Perilunate Dislocation – Case Report and Review of Literature
Karthik Subramanian1, Bakul Arora2, Abhinav Bhatnagar3, Imran Jan4
1 Consultant, Department of Orthopaedics, Hira Mongi Navneet Hospital, Mumbai, Maharashtra, India.
2 Consultant, Department of Orthopaedics, Currae Hospital, Thane, Mumbai, Maharashtra, India.
3 Consultant, Department of Orthopaedics, Abhinav Multispeciality Hospital, Nagpur, Maharashtra, India.
4 Registrar, Department of Orthopaedics, Rajawadi Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Karthik Subramanian, 1701, Happiness Building, City of Joy Complex, JSD Road, Mulund (West), Mumbai-400080, Maharashtra, India.
E-mail: dr.karthik_1@yahoo.co.in
Perilunate dislocations are rare injuries comprising of less than 10% of all wrist injuries. These usually occur after high-energy trauma to the wrist. One-fourth (25%) of perilunate dislocations are missed at the initial presentation. We report a case of perilunate dislocation in a patient who presented late, about two months after trauma. He underwent open reduction through a single dorsal approach and internal fixation with K-wires. Aggressive physiotherapy exercises were started after removal of K-wires. He regained near normal full range of motions at the wrist by the end of four months and showed no recurrence of the dislocation. In conclusion, perilunate dislocations should be considered as one of the important differential diagnosis in patients with history of high-energy trauma to the wrist. Early diagnosis and treatment is necessary to prevent the potential risk of avascular necrosis of lunate and scaphoid and secondary osteoarthritis. The best results can be obtained with open reduction and internal fixation with K-wires via a single dorsal approach.
Avascular necrosis, Carpal injuries, Dorsal approach, Wrist injuries
Case Report
A 33-year-old adult male presented with a two-month-old history of sustaining injury to his right wrist, following history of Road Traffic Accident (RTA) and fall on his outstretched hand. He did not take any medical treatment following the injury and presented to the hospital after two months, due to persistent pain in his right wrist and inability to perform his daily routine activities.
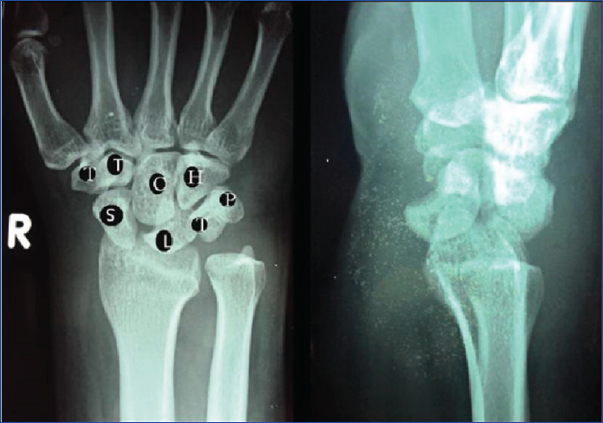
On examination, there was tenderness over carpal bones. The wrist movements were grossly restricted. There were no distal neurovascular deficits. Conventional radiographs of the wrist joint (anteroposterior and lateral views) showed increased scapholunate interval in the anteroposterior view and characteristic ‘spilled teapot sign’ in the lateral view [Table/Fig-1].
Radiograph of the right wrist (anteroposterior and lateral views) showed increased scapholunate interval in the anteroposterior view and characteristic-spilled teapot sign in the lateral view. Proximal row (from left to right): S – scaphoid, L – lunate, T – triquetrum, P – pisiform. Distal row (from left to right): T – trapezium, T – trapezoid, C – capitate, H – hamate.
Computed Tomography (CT) scan of the wrist with 3D reconstruction views showed dorsal subluxation of the distal carpus with loss of congruity of the articular surfaces and confirmed the diagnosis of perilunate dislocation [Table/Fig-2]. After obtaining preoperative fitness, the patient underwent open reduction of the dislocation.
CT scan with 3D reconstruction films showed loss of congruity of the articular surfaces and confirmed the diagnosis of dorsal perilunate dislocation.

Dorsal approach to the wrist joint between the 3rd and 4th extensor compartments was used. The perilunate dislocation was reduced and fixed with three K-wires through scapholunate, capitolunate and triquetrolunate junctions. The reduction was confirmed under C arm intraoperatively. The scapholunate ligament and dorsal capsule was meticulously sutured. The skin and subcutaneous tissues were approximated and the joint was immobilized in Below Elbow (B/E) slab. The patient was encouraged to actively move the fingers immediately postoperatively.
