Adolescence is the subsection, which encompasses 1.2 billion individuals of the entire population. The United Nations defines adolescents as individuals aged 10–19 years: in effect, those in the second decade of their lives [1]. Adolescents constitute a group, under constant exposure to additional significant factors, such as emotional, social and physical situations which creates a more challenging condition [2]. It is an important period of life when a person spends a great deal of time participating in numerous sport activities and are more attracted towards sugary diet so, they are more prone to dental disorders [3].
Adolescents are mostly injured during sports activities, traffic accidents and some forms of violence (e.g. fights, assault and battery) which may lead to traumatic injuries [4]. Traumatic injuries not only pose a health risk worldwide, but are also regarded among serious social problems. One important category of traumatic injuries is dental trauma, accounting for a major part of health problem in adolescents [5]. Dental injuries generally affect only a single tooth; though, certain trauma types such as vehicle accidents and sports injuries might involve multiple tooth injuries [6]. Coronal fracture of the anterior teeth area is common form of dental trauma that mainly affects adolescents [7]. This not only causes pain and discomfort but can affect the most endearing quality of a human being which is their smile. A ‘smile’ that shows beautiful natural teeth is a greatest asset one person can have. Adolescents are especially perceptive about missing/fractured front teeth and there is often a conscious effort to avoid smiling. The permanent anterior teeth are not only important for aesthetics but are also essential for speech, mastication, health of adjoining tissues and psychological health of adolescent [8].
Poor smile and oral health has been related to poor social relationships and permanent disabilities that affect the ability to learn and grow which may lead to reduced self-esteem [9]. Healthy and free of pain free mouth enables an individual to eat, speak and have higher self-esteem [10].
Self-esteem is a domain of social psychology and was thought to be a relevant personality trait to be included in the study. It is the sum total of one’s self-confidence, self-worth and self-respect. The fundamental nature of self-esteem is based on understanding, accepting and liking oneself [11]. It has been reported that self-esteem is an important factor to consider when predicting the outcome of health treatments. It is postulated that low self-esteem can be associated with worse oral health related quality of life, thereby indicating that the personality traits could explain some of the impacts of oral disorders [12]. The adolescents with dental disorders may have more impact on self-esteem as compared to and those without dental disorders. This study aimed to assess the prevalence of TDI and to compare its effect on self-esteem of adolescents with and without TDI.
Materials and Methods
