DH is characterized as acute, non-spontaneous, short or long lasting pain originating from exposure of dentin to thermal, chemical, mechanical or osmotic stimuli that cannot be attributed to any other dental pathology [1].
Different terminologies have been used to describe hypersensitivity based on the place of its occurrence such as: cervical, root, dentin and cemental hypersensitivity. All of these terms convey similar clinical conception and are interchangeable [2,3]. Even after extensive research in this field, no treatment has been universally accepted.
Based on the mechanism of action, desensitizing agents are classified as nerve desensitizers, protein precipitants, tubule occluding agents and tubule sealants [8]. Recently, lasers have been introduced in this classification owing to their various modes of action to reduce DH [9].
Although literature reveals abundance of in-office desensitizing agents, still no single agent can be considered as ideal for long term relief from this condition. Lasers cause closure of exposed dentinal surface due to melting of dentine without cracking and results in reducing the permeability and hydraulic conductance [10].
It employs low amperage direct electrical current to introduce ions or ionized drugs into tissues. This mechanism works on principle that like charges repels and opposite charges attract. Ionized drugs can be driven into tissue after application of appropriately charged electrical current. This explains local application of drugs in concentrated form by iontophoresis.
Microstructural changes in dentinal tubules are not evident in in-vivo studies. In vitro studies are carried out to assess dentinal tubule occlusion using SEM, where we can observe specimens under higher magnification [13].
The aim of the present in vitro study was to evaluate and compare the effectiveness of iontophoresis with 0.33% NaF gel and diode laser alone on occlusion of dentinal tubules under SEM.
Null hypothesis was proposed that there will be no statistically quantitative difference in occlusion of dentinal tubules on treatment with iontophoresis with 0.33% NaF gel and diode laser irradiation.
Materials and Methods
The present in vitro SEM study was undertaken at Department of Periodontology, School of Dental Sciences, Karad, Maharashtra, India. The study was conducted during the period from January 2015 to June 2015 after due approval from Ethical Committee of KIMSDU (Ref number KIMSDU/IEC/04/2014, dated 23/09/2014).
Teeth with intact root surfaces and unaltered by extraction procedure were included for specimen preparation. Teeth treated previously with desensitizing therapy, cracked teeth with defective restorations were excluded. Teeth which had undergone root canal therapy or with any apical lesion, caries, roughness of root surfaces, developmental anomalies such as concrescence, fusion were also excluded.
Preparation of the specimen: A pilot study was conducted (n=2 for each group) to evaluate the feasibility of acquiring SEM data in longitudinal and transverse sections of dentinal tubules. The sample size of 20 dentine specimens for each group was based on power analysis and observations of the pilot study. Twenty selected freshly extracted teeth were cleaned of gross debris and stored in 10% formalin solution. Teeth were ground with carbide bur to remove outer enamel layer and polished with sand paper. Teeth were then sectioned with a carborandum disc attached to a straight handpiece (KAVO EWL type 4415, KAVO®, West Germany) to obtain three dentin specimens each. A total of 60 dentin samples of 2 mm thickness were obtained in both longitudinal and transverse section. The dentin specimens were placed in an ultrasonic cleaner (SONICER®, Yoshida Dental Mfg Co Ltd, Osaka, Japan) with distilled water for 30 seconds. Later, the specimens were etched with 6% citric acid for a period of two minutes to remove the smear layer and then rinsed in distilled water. The prepared samples were randomly assigned to three groups: Each group included 10 longitudinal sections and 10 transverse sections.
Control group: Twenty specimens were acid etched with 6 % citric acid for two minutes and no intervention was carried out and they served as control group.
Iontophoresis treatment group: Twenty specimens were inserted into a foam tray containing 0.33 % NaF Gel (Medical S.R.L Via Olivera, 42, 31020 San Vendemiano) and subjected to iontophoresis (Jonofluor Scientific®, Medical) at 1.5 mA output current for three minutes.
Laser treatment group: Twenty specimens were lased with 980 nm Diode Laser (Photon Plus® Zolar Technology and Manufacturing Co. Inc. Mississauga, ON Canada) at 0.5 W/PW (62.2 J/cm2) in noncontact mode for 30 seconds.
Scanning electron microscope analysis: The analysis of specimens under SEM (JEOL® JSM - 6360, Japan) micrographs was carried out by an expert to evaluate occlusion of dentinal tubules. SEM test specimens were evaluated at 10KV and x2000, x5000 magnification for surface characteristics and patency or occlusion of dentinal tubules. Control samples were examined by low energy SEM (below 1 keV), to ensure that the dentin tubules were in an open un-occluded state. Test samples were examined by low voltage SEM to determine the effect of the iontophoresis and diode laser on dentin tubule occlusion. The total number of tubules visible, number of open, completely occluded and partially occluded tubules was counted in each microphotograph.
