TB has experienced resurgence in the world since the pandemic of Acquired Immunodeficiency Syndrome (AIDS). HIV infection alters the cell mediated immunity and increases the risk of progression of latent tuberculosis infection to active tuberculosis disease [1]. In HIV positive patients with CD4 counts <200/mm3, the features of pulmonary tuberculosis are often atypical [2]. Diabetics are more prone to TB due to decreased immunity [3]. Diabetes mellitus and active tuberculosis intensifies each other and combination of these two diseases forms a lethal combination [4].
Radiology remains one of the most important diagnostic modalities of tuberculosis infection. Radiological manifestations of pulmonary tuberculosis are dependent on several host factors, including underlying immune status. Impaired host immunity like HIV infection, diabetes mellitus etc., have been regarded as a predisposing factor in tuberculosis [5]. Endobronchial spread of disease, cavitatory lesions and lymphadenopathy can be easily detected by Computed Tomography (CT). Pleural effusion and bronchopleural fistula can also be detected in early stages [6]. The most common CT findings of reactivation pulmonary TB are centrilobular small nodules, branching linear and nodular opacities present as ‘tree-in-bud’ sign, patchy or lobular areas of consolidation, and cavitation. Cavitation usually indicates active disease [7].
This study was conducted to determine the CT findings of pulmonary tuberculosis and to compare the radiological presentation of pulmonary TB between immunocompetent and immunocompromised patients.
Materials and Methods
This cross-sectional study was conducted in the Department of Radiodiagnosis and Department of Tuberculosis and Respiratory Diseases, Government Medical College and Rajindra Hospital, Patiala, Punjab, India, from November 2011 to October 2013. The permission to conduct the study was taken from Institutional Ethical Committee. This study was conducted on 60 pulmonary tuberculosis patients after applying inclusion and exclusion criteria, which were sputum smear positive for Acid Fast Bacilli (AFB). These 60 patients were divided into two groups of 30 patients each as immunocompromised group and immunocompetent group. In immunocompromised group, out of 30 patients, 15 were diabetic and 15 were HIV positive. In the immunocompetent group 30 patients who were not having any other underlying disease with pulmonary tuberculosis were considered. CT chest findings of immunocompromised patients were compared with immunocompetent patients. All these patients after obtaining their consent were subjected to detailed clinical history and investigations as per performa.
Sputum smear examination for acid fast bacilli was done as per Revised National Tuberculosis Control Programme (RNTCP) guidelines [8]. Patients were considered to have diabetes if they were already a diagnosed case of DM at the time of hospital admission or were found to have two or more fasting blood glucose levels greater than 126 mg% or random blood glucose levels more than 200 mg% or values more than 200 mg% after two hours of 75 gram of oral glucose (GTT). The patients who were tested positive for HIV-1 and HIV-2 antigens with different ELISA kits as per NACO guidelines were taken as HIV infected. CD4 count was estimated at the same point and patient having CD4 count less than 200/mm3 were included in study group.
Pulmonary TB patients of less than 15 years of age, sputum smear negative patients and antitubercular treatment failure patients were excluded on the basis of history, clinical and physical examination.
Spiral CT scans of chest (Siemens 6 slice Somatom Emotion CT machine) were obtained with slice acquisition thickness of 8 mm and reconstruction interval of 8 mm from the level of 2 cm superior to lung apices up to the diaphragm. Non-ionic water soluble, 50-70 ml contrast media of strength 300 mg/ml was used in all the patients. CT scan images were viewed in lung window (level 700 HU; width 1,500 HU), mediastinal window (level 30-50 HU; width 350-500 HU) and bone window (level 2400 HU; width 200 HU).
Statistical Analysis
Quantitative and qualitative data were expressed as median [inter-quartile (IQ) range] and percentages, respectively. Qualitative variables were compared using Pearson Chi-square test. A ’p’-value of less than 0.05 was considered significant. Data was compiled and analysed using Epi info and SPSS 16.0 version software.
Results
In present study, out of 30 immunocompromised tuberculosis patients, 21(70%) patients were males and 9(30%) patients were females. Out of 30 immunocompetent patients, 16(53.3%) patients were males and 14(46.7%) patients were females.
