Cervical and ovarian cancers are the most common gynecological cancers affecting women worldwide and in India. Cervical cancer is on a declining trend, but remains the second most common cancer in women after breast cancer. Every year in India, 122,844 women are diagnosed with cervical cancer and 67,477 die from this disease [1]. The high burden of cervical cancer in developing nations like India is attributed primarily to lack of awareness programs, no formal screening programs and thus most women present in the late stages of cervical cancer.
The exploration of new markers with prognostic or predictive value is of vital significance in the development of effectual anti-cancer therapies. The HER family is one of the most widely studied growth receptor families [2]. HER-2/neu is a membrane-bound receptor with tyrosine-kinase activity [3,4] and plays a crucial part in malignant transformation and carcinogenesis by interacting with the other members of the HER family to potentiate intracellular signaling [5,6].
Other than its role in progression of many malignancies, it has also been deeply assessed as a therapeutic target. Role of HER-2/neu expression in gynaecological malignancies is still being researched [7-9] to evolve a consensus.
Materials and Methods
This prospective study was carried out from January 2015 to December 2016 at Teerthanker Mahaveer Medical College and Research Center, Moradabad, Uttar Pradesh, India, after getting ethical clearance from the Institutional Ethical Committee.
A total of 70 diagnosed cases of premalignant and malignant lesions of uterine cervix were enrolled in the study. Cases of inflammatory lesions and metaplasia of uterine cervix were excluded. Among these 27 were premalignant (10 CIN-I, 9 CIN-II and 8 CIN-III) and 43 were malignant (one adenosquamous carcinoma, two adenocarcinoma and 40 squamous cell carcinoma).
All the patients included in this study were subjected to standard diagnostic criteria including detailed history, physical examination and subsequently histological diagnosis. Paraffin blocks of the above selected cases were taken for Haematoxylin and Eosin staining and reviewed.
After confirming and noting the diagnosis and microscopy details, sections were taken for immunohistochemical HER-2/neu and golden brown colour membrane and cytoplasmic staining was taken as a positive reaction. Intensity of HER-2/neu expression was graded according to 2014 ASCO/CAP guidelines for HER-2/neu reporting [Table/Fig-1] [10].
The 2014 ASCO/CAP HER-2 reporting guideline.
| Intensity of HER-2 expression | Characteristic features |
|---|
| 0 | No staining is observed or shows membrane staining that is incomplete and is faint/barely perceptible and within <10% of tumour cells. |
| 1+ | Membrane staining that is incomplete and is faint/barely perceptible and within >10% of tumour cells. |
| 2+ | Circumferential staining that is incomplete and/or weak/moderate within > 10% of tumour cells or complete intense circumferential membrane staining within < 10% of tumour cells. |
| 3+ | Complete intense circumferential membrane staining within > 10% of tumour cells. |
Statistical Analysis
Data was analysed using SPSS version 20.0. Chi-square test was used for comparison of data. A p-value < 0.05 was considered statistically significant.
Results
Among 35.7% of HER-2/neu positive cases, HER-2/neu expression scores were 0 in 64.3% (23 cases of CIN and 22 cases of SCC), +1 in 22.9%, (four cases of CIN and 12 cases of SCC) +2 in 10% (six cases of SCC and one case of adenosquamous carcinoma and +3 in 2.9% (two cases of adenocarcinoma) patients [Table/Fig-2].
Correlation of HER-2/neu overexpression with characteristics of premalignant and malignant lesions.
| S No. | Variable | Total | HER-2/neu Expression Scores | p-value |
|---|
| 0 | +1 | +2 | +3 |
|---|
| 1. | Overall | 70 | 45 (64.3%) | 16 (22.9%) | 7 (10.0%) | 2 (2.9%) | -- |
| 2. | Status |
| Premalignant | 27 | 23 (85.2%) | 4 (14.8%) | 0 | 0 | 0.020 |
| Malignant | 43 | 22 (51.2%) | 12 (27.9%) | 7 (16.3%) | 2 (4.7%) |
| 3. | Premalignant |
| CIN I | 10 | 0 | 0 | 0 | 0 | 0.248 |
| CIN II | 9 | 0 | 2 (22.2%) | 0 | 0 |
| CIN III | 8 | 0 | 2 (25.0%) | 0 | 0 |
| 4. | Malignant |
| Adenoca-rcinoma/ Adenos-quamous carcinoma | 3 | 0 | 0 | 1 (33.3%) | 2 (66.7%) | <0.001 |
| Squamous cell carcinoma | 40 | 22 (55.0%) | 12 (30.0%) | 6 (15.0%) | 0 |
| 5. | Histopathological Grade (n=43) |
| Well differentiated | 21 | 13 (61.9%) | 5 (23.8%) | 3 (14.3%) | 0 | 0.014 |
| Moderately differentiated | 15 | 8 (53.3%) | 5 (33.3%) | 0 | 2 (13.3%) |
| Poorly differentiated | 7 | 1 (14.3%) | 2 (28.6%) | 4 (57.1%) | 0 |
HER-2/neu overexpression rate was significantly higher in malignant (48.8%) as compared to premalignant (14.8%) cases (p=0.004) and HER-2/neu expression scores were higher (+2 and +3) in 20.9% of malignant cases as compared to none of premalignant cases, thus showing a significant difference (p=0.020).