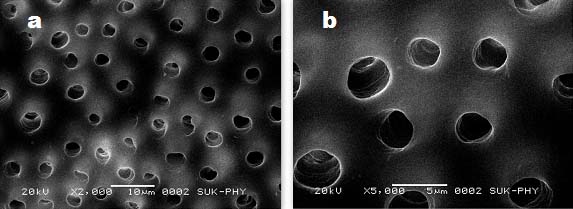
All the specimens were scanned for determining occlusion of tubules using following criteria. The tubules were considered completely occluded when they show either complete penetration of the crystal or complete obliteration of the canals by the reaction products. The tubules were considered partially occluded when there is a central opening in the canal with circumferential closure of the tubule or more than 50% reduction in the diameter of the tubule [Table/Fig-1,2, and 3].
Morphology of dentinal tubules of control group showing patency of dentinal tubules after acid etching at x2000 (a); and x5000 (b).
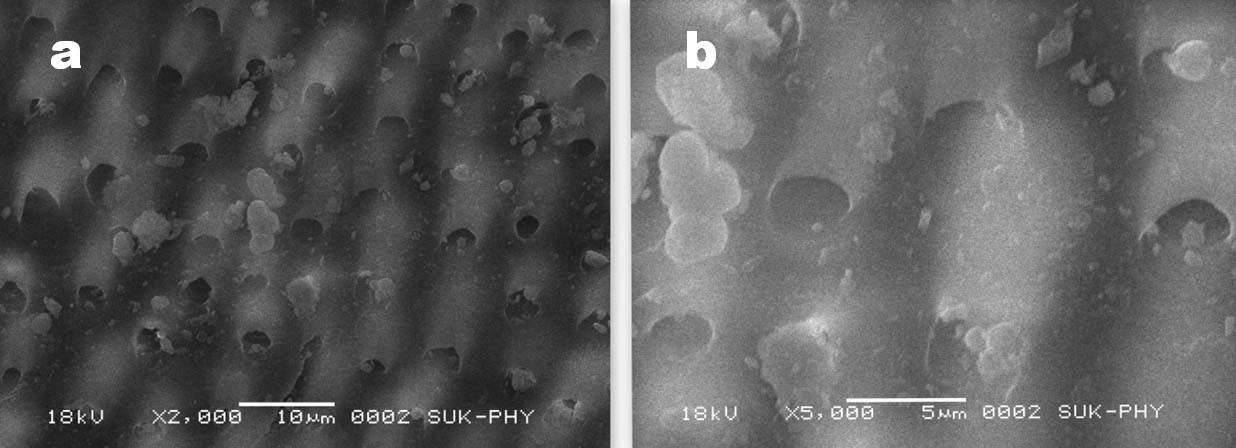
Morphology of dentinal tubules treated with iontophoresis along with 0.33% NaF gel showing completely and partially blocked tubules with crystal plug formation at x2000 (a); and x5000 (b).
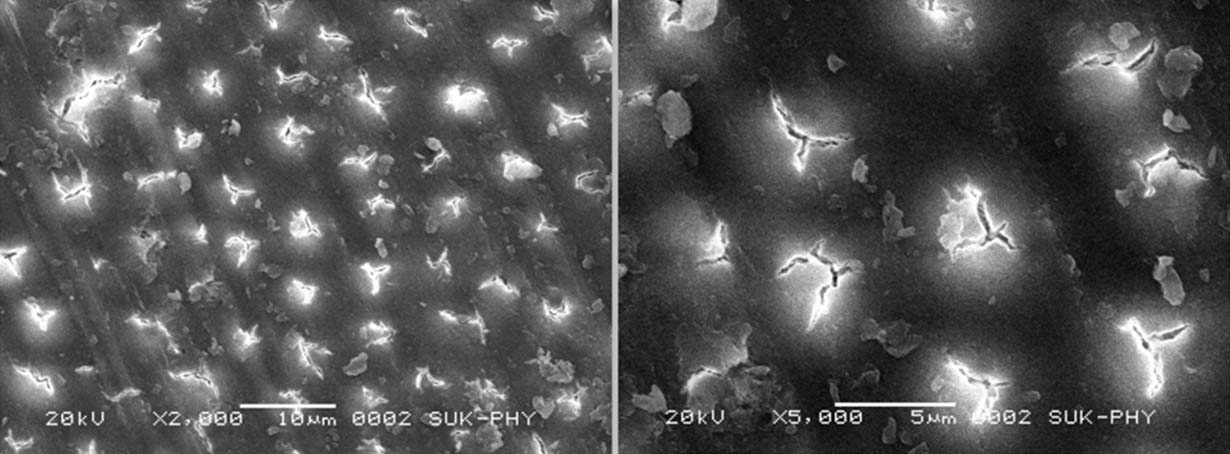
Morphology of dentinal tubules treated with diode laser (980 nm) showing partial and completely blocked tubules by melting of dentin at x2000 (a); and x5000 (b).