Age distribution of the patients included in both the groups is tabulated in [Table/Fig-1].
Age distribution of study group.
| Age(in years) | Immunocompromised Group(n=30) | Immunocompetent Group(n=30) | Total |
|---|
| No.(%age) | No.(%age) | No.(%age) |
|---|
| 20-40 | 11(36.7%) | 9(30.0%) | 20(33.3%) |
| 41-60 | 15(50.0%) | 11(36.7%) | 26(43.3%) |
| >60 | 4(13.3%) | 10(33.3%) | 14(23.3%) |
The CT findings of the patients included in both the groups are tabulated in [Table/Fig-2]. Among 30 patients of immunocompromised group 23 (76.7%) were presented with radiologically atypical presentation. Lymphadenopathy was more prevalent in immunocompromised cases as compared to immunocompetent cases (63.3% versus 23.3%). There was no significant difference among both groups for milliary TB and pleural effusion.
CT findings of pulmonary tuberculosis patients.
| CT Patterns and Findings | Immunocompromised(n=30) | Immunocompetent(n=30) | p value |
|---|
| No. (%) | No. (%) |
|---|
| Atypical presentation | 23 (76.7) | 11 (36.7) | 0.002* |
| Nodular Opacities | 20 (66.7) | 27 (90.0) | 0.028* |
| Consolidation | 14 (46.7) | 22 (73.3) | 0.035* |
| Cavitation | 6 (20.0) | 18 (60.0) | 0.002* |
| Milliary Tuberculosis | 2 (6.7) | 1 (3.3) | 0.554# |
| Lmphadenopathy | 19 (63.3) | 7 (23.3) | 0.002* |
| Pleural Effusion | 8 (26.7) | 5 (16.7) | 0.347# |
Pearson Chi-square test applied.* - Significant, # - Non Significant
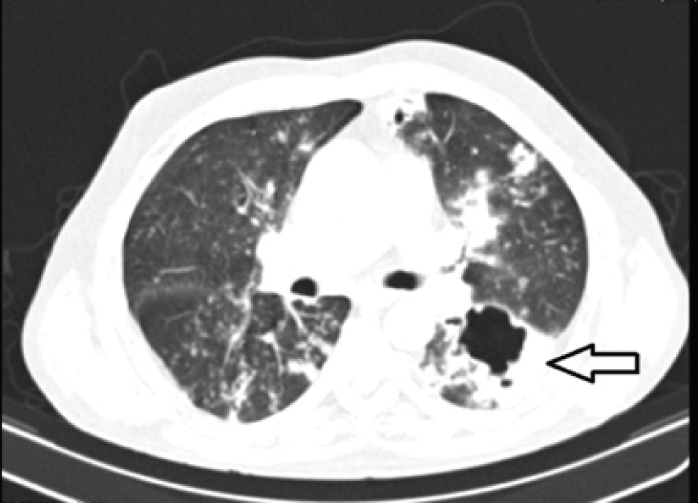
Though, number of cavities were more in immunocompetent patients than immunocompromised patients (18 versus 6) but they were multiple in immunocompromised patients (3/6) than in immunocompetent patients (1/18) which was statistically significant. Among six immunocompromised patients cavities were more in DM patients than HIV patients (5 versus 1) [Table/Fig-3a,b].
Number of cavities in DM versus immunocompetent group.
| Number of cavities | DM(n=15)No. (%) | Immunocompetent (n=30)No. (%) | Test used |
|---|
| Patients with Cavities | 5(33.3%) | 18(60%) | Pearson Chi- Square = 8.074p value = 0.004 |
| Single cavity | 2(40%) | 17(94.4%) |
| Multiple cavities | 3(60%) | 1(5.6%) |
Axial CECT chest lung window of a diabetic pulmonary tuberculosis patient. A bizarre shaped cavitatory lesion seen in the left lower lobe.
