microorganisms and their products which are embedded in a highly organized intracellular matrix [4]. Dental caries and periodontal diseases are the two globally leading oral afflictions which can be effectively prevented and controlled by an effective plaque control method [5,6].
Mechanical tooth cleaning even today remains the most dependable method for effective plaque control. Apart from mechanical tooth cleaning, research has focused on chemotherapeutic agents for reducing or preventing plaque induced oral diseases [5]. Among several chemotherapeutic agents, chlorhexidine was gold standard clinical adjunct in the treatment of both caries and periodontal diseases, but it has certain disadvantages like unpleasant taste, tooth staining and alterations in taste sensations [7]. In order to overcome these problems several other alternatives have been put forward, among that oil pulling procedure is the one which has no side effects and is readily available in the household.
Oil pulling, a traditional folk remedy that has been extensively used for many years to strengthen teeth, gums and jaws, to prevent decay, oral malodor, dryness of throat and cracked lips [8]. The concept of oil pulling was mentioned as Kavala Gandoosha/Kavala Graha in Ayurvedic text charakasamhita and was claimed to cure about 30 systemic diseases including headache, migrane, thrombosis, eczema, intestinal infection, diabetes and asthma [9,10].
Dr. F Karach was the person who familiarized the concept of oil pulling in the 1990s in Russia [11]. Edible oils like coconut oil, corn oil, rice bran oil, palm oil, sesame oil, sunflower oil, and soya bean oil has been used for oil pulling therapy including liquids from milk and water to extracts of gooseberries and mangoes [5].Coconut oil is different from other oils due to its predominant composition of medium chain fatty acid rather than long chain fatty acids which might influence the physical and chemical properties of the oil [12]. In India, coconut oil is used for food preparation and Ayurveda medicine and is described as fruit of aspiration [13].
Coconut oil contains 92% saturated acids, approximately 50% of which is lauric acid [12]. Lauric acid has proven antibacterial and antifungal effects [14]. Evidence showed that coconut oil has significant antimicrobial activity against Escherichia vulneris, Enterobcater spp., Helicobacter pylori, Staphylococcus aureus, Candida spp., including C. albicans, C. glabrata, C. tropicalis, C. parapsilosis, C. stellatoidea and C. krusei [10]. Studies proved that coconut oil is also affective against S. mutans and C. albicans in an in vitro oral biofilm model [10]. The exact antibacterial action of coconut oil still unclear, but it was hypothesized that manolaurin and other medium chain fatty acids have the capacity to alter bacterial cell wall, penetrate and disrupt cell membranes, inhibit enzymes involved in energy production and nutrient transfer, causing death of the bacteria [10]. Besides the health and nutritional benefits, coconut oil has been shown to have anticarcinogenic effects against colon tumours [15].
In a developing country like India where majority of the population resides in rural area having limited access to rural healthcare and preventive services. Coconut oil pulling would be helpful to maintain good oral hygiene status with teeth and gums as it plays vital role inpreventing oral infection by pulling the infection (bacteria, toxins, and pus) out of the tissues, allowing the body to heal itself [15]. Furthermore, there is a dearth of evidence reporting the antiplaque efficacy of coconut oil pulling. Hence, the present study was conducted to compare and evaluate antiplaque efficacy of coconut oil pulling and a placebo.
Materials and Methods
A randomized control, double blinded parallel clinical trial was designed to evaluate the antiplaque efficacy of coconut oil pulling and a placebo among dental college students of Panineeya Institute of Dental Sciences, Hyderabad over a period of seven days. Ethical clearance was obtained from Panineeya Institute of Dental Sciences and Hospital Review Board (PMVIDS&RC/IEC/PHD/PR/0069-16). Participants were informed about the purpose of the study wherein, no incentives were provided to the students for participation and written informed consent was taken and the anonymity and confidentiality was maintained.