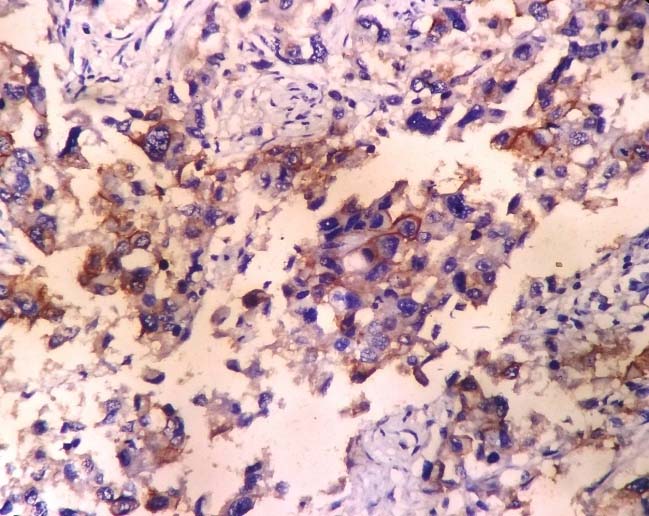
HER-2/neu positivity in CIN was 14.8% and it was only of +1 type, 45.0% in SCC which varied from +1 (12 cases) to +2 (six cases) [Table/Fig-3] and 100% positivity in adenocarcinoma and its variants which varied from +2 (one case) to +3 (two cases) [Table/Fig-4] but this difference was not significant statistically.
Showing +2 HER-2/neu expression score in a case of cervical squamous cell carcinoma (IHC; 400X magnification).
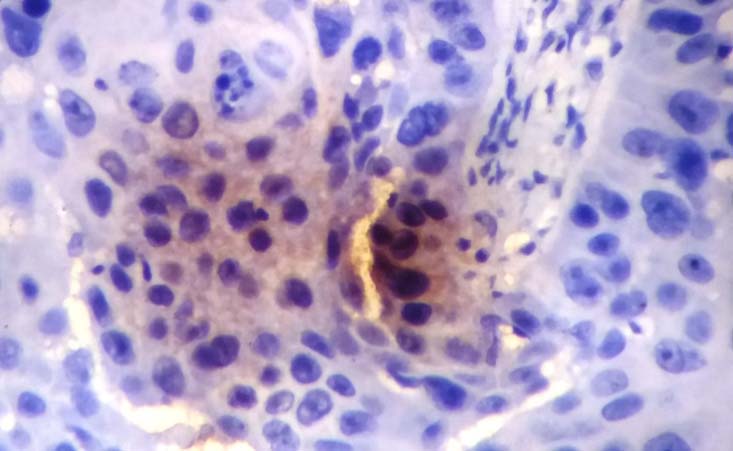
Showing +3 HER-2/neu expression score in a case of cervical adenocarcinoma (IHC; 400X magnification).
Higher HER-2/neu scores (+2 and +3) were seen in all the adenocarcinoma cases (100%) as compared to only 15% cases of SCC and this difference was significant statistically too (p<0.001) [Table/Fig-2].
Among premalignant cases, HER-2/neu expression scores did not show a significant association with CIN grades while among malignant cases, HER-2/neu expression was appreciably higher in (MD and PD) 59.09% as compared to (WD) 38.09% cases but association was not significant statistically (p=0.090) [Table/Fig-2].
Discussion
In the light of the literature and controversy that exists regarding the expression of HER-2/neu in various disorders of the cervix, this prospective study was designed to explore the expression of HER-2/neu oncoprotein in the cervical lesions and the correlation of these receptors with the histopathological grade and type of the tumour at the time of diagnosis. In the present study, we included only 23 premalignant and 47 malignant lesions and ruled out chronic cervicitis and metaplasia. In our study SCC cases (57.1%) outnumbered the adenocarcinoma cases (4.28%) which was in concordance to World Health Organization (WHO) too which states that squamous cell carcinomas account for ~70%–80% of cervical cancers while adenocarcinomas for 10%–15% [11].
Overall expression of HER-2/neu: In present study, HER-2/neu expression was seen in 35.7% and rest 64.3% did not show any positivity for HER-2/neu. A substantial difference in HER-2/neu overexpression in uterine cervical lesions has been shown in different contemporary studies. The positivity rate in present study is close to that reported by Sharma N et al., and Sarvade P et al., who reported positivity rate of 36.6% and 44% respectively [12,13]. The low positivity rate (0.006%) in the study of Conesa-Zamora P et al., could be attributed to strict criteria used by them wherein only a score of 3+ was considered as positive [14].
In present study, overexpression rate was significantly higher (p=0.020) in malignant cases (48.8%) as compared to premalignant cases (14.8%).