This population based comparative study was conducted in three phases [Table/Fig-1] among 10 to 17 years old adolescents from November 2014 to January 2016, for which the ethical clearance was obtained from Institutional Ethical Review Board of Surendera Dental College and Research Institute, Sri Ganganagar, India. The required cluster of adolescent population was targeted from the students enrolled in various schools. Written consent was taken from the administrators of the selected schools and the guardians of the students for the research.
Flowchart of the study
TDI, Traumatic Dental Injury; PPE, Probability Proportional to Enrolment Size; RSES, Rosenberg’s self esteem scale, SES- socio-economic status
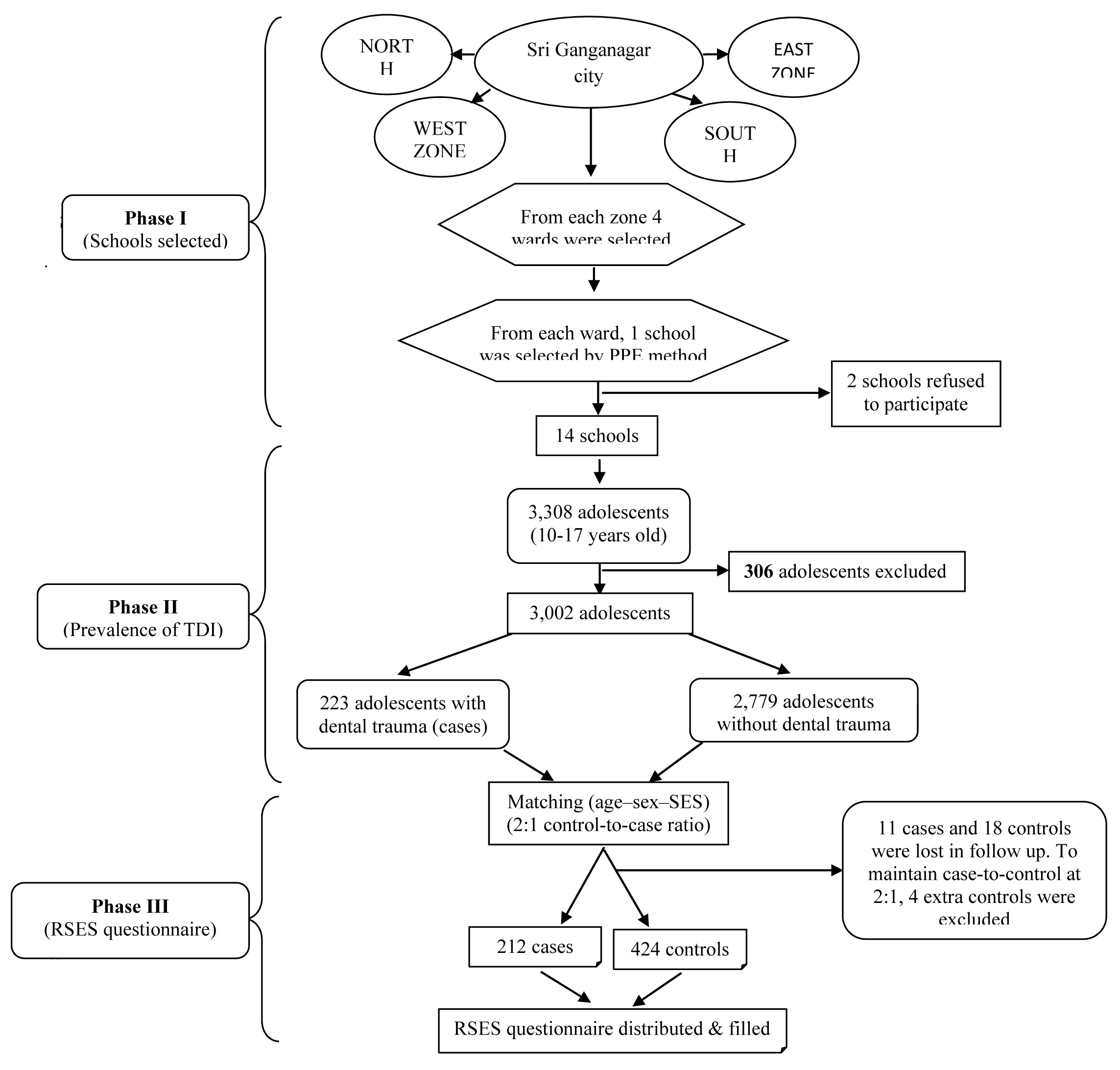
First phase: In order to obtain a representative sample, multi-stage sampling technique was used, for which the city was divided into four different zones in first stage. Later, four wards were selected randomly from each zone. Out of each selected ward an English medium school was selected based on Probability Proportional to Enrolment (PPE) size making the initial number of selected schools to 16. According to PPE, the schools with high number of regularly attending students were more likely to be selected than schools with low attendance of students. Out of 16 total schools, two schools refused to participate, giving an initial school participation rate of 87.5%. The power design considered for the present study was 80%.
Second phase: Oral health assessment was carried out among a total of 3,308 adolescents aged 10 to 17 years old from the selected schools. All adolescents who presented with erupted permanent anterior teeth (laterals and centrals) and who consented to further participation, were eligible for inclusion provided they had no missing or filled anterior teeth, excessively large diastema, open bites, malformed teeth (peg laterals), severely rotated teeth, extensive crowding, orthodontic appliances, abundant amounts of plaque or severe gingival inflammation, as these factors might also affect perception of appearance. After applying inclusion and exclusion criteria, a total of 3,002 adolescents were included in the study, among which a total of 223 adolescents were diagnosed with dental trauma in the anterior teeth (cases). After selecting the cases, a list of all the potential controls was prepared by one of the examiners comprising 2,779 adolescents 10-17 years old, without any TDI.
The children were examined by four examiners (NG, DKM, AS, PK). WHO type III examination was carried out under natural light using mouth mirrors and sharp probes [13]. The maxillary and mandibular anterior teeth from canine to canine were examined for traumatic injury which was scored using a modified version of Ellis classification [14]. Ellis Class I, Ellis Class II and Ellis Class III were included in the study and rest were excluded as the researchers did not have access to X-rays.
Prior to the examination, process of calibrating the four examiners for the clinical conditions was conducted by a ‘Gold Standard’ examiner before the main study was carried out to ensure the diagnostic reliability. The pilot study consisted of evaluating 30 adolescents, for diagnosing and recording dental trauma. A kappa value of 0.95 for inter examiner agreement was obtained using Statistical package for the social sciences (SPSS).