The percentage of tubules blocked was calculated as:
Number of tubules blocked x100/total number of tubules [14].
Statistical Analysis
The mean values were calculated for completely closed, partially closed and open tubules in iontophoresis and laser groups. The percentage of completely closed tubules, partially closed tubules and open tubules were analysed. Mann Witney U Test was employed for comparison of partially closed and closed tubules between laser and iontophoresis groups. For comparison of open tubules between control, iontophoresis and laser groups, Kruskal Wallis test was employed.
Value of p < 0.05 was considered as level of statistical significance. Data was analysed using IBM SPSS version 20.0 software.
Results
The percentage of open, partially closed and completely closed dentinal tubules among the study groups is shown in [Table/Fig-4].
Percentage of tubules open (patent), closed and partially closed in each study group.
| Tubules | Control | Iontophoresis | Laser |
|---|
| No. (%) | No. (%) | No. (%) |
|---|
| Closed | 0 (0) | 6 (1.99) | 101 (24.16) |
| Partially Closed | 0 (0) | 141 (46.69) | 187 (44.74) |
| Open | 417 (100) | 155 (51.32) | 130 (31.10) |
| Total | 417 (36.68) | 302 (26.56) | 418 (36.76) |
Intergroup comparison of closed tubules between the groups suggest that laser group was highly effective in completely occluding the tubules than iontophoresis group with p<0.001. On further comparison of partially occluded tubules among the study groups, the results were not statistically significant with p-value being 0.16. This suggests that both laser and iontophoresis showed similar ability of partially occluding the dentinal tubules [Table/Fig-5].
Comparison of closed and partially closed tubules between iontophoresis and laser groups using Mann-Whitney U Test.
| Closed Tubules | Mean | SD | Mann Whitney U statistic | p-value |
|---|
| Iontophoresis | 0.3 | 0.92 | 16 | <0.001* |
| Laser group | 5.05 | 3.71 |
| Partially Closed Tubules |
| Iontophoresis | 7.05 | 4.32 | 173 | 0.16 |
| Laser group | 9.35 | 6.06 |
*significant
The distribution of open tubules among the three groups revealed a high statistical significance with p<0.001 suggesting the order of efficacy in occluding the dentinal tubules as, laser >iontophoresis> control [Table/Fig-6].
Kruskal Wallis test for distribution of open tubules in control, iontophoresis and laser groups.
| Open Tubules | Sum of ranks | Mean of ranks | Mean | KW | p-value |
|---|
| Control | 903.5 | 45.18 | 20.85 | 19.556 | <0.001* |
| Iontophoresis | 437.5 | 21.88 | 7.75 |
| Laser group | 489 | 24.45 | 6.5 |
*significant
Comparison between longitudinal and transverse sections: The longitudinal and transverse sections were compared among the study groups to determine any differences in the number of partial and complete occlusion of the tubules using two sample t-test (unpaired test). It was found that there was no significant difference between the longitudinal sections and transverse sections (p > 0.05) suggesting there was no difference in laser and iontophoresis group in occluding the tubules in longitudinal sections and transverse sections.
Discussion
DH is a common clinical condition that is frequently encountered yet poorly understood [15]. Numerous theories have been proposed over more than a century towards explaining the mechanisms involved in DH.
Routinely used desensitizing methods may range from simplest to the most complex (e.g., simple-desensitizing tooth pastes, intermediate-iontophoresis and to complex ones such as lasers and tissue graft) [16]. Keeping in mind the limitations and shortcomings of the available literature and need of the hour, the present study was designed to test the efficacy of iontophoresis with 0.33 % NaF and diode laser application in management of dentinal hypersensitivity.
NaF gel was used in the present study as it is readily absorbed by dental hard tissues and fluoride ions thus adsorbed under walls of the dentinal tubules as well as on the surface of calcium, forms an insoluble compound calcium fluoride (CaF2) with the tooth substance [17]. This forms a new physical barrier and narrows the diameter of dentinal tubules, reducing its permeability. It was discovered that fluoride penetrates the pulp and interferes with its function, lowering its vitality. Thus, it is no longer receptive to pain and a reaction between fluoride and the free ions of some electrolytes, such as calcium, makes these ions unavailable for the normal mechanism of pain conduction [18]. A single application of NaF is less effective as it forms small sized calcium fluoride crystals (approximately 0.05 μm) which are easily soluble in saliva [19].