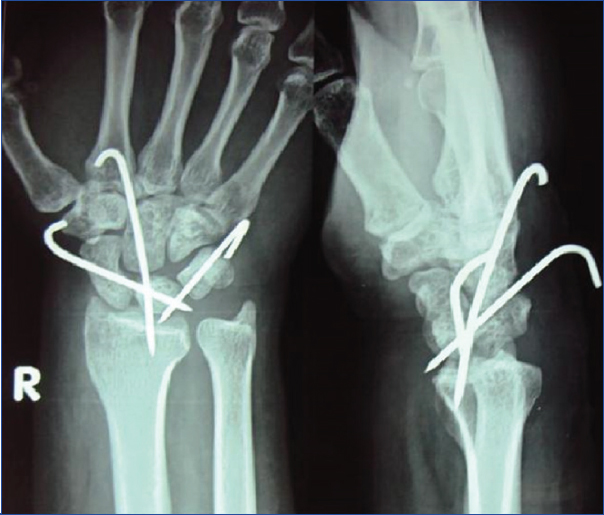
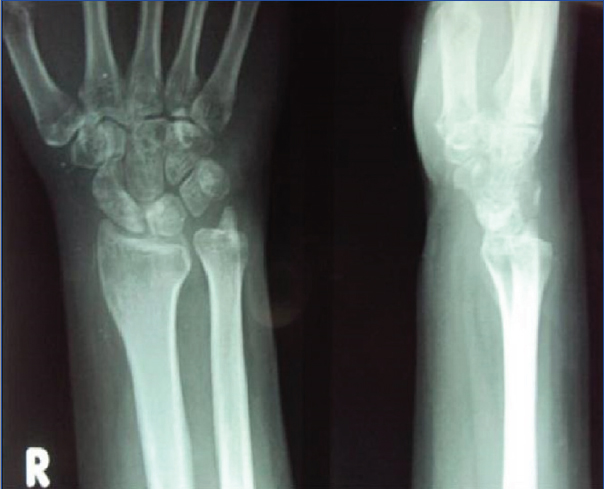
The postoperative radiograph showed satisfactory reduction of the dislocation by the K-wires [Table/Fig-3]. After suture removal, a short B/E cast was applied. The cast and the K-wires were removed after six weeks and the patient was put on physiotherapy sessions. The patient was followed up at regular intervals and his recent radiograph at the completion of nine months showed satisfactory alignment of the carpal bones and no recurrence of the dislocation [Table/Fig-4]. Clinically, the patient recovered near normal range of movements at the wrist joint by the end of four months.
Immediate radiograph of the right wrist joint showed reduction and fixation of the dislocation with the three k-wires in situ.
Nine months follow up radiograph of the right wrist joint showed satisfactory alignment of the carpal bones and no recurrence of the dislocation.
Discussion
Perilunate Dislocations (PLD) are rare injuries. They constitute less than 10% of all wrist injuries [1]. According to Aitken AP and Nalebuff EA, the most common mechanism of sustaining this injury is fall onto a hyperextended wrist with or without the forearm in supination [2].
Few researchers showed, that the disruption of ligaments due to perilunate dislocation follows the progressive perilunate instability pattern of joint derangement, classically disrupting the scapholunate, capitolunate and lunatotriquetral joints. Stage I results in scapholunate instability. Stages II to IV result in progressively worse perilunate instability [3]. Thus, the arc of disruption of ligaments starts radially and extends to the ulnar side of the carpus. The distal row dislocates in a dorsal or dorsoradial direction followed by the entire scaphoid and triquetrum in pure perilunate dislocations. When the perilunate ligaments rupture, because of the stronger palmar ligaments, the lunate usually remains within the radiocarpal joint and the remainder of the carpus dislocates, usually dorsally [3].
Perilunate dislocations are commonly missed injuries either due to lack of careful clinical examination at the time of initial presentation or due to delayed presentation by the patient Pappas ND et al., briefly described the necessity to detect such injuries at an early stage and to prevent its complications such as wrist stiffness and post-traumatic arthritis [4]. Herzberg G et al., conducted a study which emphasized that delay in treatment adversely affects the functional outcome of the patient [3].
The soft tissue damage coupled with late treatment has the potential risk of median nerve injury, avascular necrosis of scaphoid and lunate and post-traumatic osteoarthritis [4-7]. Gellman H et al., reported on a late presenting dorsal trans-scaphoid, transtriquetral, perilunate wrist dislocation [8]. Grissis P et al., described a neglected trans-scaphoid, transstyloid, volar dislocation of lunate which presented after six weeks post injury [5]. In Herzberg’s series of perilunate dislocations, 23% of the patients presented with acute carpal tunnel syndrome and 33% of those with missed diagnosis went on to present with carpal tunnel syndrome [3].