Third phase: A 2:1 control-to-case ratio was adopted and matching the adolescents was fulfilled by limiting the referent group (controls) to have essentially the same structure as that of index group (cases) according to the various variables age, sex and Socio-Economic Status (SES) which were categorized determining the age–sex–SES combination for each case. Subsequently, controls with the same age–sex–SES combination were chosen for each case. When more than two controls matched one case, adolescents were selected by the most similar characteristics in this order: same class, same school and closest home address. If more than two controls still matched one case, a simple random selection was performed. SES was determined by household income. The sample size was assessed to be 669 adolescents (223 cases and 446 controls). The cases and controls were followed up after evaluating the sample for the assessment of self-esteem. Few adolescents (11 cases and 18 controls) were absent on the day of follow up. To maintain case-to-control ratio at 2:1, four extra participants present in the control group were also excluded. So the final sample size was 212 cases and 424 controls among which RSES questionnaire was distributed [15].
Two examiners (AM, MB) distributed RSES questionnaire among the students with a prior detailed description of the inventory in regional language for better understanding and interviewed them. All the 636 students were requested to fill the RSES questionnaire in the school itself.
The RSES scale [15] consisted of 10 items regarding self-esteem. Each item was rated on a four-point response scale, one being ‘strongly agrees’ and four ‘strongly disagrees’. Five items were positively worded (item 1, 3, 4, 7, 10) and five were negatively worded (item 2, 5, 6, 8, 9). The scores for the positively worded items in the analysis were inversed so that a score of one (‘strongly agree’) was set to four. After adding the total item scores, overall score was obtained in between 10-40 with higher score indicating higher self-esteem. To differentiate between participants with high and low self-esteem, the participants were allocated to a high RSES group and a low RSES group based on the mean RSES score. Participants with a score of 31–40 were assigned to the high RSES group and participants with a score of 30 or below were assigned to the low RSES group, similar division was conducted by Ozhayat EB [11]. This division is in agreement with other studies dividing the RSES score into high and low self-esteem groups [16,17].
Statistical Analysis
The descriptive and inferential analysis of the data was done by using IBM SPSS. Statistics Windows, Version 20.0. (Armonk, NY: IBM Corp). For comparing self-esteem of cases and controls according to 10 RSES questions, t-test is used. Odds ratio (OR) was utilized to assess and compare the self-esteem according to high and low esteem in cases and controls.
Results
Out of the 212 students who were examined with dental trauma, most common type of fractures belong to Ellis class I which accounted to 53.3% followed by Ellis Class II (33.49%), Ellis Class III (13.20%). The maxillary arch was the most affected (72.48%) which included central incisors, lateral incisors and canines. In the mandibular arch, central incisors (19.8%) were the most affected [Table/Fig-2].
Traumatized anterior teeth and types of injured teeth.
| Types of injury | N | % |
|---|
| Ellis class I | 113 | 53.3 |
| Ellis class II | 71 | 33.49 |
| Ellis class III | 28 | 13.20 |
| Types of injured teeth | N | % |
| Maxillary central incisors | 99 | 46.69 |
| Maxillary lateral incisors | 24 | 11.3 |
| Maxillary canine | 28 | 13.2 |
| Mandibular central incisor | 42 | 19.8 |
| Mandibular lateral incisor | 19 | 8.96 |
N= Number
The main causes of tooth injury were sports (40.09%), falls (28.77%), traffic accidents (18.8%) and violence (12.26%). TDI reported among males and females were 69.33% and 30.66% respectively [Table/Fig-3].
Etiology of traumatic dental injuries among males and females.
| Causes | Male (147) | Female (65) | Total (212) |
|---|
| N | % | N | % | N | % |
|---|
| Road traffic accident | 29 | 13.67 | 11 | 5.18 | 40 | 18.8 |
| Sports | 57 | 26.89 | 28 | 13.20 | 85 | 40.09 |
| Falls | 41 | 19.34 | 20 | 9.4 | 61 | 28.77 |
| Violence | 20 | 9.43 | 6 | 2.8 | 26 | 12.26 |
N= Number
The ten items of RSES scale were answered by all the students (212 cases and 424 controls) in the study which were helpful in determining their self-esteem [Table/Fig-4]. Total mean score in cases (23.16) and in controls (24.43). This difference was statistically significant (p< 0.01). The controls had 5.23 times higher self-esteem than cases and low self-esteem is 2.44 times more in controls than cases (p<0.01) [Table/Fig-5].