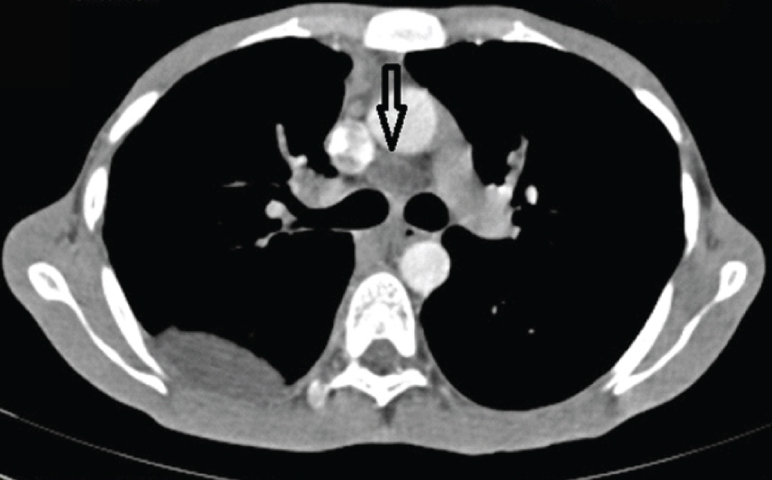
Lymphadenopathy was more prevalent in immunocompromised cases as compare to immunocompetent cases (19 versus 7). Among 19 immunocompromised patients lymphadenopathy was more prevalent in pulmonary tuberculosis-HIV patients as compared to DM patients (11 versus 8). As such lymphadenopathy was significantly higher in TB-HIV patients than immunocompetent patients (73.3% versus 23.3%) [Table/Fig-4a,b].
Lymphadenopathy in HIV versus immunocompetent group.
| Lymphadenopathy | HIV(n=15) | Immunocompetent(n=30) | Test used |
|---|
| No. (%) | No. (%) |
|---|
| Present | 11(73.3) | 7(23.3) | Pearson Chi-Square = 10.417p value= 0.001 |
| Absent | 4(26.7) | 23(76.7) |
Axial CECT chest mediastinal window of HIV seropositive pulmonary tuberculosis patient. Well defined lymph nodes with central hypodense area seen in the precarinal region with right pleural effusion.
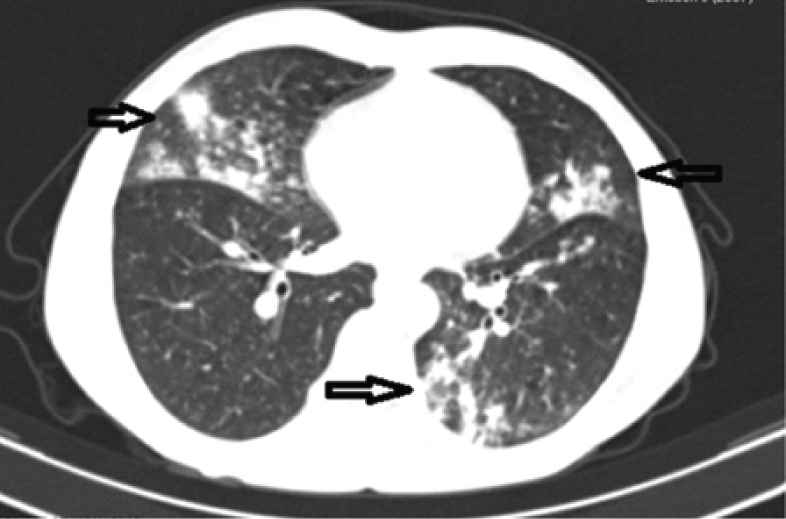
The involvement of different lung fields in both the immunocompromised and immunocompetent groups with pulmonary TB is given in [Table/Fig-5a,b]. Isolated lower lung field involvement was statistically significant in immunocompromised group as compared to immunocompetent group (23.3% versus 6.7%).
Involvement of lung fields in pulmonary tuberculosis.
| Disease Distribution | Immunocompromised Group (n=30) | Immunocompetent Group(n=30) |
|---|
| No. (%) | No. (%) |
|---|
| Isolated Upper Lung Field | 6(20.0) | 18(60.0) |
| Isolated Lower Lung Field | 7 (23.3) | 2(6.7) |
| Middle Lung Lobe | 6(20.0) | 2 (6.7) |
| Multilobar | 11(36.7) | 8 (26.7) |
Pearson Chi-Square 11.251, p-value 0.01
Axial CECT lung window of HIV positive pulmonary tuberculosis patient. Multiple air space nodules getting confluent at places forming patchy opacities in bilateral lung parenchyma (Right middle lobe, lingular lobe and left lower lobe).