Adequate clinical history and careful physical examination will help in early detection of these injuries [4]. Careful scrutiny of radiographs is essential with attention to the Gilula’s arc of the carpal joints, scapholunate interval, scaphocapitate and capitolunate angles [5]. The typical radiographic appearances of a perilunate dislocation include disruption of the proximal and distal outlines of the proximal carpal rows. On the lateral view, the lunate no longer articulates with the head of the capitate, but appears palmarly rotated, the so-called ‘spilled teapot sign’ [5]. CT scan and 3D reconstruction films are helpful in confirming the diagnosis.
Early surgical management of these injuries result in a better functional outcome as compared to conservative line of management. Bagheri F et al., in their study, found similar results [6]. Combined dorsal and volar surgical approach to the wrist joint has usually been advocated for the management of this injury [9-11]. However, single dorsal approach helps to preserve the palmar wrist ligaments to the maximum with minimal surgical soft tissue damage [9]. It also gives good exposure of the proximal carpal row, mid-carpal joint and helps in earlier functional return of the patient [5]. Various implants have been used for stabilisation of the dislocation after reduction such as compression screws, cerclage wires and K-wires [9,11]. In our case, we treated by open reduction and internal fixation with percutaneous K-wires via a single dorsal approach. Adequate regular follow up of the patient is essential to prevent recurrence of carpal instability.
Conclusion
Perilunate dislocations although rare, should be considered as one of the important differential diagnoses in patients with history of high-energy trauma to the wrist. Early diagnosis and treatment is necessary to prevent the potential risk of avascular necrosis of the carpal bones. These injuries should therefore be ruled out while examining a patient presenting with wrist pain after high-energy trauma incidents. Adequate radiographs supplemented with CT scan and 3D films are useful in confirmation of the diagnosis. The best results can also be obtained with open reduction and internal fixation with K-wires via a dorsal approach.
[1]. Dobyns JH, Linschield RL, Fractures in adults 1984 2ndednPhiladelphiaJB Lippincott:411-509. [Google Scholar]
[2]. Aitken AP, Nalebuff EA, Volar transnavicular perilunar dislocation of the carpusJBJS 1960 :1051-1057. [Google Scholar]
[3]. Herzberg G, Comtet JJ, Linschied RL, Amadio PC, Cooney WP, Stadler J, Perilunate dislocations and fracture dislocations a multicenter studyJ Hand Surg 1993 18(A):768 [Google Scholar]
[4]. Pappas ND, Lee DH, Perilunate InjuriesAm J Orthop 2015 September44(9):E300-02. [Google Scholar]
[5]. Grissis P, Christodoulou A, Chalichlis B, Pournaran J, Neglected transscaphoid, transstyloid volar dislocation of lunateJ Bone Joint Surg Br 2006 88:676-80. [Google Scholar]
[6]. Bagheri F, Taraz-Jamshidi MH, Birjandinejad A, Sharifi-Daloei SR, Mirkazemi M, Meysam Choghadeh F, Trans scaphoid perilunate fracture dislocation and isolated perilunate dislocations;surgical versus non surgical treatmentArchives of Bone and Joint Surgery 2013 1(2):74-77. [Google Scholar]
[7]. Forli A, Courvoisier A, Wimsey S, Corcella D, Moutet F, Perilunate dislocations and transscaphoid perilunate fracture-dislocations: a retrospective study with minimum ten-year follow upJ Hand Surg Am 2010 35:62-68. [Google Scholar]
[8]. Gellmann H, Schwartz SD, Botte MJ, Felwell L, Late treatment of dorsal transscaphoid, transtriquetral, perilunate wrist dislocation with avascular changes of lunateClin Orthop Relat Res 1988 237:196-203. [Google Scholar]
[9]. Mario M, Roman P, Milan M, Treatment of trans-scaphoid perilunate dislocations using a volar approach with scaphoid osteosynthesis and temporary kirschner wire fixationMilitary Medicine 2011 176(9):1077-82. [Google Scholar]
[10]. Capo JT, Corti SJ, Shamian B, Nourbakhsh A, Tan V, Kaushal N, Treatment of dorsal perilunate dislocations and fracture dislocations using a standardized protocolHand 2012 7(4):380-87. [Google Scholar]
[11]. Trumble T, Verheyden J, Treatment of isolated perilunate and lunate dislocations with combined dorsal and volar approach and intraosseous cerclage wireJ Hand Surg Am 2004 29(3):4127 [Google Scholar]