A pilot study was conducted to assess the feasibility, to estimate the sample size and to finalize the survey. With a mean plaque score of 0.9145, at power of 90%, α=0.05, effect size d=1.10526, the estimated overall sample size was 35. Hence, a sample of 40 students aged 18-22 years, willing to give consent and with a minimum twenty natural teeth with a minimum baseline plaque score ≥1 and with no history of dental visit in past three months were considered for the present study. Subjects were ineligible if they had existing soft tissue damage due to ill-fitting appliance and with orthodontic and prosthodontic appliances, who used systemic or topical antibiotics in past three month and presence of any dental condition which needed prompt professional attention (periodontal disease, pain, abscess, and swelling).
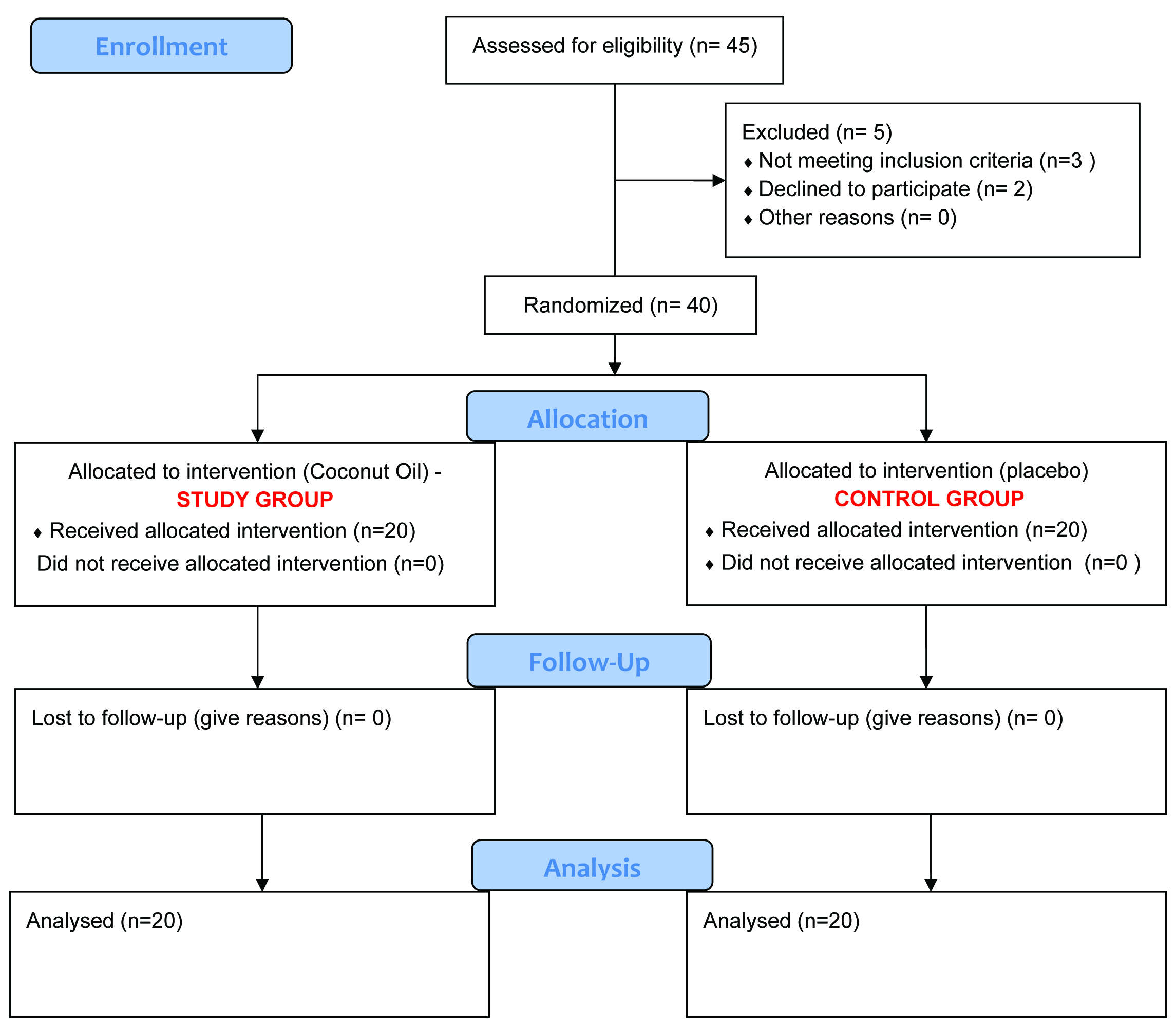
Coconut oil (Maxcare edible Coconut oil) and mineral water were used in the present study. The solutions were transferred to sterile amber colored containers and labelled A and B and given to investigator. Both the subjects and examiner were blinded in the study. All the examinations were conducted by a single pretrained and precalibrated investigator. The method of randomization (table of random numbers) and the distribution of liquids were done by second examiner. Each group comprised of 20 study subjects and random allocation of liquids was done to each group [Table/Fig-1].