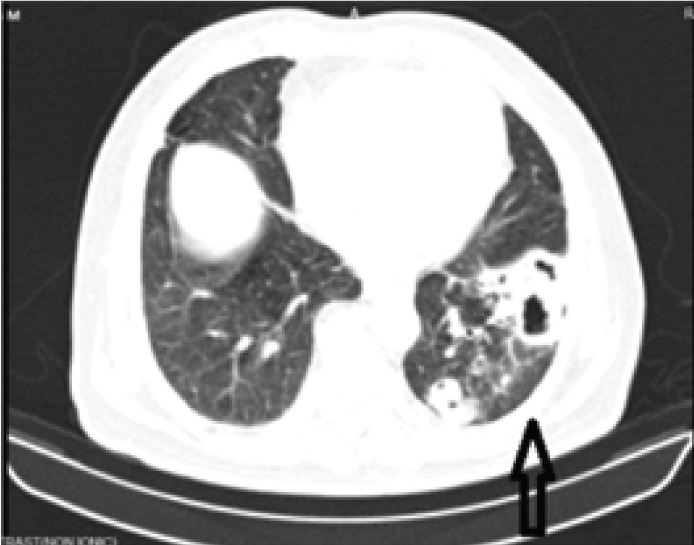
Isolated lower lung field involvement was statistically significant in diabetic group as compared to immunocompetent group (26.7% versus 6.7%). Isolated upper lung fields were involved more in immunocompetent group (60.0%) than in diabetic group (13.3%). [Table/Fig-6a,b].
Involvement of lung field-DM Vs immunocompetent group.
| Distribution of Disease | DM Group (n=15) | Immunocompetent Group(n=30) |
|---|
| No. (%) | No. (%) |
|---|
| Isolated Upper Lung Field | 2(13.3) | 18(60.0) |
| Isolated Lower Lung Field | 4(26.7) | 2(6.7) |
| Middle Lung Lobe | 1(6.7) | 2(6.7) |
| Multilobar | 8(53.3) | 8 (26.7) |
Pearson Chi-Square 9.900, p-value 0.019
Axial CECT lung window shows predominantly lower lung field involvement in a diabetic tuberculosis patient.
Discussion
The present study was carried out to understand the influence of underlying diseases like HIV and DM on radiological manifestations of sputum positive pulmonary tuberculosis patients.
Patients having HIV and DM have an increased risk of tuberculosis. Both these diseases adversely affect pulmonary tuberculosis and the radiological manifestations and management differ from situations where none of them exist in pulmonary tuberculosis patients [9].
The radiological pattern of pulmonary tuberculosis in HIV positive patients differs from those in HIV negative patients.
Pattern
Regarding the lung involvement, our study shows immunocompromised patients have atypical radiological findings of diseased lung in 23 (76.7%) cases, whereas, in immunocompetent cases atypical involvement of lung was in 11 (36.7%) patients only which were statistically significant. This is comparable to the study done by San KE et al., [10] who observed 67 (83.8%) patients with atypical pattern of disease in HIV positive patients. In HIV positive patients tuberculosis presents in atypical pattern, thus, confusing its presence with other opportunistic infections. Haramati LB et al., [11] observed atypical infiltrates (55% versus 10%) significantly more frequently in HIV positive patients than HIV negative patients. The study by Badie BM et al., [12] also observed that atypical radiological appearance of pulmonary tuberculosis in HIV positive subjects was common and mostly related to the low level of patient’s immune system. In case group, 80% patients presented with atypical involvement as compared to 31.7% in control group. Jabbar A et al., [13] observed lower lung fields were most frequently involved, followed by the upper and middle fields.
Nodular Opacities
Nodular opacities were present in 66.7% immunocompromised patients and 90% immunocompetent patients in our study, which was statistically significant. This was comparable to the study done by Leung AN et al., [14] who observed nodular opacities in 81% of tuberculosis-HIV positive patients and in 90% of HIV negative tuberculosis patients. de Almeida LA et al., [15] observed that 35.5% patients presented with ill-defined nodular opacities with centrilobular distribution. Naseem et al [16] observed centrilobular nodules (92%) was the most common CT finding in new tuberculosis cases.