Rosenberg’s Self-Esteem Scale (RSES) scale in cases and controls.
| Self-esteem | Cases (with anterior dental trauma) 212 | Control (without anterior dental trauma) 424 | t-test | p-value |
|---|
| Mean±SD | Mean±SD |
|---|
| On the whole, I am satisfied with myself | 2.25±0.75 | 2.41±0.88 | 2.27 | 0.02* |
| At times I think I am no good at all | 2.52±0.69 | 2.47±0.68 | 0.87 | 0.38 |
| I feel that I have a number of good qualities | 2.14±0.73 | 2.22±0.65 | 1.40 | 0.16 |
| I can do all that things which other people can do | 2.11±0.79 | 2.37±0.88 | 3.63 | <0.01* |
| I have not done such things in my life that someone feels proud on me | 2.53±0.84 | 2.55±0.82 | 0.29 | 0.77 |
| I certainly feel useless at some point of time | 2.59±0.85 | 2.57±0.89 | 0.27 | 0.79 |
| I feel that I am a person of worth, at least on an equal plane with others. | 2.25±0.85 | 2.65±0.81 | 5.77 | <0.01* |
| I wish I could have more respect for myself. | 1.91±0.78 | 1.94±0.56 | 0.56 | 0.58 |
| All in all, I am inclined to feel that I am a failure | 3±0.97 | 2.90±0.74 | 1.44 | 0.15 |
| I take a positive attitude toward myself. | 1.88±0.85 | 2.35±0.93 | 6.18 | <0.01* |
| Total | 23.16±3.10 | 24.43±3.94 | 4.10 | <0.01* |
*denotes highly significant differences of RSES question between cases and controls (p<0.05)
The high and low self-esteem in cases and controls.
| Self-esteem | Cases (with anterior dental trauma)Mean±S.D | Control (without anterior dental trauma)Mean±S.D | Odd Ratio(OR) | p-value |
|---|
| High esteem | 30.58±1.73 | 34.33±3.06 | 5.23 | <0.01* |
| Low esteem | 25.87±3.34 | 23±2.83 | 2.44 | <0.01* |
* denotes highly significant results (p<0.01)
Discussion
The present study is distinctive, as it investigates the effect of TDI on self-esteem (measured by RSES scale) among adolescents with and without TDI. The greatest strength and advantage of this population-based comparative study was matching, which ensured that the groups were similar with regard to important confounding factors. In addition, the 2:1 control-to-case ratio was used to reduce the impact of different clinical dental status, which could influence the perception and significance of the ultimate impacts. Besides that, using such a design provided a valid estimation of the association between the condition, untreated fractured teeth and the impact on the self-esteem of the adolescents, so that a judgment could safely be made concerning the generalization of the results to that population.
Despite the progress made on the development of measures of oral health outcomes for adults, little work has been done among adolescents and moreover there is no published research particularly on impact of TDI on adolescent’s self-esteem.
Teeth are an important part of the individual’s life as beautiful set of teeth gives the owner immense confidence and could be a good selling point for certain career paths [18]. When anterior teeth are affected, not only the individual become self-conscious of his/her dental appearance, but also visible differences may be more readily seen by others during daily social interactions [19]. Consequently, adolescents with fractured incisors were significantly more dissatisfied with the appearance of their teeth than were adolescents without any traumatic injury.
Ellis Class I was the most common type of injury in the cases (53.3%). This finding corroborates previous researchers like Tumen EC et al., [20] who found that the Ellis Class I fracture dominated (65.9%) followed by Ellis Class II fracture (12.2%). However, Kovacs M et al., [21] showed that the most common fracture in permanent teeth was the Ellis Class II fracture, followed by the Ellis Class I fracture.
TDI usually occur in the anterior segment and have a significant role in physical and psychological health [22]. This study found that permanent incisors were most affected by TDI (60.82%). In comparison, Ingle NA et al., in Chennai [23], Traebert J et al., in Fllorianopolis [24], Adekoya CA et al., in sub-urban Nigerian adolescents [25] found much less prevalence of TDI to the permanent incisors (almost 9-20%).