Consort patients flow diagram.
Oil pulling procedure: Subjects were advised to take 10-15 ml (Maxcare edible coconut oil, mineral water) using a table spoon or till the mouth is half filled and sip, suck, pull the liquid through the teeth. Subjects were advised to lift their chin a bit; close eyes and start swishing liquid from left to right, front to back approximately for 10 minutes or till the subjects feel fullness in mouth. The participants were clearly instructed to take adequate precautions not to swallow the liquid while demonstrating the procedure. If at all swallowing occurs not to feel panic or fearful about the procedure. They were instructed to refrain from tooth brushing and not touse any other mouth wash during the study period.
Oral examination: The study was conducted for a period of seven days with clinical examination being carried out at baseline, day third and day seventh. Plaque levels were assessed by Turesky-Gilmore-Glickman Modification of the Quigley-Hein Plaque Index [16] (1970) for both the groups. At every visit, subjects were made to sit comfortably on a dental chair and plaque score were recorded under artificial light condition
Statistical Analysis
Statistical analysis was done using SPSS version 18.0 Independent sample t-test was used to calculate significant difference between two groups and percentage reduction in plaque scores from baseline to third and seventh day. Repeated measures ANOVA with post-hoc Bonferroni test was used to calculate significant difference between study and control groups at baseline, third and seventh day. A p-value of <0.05 was considered statistically significant.
Results
Out of 40 subjects, 20 subjects were randomly included in the study group and other 20 subjects in control group with a minimum of plaque score of ≥1. Majority of subjects were females (32), out of which 17 (85%) were in study group and 15 (75%) in control group. The mean age of study subjects was 20.5±1.72. The control group reported a slight high mean age (20.75±1.83), when compare to the mean age of study group (20.25±1.68).
The mean plaque scores at baseline among study group were 1.64±0.37 and for control group was 1.74±0.40. Though the mean plaque scores was higher among control group at baseline, third day and seventh day, significant difference was noticed only on seventh day (p=0.001) [Table/Fig-2].
Comparison of mean plaque scores between study group and control group at baseline, 3rd day and 7th day.
| Days | Study group mean±SD | Control group mean±SD | p-value |
|---|
| Baseline | 1.64 ±0.37 | 1.74±0.40 | 0.443; NS |
| Third day | 1.35±0.27 | 1.52±0.38 | 0.102; NS |
| Seventh day | 1.16±0.28 | 1.50±0.37 | <0.001; Sig |
Independent sample t-test.
Post-hoc Bonferroni test revealed that, among study group there was a decrease in the mean plaque scores from baseline to third day and to seventh day (B>3>7). Whereas in control group, the mean plaque scores decreased only on third day with no difference in plaque scores between third and seventh day there was no difference (B>3,7). The mean plaque scores showed a significant difference at baseline, third day and seventh day among both study (p<0.001) and control groups (p<0.001) [Table/Fig-3].