In this study, concentration of 0.33 % NaF was used in combination with iontophoresis, as it was seen that at this concentration, secondary dentine formation occurs. The efficacy of sole diode laser in the management of DH has been well documented in the literature, suggesting its effectiveness for one week, two months, three months and six months [20-25].
In our present study, the laser group exhibited complete occlusion in 24.16% of the tubules and partial occlusion in 44.74%. Our results are in agreement with the results of Umana M et al., and Nandkumar A and Iyer VH who suggested that diode lasers were able to seal the dentin tubules [26,27]. Umana M et al., showed that diode laser irradiations at 0.8 and 1 W led to occlusion or narrowing of dentin tubules without provoking fissures or cracks while graphite paste increased the thermal effects in dentin [26]. Nandkumar A and Iyer VH conducted a study to evaluate the efficacy of Er;Cr:YSGG and diode laser (810 nm) against clinically proven dentrifices [27]. They concluded that laser treatment of exposed dentinal tubules with Er;Cr:YSGG or diode laser promises a non invasive, pain free and relatively safe treatment option.
However, the results of present study are in contrast with Kreisler M et al., and Gholami GA et al., who did not obtain any microstructural changes after using diode laser at 1W, 10 Hz, 810 nm for 30 and 60 seconds respectively [28,29]. On further comparison between the longitudinal sections with the transverse sections, there was no statistically significant difference in tubule occlusion after laser irradiation.
Diode laser is a soft tissue laser with wavelength ranging from 655 nm to 980 nm. Diode laser at different wave length of 780,790, 830 and 900 nm have been studied by various authors for desensitization [29]. Diode laser leads to increase in mitochondrial ATP through bio-stimulation, increases pain threshold of free nerve ending, provide analgesic effect by increase in endorphins. It also inhibits cyclooxygenase enzyme which causes conversion of arachidonic acid into prostaglandin which in turn increases the pain transmission by glutamate or substance P. There is also formation of secondary dentin by odontoblast due to bio-stimulation [30].
Modification of dental hard tissue by laser irradiation is becoming increasingly popular in dentistry. The results of our current study show that thermal effects caused by diode laser resulted in sealing of dentinal tubules. Absorption of the laser energy by carbonate and phosphate minerals in dentine would have led to the melting of the tubular structure thereby altering the morphology of the tubules [31-33].
The features of an ideal desensitizing technique/material as described by Lutin ND et al., are; it should be easy to apply, non irritating to the pulp tissue, painless, consistent and effective in long term, quick acting and produce no discoloration [34].
In our present study, the iontophoresis group showed complete occlusion in 1.99% of the tubules and partial occlusion in 46.6% and there was a statistically significant difference with p<0.05 between iontophoresis and laser group. These results are concurrent with Mangalekar SB et al., [35] who reported that NaF iontophoresis provided better desensitising effect than dipotassium oxalate and potassium nitrate.
Lefkowitz W et al., proposed formation of reparative dentin in response to current application to dentin resulting in formation of dead tracts in primary dentin [36]. Here, the effective agent was direct current. Proposed mechanism involves electric current induced paraesthesia by altering sensory mechanism of pain conduction. Another alternative states that iontophoresis acts by influencing ionic motion by electric currents, thus enhancing ion uptake by the dentinal tubules and achieving desensitization [37].
However, the findings of our study relies on the mechanism of its action that it causes increased penetration of fluoride into the tubules forming insoluble crystals which plug the dentinal tubules.
The comparative SEM findings of the present study revealed statistically significant difference in terms of percentage of completely occluded tubules wherein the laser group showed better results. The present study revealed no significant difference in terms of percentage of partially occluded tubules among the groups. These findings are in agreement with separate non comparative studies of Umana M et al., and Mangalekar SB et al., [26,35]. The results obtained in our study are in agreement with study conducted by Liu Y et al., who demonstrated that 2 Watt/Continuous wave (166 J/cm2) was suitable parameter for a 980 nm diode laser to seal dentinal tubules without excess melting of the dentin [38].
Limitation
The limitation of the present study is the small sample size and lack of clinical assessment of DH. Furthermore, variations in morphology and source of dentin specimens make interpretation of in vitro results complicated and therefore extrapolating such results to the clinical scenario should be done carefully. Further in vivo studies using diode laser with different power outputs and with different concentrations of NaF gel can be tested so as to obtain ideal parameters for management of DH.
Conclusion
Within the limitations of this study, diode laser was found to produce more complete occlusion of dentinal tubules while iontophoresis with 0.33% NaF gel produced more of partial occlusion. Hence, diode laser could provide more effective and long term relief from DH than iontophoresis with NaF gel.
*significant
*significant