In the present study, the most frequently traumatized teeth were maxillary incisors (60.82%), amongst which maxillary central incisor (45.41%) was the most affected, which was similar to various other studies [23,20,26]. The reason may be ascribed to the fact that maxillary central incisors are generally more protruded than the mandibular teeth and tend to be the first to receive a direct blow producing a fracture and are less protected. In addition, the maxilla is fixed to the skull which makes it rigid, while the mandibular, being a flexible part, tends to reduce the impact forces directed on the mandibular anterior teeth by movement. Least traumatized tooth in the current study was found to be mandibular lateral incisor (7.91%) whereas in another studies, the least traumatized tooth was mandibular canine [23, 27].
In the hierarchy of causes, this study found that on most occasions dental injuries are caused by sports, followed by falls, road traffic accidents and violence. This may be due to the reason that all sporting activities have an associated risk of orofacial injuries due to falls, collisions and contact with hard surfaces. Few studies reported falls to be the more common reason for TDI [21,28,29]. On the contrary, other studies reported fights and violence to be more common [30].
Current study found that males (69.33%) suffer trauma almost twice as frequently as females (30.66%). These findings were similar to many other studies [25,31]. In yet another study, the frequency of the TDI of males was increased to four times more than of females [23]. This is probably reliant on the fact that boys are more active and they practice more aggressive sports. Thus, sports such as judo, boxing, cycling, athletics, hockey and polo are more frequently practiced by boys, whereas girls generally prefer dancing or swimming. Even while practicing more dangerous sports, such as handball or basketball, girls appear more cautious than boys.
The results of this comparative study showed that the adolescents with TDI (cases) experienced more impacts on their self-esteem than adolescents with no TDI (controls). Cases were more likely to report an impact for items ‘I can do all that things which other people can do’, ‘I feel that I am a person of worth, at least on an equal plane with others’, ‘all in all I am inclined to feel that I am a failure’ and ‘I take a positive attitude toward myself’ than controls, proving that cases had lower self-esteem than controls.
Cortes MIS et al., [32] found that adolescents with TDI had lower self-esteem and are more likely to report a negative impact on eating and enjoying food; smiling, laughing and showing teeth without humiliation and enjoying contact with people, compared to those without such injury. In addition, adolescents with TDI are more likely to feel worthless and inferior, shy, unhappy, sad or depressed and are less likely to be friendly compared with those without oral health problems.
Few other studies reported that dental trauma often causes permanent damage and may create problems that last for years after the accident. Furthermore, when dental trauma occurs in anterior teeth, most individuals respond in a more emotional way, due to the direct association with self-esteem and self-image which may lead to psychological health problems [33,34].
Dental trauma can mainly cause decreased appetite and depression and increased inattention and distractibility, which in turn may negatively impact self-esteem and may lead to school failure [35].
Lower self-esteem in cases may also be due to peer relationships which play a major role in the adolescent’s emotional separation and emerging individuality. Adolescents often seek out peers whose beliefs, values and even behaviours are similar. Thus, the need to balance peer pressure creates new challenges, tensions as adolescents begin to make independent decisions but, being unable to do so subsides their self-esteem. So, treating the traumatized tooth can be a boon for these adolescents (cases) and they may feel equivalent to the controls.
Limitation
Limitation of the study is the possible homogenized sample of this study. Moreover, as the present research did not use X-rays to assess TDI, there is some possibility that this prevalence is underestimated. Also concussions and subluxations are mild injuries which tend to solve themselves, but they may result in radiographic signs such as root resorption, pulp canal obliteration or periapical radiolucency (pulp necrosis). Also, root fractures are only found in radiographic exams. The study was based on completion of a self-administered questionnaire by 10–19 year olds; the response may be subjectively affected by the age of the participants, especially those of 10 years of age. Further studies are needed to assess the long term socio-psychological effects of dental injuries. These studies should include measures of interpersonal relationships, as well as education and work. Finally, it is also important to assess the impact of treated dental injuries.
Conclusion
Adolescence is a period when some childhood health problems may be determined, new issues may emerge and probability of risks for some longterm adult health problems which may lead to deprived self-esteem. The results in the present study showed that children with TDI showed poor self-esteem. This poor self-esteem may lead to loss of individual’s self-confidence in himself/herself. It can be overcome by providing oral health education to the adolescents at school level. Health promotion programs in schools can help adolescents establish good healthy habits avoid those that may lead to traumatic injuries. Therefore, by improving oral health in schools may contribute considerably to the self-esteem of individuals in a positive direction and help them in becoming a socially competent adult.
N= Number
N= Number
*denotes highly significant differences of RSES question between cases and controls (p<0.05)
* denotes highly significant results (p<0.01)