Comparison of mean plaque scores among study group and control group from baseline to 3rd day and 7th day.
| Groups | Days | Mean SD | p-value | Post-hoc test |
|---|
| Study Group | Baseline | 1.64 ±0.37 | <0.001; Sig | B>3>7 |
| Third day | 1.35±0.27 |
| Seventh day | 1.16±0.28 |
| Control Group | Baseline | 1.74±0.40 | <0.001; Sig | B>3,7 |
| Third day | 1.52±0.38 |
| Seventh day | 1.50±0.37 | | |
Repeated measures ANOVA with post-hoc Bonferroni test
Analysis of mean percentage reduction of plaque scores revealed a higher percentage of reduction among study group on third day (16.57±11.25) and seventh day (28.87±14.07) on comparison to control group (11.9±11.33, 13.79 ±13.38 respectively). However, statistical significant difference was obtained only on the seventh day [Table/Fig-4].
Comparison of mean percentage reduction of plaque scores of groups from baseline, Day 3 and Day 7.
| Variables | Groups(Mean percentage ± SD) |
|---|
| Study group | Control group | p-value |
|---|
| Percentage reduction at third day | 16.57 ± 11.25 | 11.90 ± 11.33 | 0.198 |
| Percentage reduction at seventh day | 28.87 ± 14.07 | 13.79 ± 13.38 | <0.001 |
p-value of <0.05 was considered statistically significant.
Percentage change is calculated = Baseline – follow-up/baseline*100
Independent sample t-test
Discussion
Oil-pulling therapy an alternate plaque control method claimed to have advantages over commercial mouth rinses with no side effects and being readily available in the household [10]. Furthermore, it was scientifically proven that oil pulling reduce the plaque scores [1] modify gingival scores [8] total oral bacteria count [10] in gingivitis patients and convert caries susceptibility from marked to slight or moderate susceptibility [10]. Asokan S et al., found oil pulling therapy was equally effective as chlorhexidine mouthwash in plaque control [8]. Similarly a significant reduction in plaque and gingival scores were noticed in a study by Amith HV et al., by using refined sunflowers oil [5].
As the oil is swished, mechanical shear forces exerts on the oil leads to its emulsification and increased surface area of the oil thereby reduce plaque adhesion and bacterial coaggregation [1]. The other possible mechanism might be the saponification process through alkali hydrolysis of oil by bicarbonates in saliva [10].
Oil pulling therapy can be done using edible oils like sunflower, seasame, coconut etc. The coconut oil is one of the edible oil with a high saponification value. Hughes FJ and McNab RR has reported that coconut oil inhibit bacterial growth by 26%, this may be due to saponification process [17]. Furthermore, the lauric acid of coconut oil reacts with sodium hydroxide of saliva and forms sodium laurate and is responsible for cleansing action and inhibition of plaque accumulation [1]. The effect of oil pulling using various edible oils on the biofilm model formed by S. mutans, Candida albicans, and Lactobacillus casei and it was found that coconut oil exhibited a significant antimicrobial activity against S. mutans and C. albicans on comparision with other oils [10]. In the view of a household agent which can comprehensively prevent plaque induced oral diseases, this study was initiated to evaluate and compare antiplaque efficacy of coconut oil pulling with a placebo among dental students of Hyderabad.
In the present study, Turesky, Gilmore and Glickman modification of Quigley Hein Plaque Index [16] (1970) was used to record plaque. The above index was considered for the study as it estimates the extent of plaque on the buccal or lingual surfaces covered on an ordinal scale and further uses a disclosing agent, which allows the patient visualization of plaque and helps them to develop efficient technique for plaque removal.
Dentistry has become an increasing popular career option for women and its expansion in dentistry has been one of the major dental work force trends in recent decades [18]. Hence, in the present study, a higher proportion of females formed the study population.
In this study, the mean baseline plaque levels were higher among control group (1.74±0.40) on comparison with the study group (1.64±0.37) but no statistical significant difference was noted. Similar findings were observed in a study by Asokan S et al., (0.96±0.431, 0.845± 0.376 respectively) among Chennai adolescents [9].