Consolidation
In our study consolidation was present in 46.7% patients of immunocompromised group and in 73.3% patients of immunocompetent group and difference was statistically significant. Our study is comparable with Leung AN et al., [14], who observed that parenchymal consolidation was observed in 43% HIV positive and 69% HIV negative patients.
Cavitation
Our study found cavitation in immunocompromised group was 20% whereas, in immunocompetent group it was found in 60% patients. Our study is in concordance with the study done by Haramati LB et al., [11] where they showed that HIV negative patients had cavitation significantly more frequent than HIV positive patients (52% versus 18%). Leung AN et al., [14] also observed cavitation in 19% HIV-seropositive patients and in 55% HIV-seronegative patients.
Cavitation in Diabetes Mellitus
In our study we found that among immunocompromised group cavitations were found in 33.3% diabetic patients and out of these multiple cavities were found in 60% patients. In immunocompetent group single cavities were found in 94.4% patients. Ikezoe J et al., [17] found that in diabetic or immunocompromised patients with active tuberculosis, multiplicity of cavities was present in 44% patients. In study done by Inayat N et al., [18] main radiological presentation was cavitation which was seen in 20% in TB group as compared to 25% in TB-DM group. Tatar D et al., [19] detected higher rates of smear positivity and a greater incidence of cavity disease in DM cases. Thus, a higher smear-positivity rate is likely to be associated with greater cavity formation and extensive pulmonary damage due to DM. Our study correlates with the above mentioned findings because in our study group also, only sputum positive patients were included.
Lymphadenopathy
In present study, lymphadenopathy was in 19 immunocompromised patients and seven immunocompetent patients and the difference was statistically significant. Out of these 19 patients of immunocompromised group, lymphadenopathy was present in 73.3% of HIV positive patients and rest was in diabetic patients. Our study is in concordance with the study conducted by Haramati LB et al., [11] where they found that HIV positive patients had mediastinal lymphadenopathy (60% versus 23%) significantly more frequent than HIV negative patients. de Almeida LA et al., [15] also found 68.8% patients with mediastinal or hilar lymph node enlargement were AIDS patients with pulmonary TB.
Distribution of Disease
Pulmonary tuberculosis patients characteristically show radiographic evidence of apical abnormalities of lung. It is mainly attributed to oxygen rich environment in the lung apices but in fact may result from diminished apical lymphatic drainage. In our study, isolated upper lung fields were involved in 60% patients of immunocompetent group and in 20% patients of immunocompromised group. An isolated lower lung field was involved in 23.3% patients in immunocompromised group and in 6.7% patients in Immunocompetent group. Multilobar involvement in immunocompromised group was in 36.7% patients and in immunocompetent group was in 26.7% patients. Study conducted by Singla R et al., [20] concluded that there is higher involvement of lower lung fields in diabetic patients than immunocompetent patients (23.5% versus 2.4%). Study done by Perez-Guzmen C et al., [21] concluded that lower lung field lesions are significantly higher in tuberculosis patients with DM than tuberculosis patients without DM. (19% versus 7%). Ahmad Z et al., [22] in their study concluded that in HIV-TB cases lower lung fields were more involved than non-HIV TB patients (46.15% versus 9.75%).
Limitation
Few immunocompromised patients had deranged renal function tests, so contrast enhanced CT could not be performed in such cases.
Conclusion
HIV seropositive tuberculosis patients have an impaired host cell mediated response to Mycobacterium tuberculosis, so they have a lower prevalence of consolidation, cavitation and nodules however, they have a higher prevalence of hilar or mediastinal lymphadenopathy. Diabetic patients with tuberculosis have a higher prevalence of nonsegmental distribution and of multiplicity of cavities. Our study highlights the impact of HIV and diabetes on radiological manifestation of pulmonary tuberculosis which is very atypical on presentation. Thus, active case finding by interpreting atypical radiological manifestations amongst people with underlying immunosuppressive diseases has essential role in control of pulmonary tuberculosis.
Pearson Chi-square test applied.* - Significant, # - Non Significant
Pearson Chi-Square 11.251, p-value 0.01
Pearson Chi-Square 9.900, p-value 0.019