HER-2/neu expression and IHC scores: With respect to expression of scores, the number of cases with scores 2 and 3 were significantly higher in malignant lesions (21%) as compared to nil (0%) in premalignant lesions (p=0.020) [Table/Fig-2]. All the premalignant cases showed HER-2/neu overexpression score upto +1 only. Compared to findings of present study, in their study Joseph T and Raghuveer VC noted HER-2/neu overexpression in 70% of premalignant and 100% of malignant cases [15]. In their study, out of seven positive cases of CIN, four had score 1+ and remaining three had score 2+ whereas in 24 positive malignant cases, 22 (91.7%) had score 2+ and 3+, thus showing that higher scores are indicative of more severe form of cervical cancer. However, according to Sarvade P et al., no HER-2/neu overexpression was observed for any of the CIN cases (0%) whereas for malignant cases, the overexpression rate was 56.1% [13]. Thus, showing overexpression rate in malignant lesions to be closer to that observed in the present study (48.8%).
Premalignant and malignant lesions: Higher expression of HER-2/neu among malignant as compared to premalignant lesions in our study is in agreement with the findings of Sarvade P et al. and Carreras R et al., [13,16] and indicated the possibility of gradual progression in HER-2/neu expression from premalignant to malignant cases although several previous studies [17] do not endorse the same in terms of positivity alone. In his study, Gupta et al., also expressed similar concerns regarding the usefulness of HER-2/neu overexpression [18].
All the adenocarcinoma (100%) cases had IHC score 2 or 3 as compared to only 15% cases of squamous cell carcinoma had the same score, thus showing a significant difference [Table/Fig-2]. In contrast, Joseph T and Raghuveer VC who in their study reported 100% positivity rate for both adenocarcinoma as well as squamous cell carcinoma cases [15]. However, similar to our study, the lesser IHC score of 1+ was reported only in 10% SCC cases, thus indicating no differentiation capability of either IHC overxpression as well as the score in their study sample. Contrary to findings of both present study and that of Sharma N et al., and Joseph T and Raghuveer VC, in their study found none of the adenocarcinoma cases to be IHC positive [12,15] whereas for SCC cases, this rate was 61.1% and for adenosquamous carcinoma this rate was 50%. In another study, by Sarvade P et al., the positivity rate for adenocarcinoma, adenosquamous cell carcinoma and SCC was 60%, 0% and 56.7% respectively [13].
The findings of present study, thus do not show harmony with any of the previous studies except some resemblance with the study of Gupta N et al., who reported a positivity rate of 84.62% for adenocarcinoma as compared to only 54.17% for squamous cell carcinoma and a higher proportion of IHC scores 2+ and 3+ for adenocarcinoma (61.54%) as compared to SCC (43.8%) [18]. In fact, all the studies show different trends, thus indicating that these trends need to be followed further using larger sample sizes. Many studies on cervical lesions are of the opinion that HER-2/neu overexpression is directly linked to advanced grades and poorly differentiated tumour and having bad outcomes [19,20].
HER-2/neu expression and grade of tumour: In present study, HER-2/neu positivity rate showed an incremental trend from well differentiated (28.1%) to poorly differentiated (85.7%) malignant lesions. However, the association was not considerable statistically. However, with respect to higher scores 2 and 3, the proportion of cases with higher scores (2 and 3) was significantly higher in poorly differentiated grade (57.1%) as compared to well differentiated (14.3%) and moderately differentiated (13.3%) cases [Table/Fig-2].
Contrary to these findings, Joseph T and Raghuveer VC in their study reported 100% positivity rate for all the histopathological grades [15], however, with respect to IHC scores, they also reported an increasing trend of higher scores (3+) increasing from 0% (well differentiated) and 27.3% (moderately differentiated) to 72.7% (poorly differentiated) histopathological grades respectively. Gupta N et al., like our study also correlated HER-2/neu expression in various grades of 48 cases of SCC uterine cervix [18]. Expression was found to be 0% in well differentiated, 55% in moderately differentiated and 80% in poorly differentiated type of SCC. Sharma N et al., and Sarvade P et al., also reported similar trend of HER-2/neu expression [12,13]. Thus, the findings of present study are in agreement with the literature and show that with increasing loss of differentiation, the HER-2/neu IHC expression rate shows an incremental trend.
Limitation
One of the limitations of present study is a small sample size. In view of this small sample size, especially of premalignant lesions, most of the evidence are restricted to study of trends only and has not been established statistically. Even for meta-analysis and pooled analysis, the data on the issue is insufficient, hence further studies on larger sample size are recommended.
Considerable heterogeneity in the distribution of immunoreactive tumour cells could also be accountable for such conflicting reports on HER-2/neu expression in uterine lesions.
Conclusion
In conclusion, our study indicates that expression of HER-2/neu is relatively lower in cervical lesions. With shift from well to poorly differentiated lesions, the HER-2/neu expression rate shows an incremental trend. Immunohistochemical verdict of HER-2/neu expression do not distinguish subgroups of patients at higher risk of recurrence of disease. Additionally, this oncogene may not represent a future target for monoclonal antibody directed therapy for cervical cancer but still further studies on the issue are required before making a consensus.