Tooth brushing study by Godha S et al., revealed no significant difference in mean plaque scores from baseline to seventh day and Bansal A et al., reported a significant reduction on using a 0.2% chlorhexidine mouthwash on seventh day [19,20]. Also, in the present study, coconut oil pulling showed a significant reduction in mean plaque score on seventh day. Furthermore, similar results also observed in a study by Peedikayil FC et al., among Kerala population [1]. Nonetheless, the control group also showed a significant reduction in mean plaque scores and this might be due to cleaning action by swishing of water for 10 minutes.
On comparison with the other oils Asokan S et al., found significant reduction in mean plaque scores using sesame oil at 10th day [9], whereas Amith HV et al., observed on 30th day on use of a sunflower oil [5]. However, in our study, we found a significant reduction on seventh day itself. This might be due to high saponification value and high lauric acid content in coconut oil leading to cleansing action and decreasing plaque accumulation.
Groupwise comparison revealed a decrease in the mean plaque scores among for both the groups on the third day, yet it was insignificant. However, on the day of third examination (seventh day), mean plaque scores were significantly lower among study group as compared to control group and this might be due to anti-inflammatory, antibacterial and emollient actions of coconut oil. These findings were in congruent with the study done by Peedikayil FC et al., in kerala where coconut oil pulling subjects showed significant reduction of plaque scores over seven days [1]. Furthermore, the above result is far more superior on comparison to other oral hygiene aid or, various oils, whereas, Brecx M et al., found a significant reduction only after three weeks on using a chlorhexidine mouthwash [21] and Amit HV et al., found it after 30 days on using sunflower oil on comparison with a control group (placebo) [5].
Many controlled clinical trials using chlorhexidine ranging for a period of six months or more has reported the plaque reduction from 16%-45%. On the other hand, Amith HV et al., observed 18%-30% of plaque reduction upon use of sesame oil for 45 days [5]. These results were similar with our study, except that the coconut oil pulling showed greater reduction (29%) within a short period of time (seven days). This might be due to the emulsification and saponification process of oil and further the viscosity of the oil can inhibit bacterial adhesion and plaque coaggregation [15].
Limitation
However, the present study acknowledges certain limitations such as short duration study period and single institutional study hence, generalization of results should be cautioned. Though study showed immediate positive effects, changes observed for short duration cannot be predicted in the long run. The most objectionable part of this procedure is that, it has to be performed early in the morning, on empty stomach and time required is long. A cross-over or parallel design with wash-out period would have been more validating as it removes the bias of variable response of the host.
Conclusion
In the present study, coconut oil pulling showed a significant reduction of plaque scores. Hence, could be used as a preventive home therapy to maintain oral hygiene, especially in developing countries. Further we recommend studies with large samples, varying time period and longtime follow ups to establish the efficacy of oil pulling therapy for effective plaque control and prevention of dental diseases.
Independent sample t-test.
Repeated measures ANOVA with post-hoc Bonferroni test
p-value of <0.05 was considered statistically significant.Percentage change is calculated = Baseline – follow-up/baseline*100Independent sample t-test
[1]. Peedikayil FC, Sreenivasan P, Narayanan A, Effect of coconut oil in plaque related gingivitis -preliminary reportNiger Med J 2015 56:143-47. [Google Scholar]
[2]. WHO / Oral healthlast accessed on 20/08/2016Available at http://www.who.int/topics/oral_health/en/ [Google Scholar]
[3]. Oral Health PageLast accessed on 20/08/2016Available at http://www.who.int/topics/oral_health/en/ [Google Scholar]
[4]. Quirynen M, Teughels W, Haake SK, Newman MG, Newman MG, Takei HH, Klokkevold PR, Microbiology of periodontal diseasesCarranza Clinical Periodontology 2006 10th edSaunders publishers:134-69. [Google Scholar]
[5]. Amith HV, Ankola AV, Nagesh L, Effect of oil pulling on plaque and gingivitisJ Oral Health Community Dent 2007 1(1):12-18. [Google Scholar]
[6]. Sirisha K, Devi PK, Oil pulling – a comprehensive cost-effective domiciliary remedyInt J of Res Dent 2014 4(1):01-05. [Google Scholar]
[7]. Kaur G, Singh A, Patil KP, Gopalakrishnan D, Nayyar AS, Deshmukh S, Chlorhexidine: first to be known, still a gold standard anti-plaque agentRes J Pharm Biol Chem Sci 2015 6(4):1407-24. [Google Scholar]
[8]. Asokan S, Emmadi P, Chamundeswari R, Effect of oil pulling on plaque induced gingivitis: A randomized, controlled, tripleblind studyIndian J Dent Res 2009 20:47-51. [Google Scholar]
[9]. Asokan S, Kumar RS, Emmadi P, Raghuraman R, Sivakumar N, Effect of oil pulling on halitosis and microorganisms causing halitosis: A randomized controlled pilot trialJ Indian Soc Pedod Prev Dent 2011 29:90-94. [Google Scholar]
[10]. Thaweboon S, Nakaparksin J, Thaweboon B, Effect of oil pulling on oral microorganisms in biofilm modelsAsia J Public Health 2011 2:62-66. [Google Scholar]
[11]. Bruce Fife MD, The healing miracle of coconut oil. Piccadilly Books Ltd 2000 1st editionHealth Colardo Springs: Wise publications Co:01-46. [Google Scholar]
[12]. Shino B, Peedikayil FC, Jaiprakash SR, Bijapur GA, Kottayi S, Jose D, Comparison of antimicrobial activity of chlorhexidine, coconut oil, probiotics, and ketoconazole on candida albicans isolated in children with early childhood caries: An In Vitro StudyScientifica 2016 :01-05. [Google Scholar]
[13]. DebMandal M, Mandal S, Coconut (Cocos nucifera L: Arecaceae): In health promotion and disease preventionAsian Pac J Trop Med 2011 4:241-47. [Google Scholar]
[14]. Srivastava P, Durgaprasad S, Burn wound healing property of Cocos nucifera: An appraisalIndian J Pharmacol 2008 40:144-46. [Google Scholar]
[15]. Tomar P, Hongal S, Jain M, Rana K, Saxena V, Oil pulling and oral health: A reviewIJSS Case Report & Reviews 2014 1(3):33-37. [Google Scholar]
[16]. Turesky S, Gilmore ND, Glickman I, Reduced plaque formation by the chloromethyl analogue of Vitamine CJ Periodontol 1970 41:41-43. [Google Scholar]
[17]. Hughes FJ, McNab RR, Oral malodour--a reviewArch Oral Biol 2008 53:1-7. [Google Scholar]
[18]. Parkash H, Mathur VP, Duggal R, Jhuraney B, Dental workforce issues: a global concernJ Dent Educ 2006 70(11):22-26. [Google Scholar]
[19]. Godha S, Dasar PI, Sandesh N, Mishra P, Kumar S, Balsaraf S, Impact of different oral hygiene aids for the reduction of morning bad breath among dental students: a crossover clinical trialClujul Medical 2016 89(4):525-33. [Google Scholar]
[20]. Bansal A, Marwah N, Nigam AG, Goenka P, Goel D, Effect of Achyranthusaspera, 0.2% aqueous chlorhexidine gluconate and punicagranatum oral rinse on the levels of salivary streptococuusmutans in 8-2 old childrenJ Contemp Dent Pract 2015 16(11):903-09. [Google Scholar]
[21]. Brecx M, Brownsfone E, MacDonald L, Gelskey S, Cheang M, Efficacy of listerine, meridol and chlorhexidine mouthrinses as supplements to regular tooth-cleaning measuresJ Clin Periodontol 1992 19:202-07. [Google Scholar]