Microfilariae of Wuchereriabancrofti in Testicular Aspirate
Anil Kumar Verma1, Ashok Kumar Kapoor2, Manish Singh3
1 Assistant Professor, Department of Pathology, School of Medical Sciences and Research, Sharda University, Greater Noida, Uttar Pradesh, India.
2 Pathologist, Department of Pathology, RML Mehrotra Pathology Ltd, Lucknow, Uttar Pradesh, India.
3 Pathologist, Department of Pathology, RML Mehrotra Pathology Ltd, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashok Kumar Kapoor, Pathologist, Department of Pathology, RML Mehrotra Pathology Ltd, Nirala Nagar, Lucknow-226020, Uttar Pradesh, India.
E-mail: drashokkapoor2016@gmail.com
Present study deals with results of fine needle aspiration of both the testes in a patient with azoospermia. Surprisingly, aspiration of right testis revealed large number of microfilariae in the smears. Conversely, left testicular aspirate showed few spermatogonia. However, microfilariae were not detected in venous blood smears. Findings of this study suggested possible role of Wuchereriabancrofti in causation of azoospermia.
Aspiration biopsy, Azoospermia, Filariasis
Case Report
Present report relates to the results of Fine Needle Aspiration (FNA) of right testis in a patient with azoospermia. A patient, aged 25 years, was married for the last five years. Couple was suffering from primary infertility. Semen analysis showed grayish white turbid fluid. Its volume was ~5 ml. Microscopic examination did not show spermatozoa. Repeated semen examinations revealed azoospermia. Bilateral testicular FNA of spermatic cords were done under local lignocaine anaesthesia. About 0.5 ml of clear transparent fluid was aspirated from right testis. Smears were fixed in ethyl alcohol and stained using conventional Haematoxylin&Eosin (H&E) technique. Later, smears were microscopically examined.
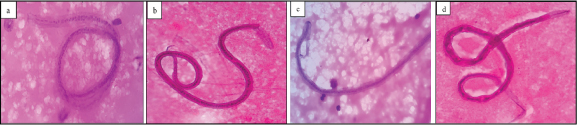
To our surprise, large number of microfilariae of Wuchereria bancrofti (~ 450 larvae in 0.5 ml of aspirate) was seen [Table/Fig-1a-d]. Differential leucocyte count of these smears revealed neutrophils- 24%, lymphocytes-70%, monocytes-05% and eosinophils-01%. We interpreted blockage of right vas deferens by dilated lymphatics, fibrous tissue and newly formed lymphatics. Aspirate from left testis did not show microfilaria. Left testicular aspirate was haemorrhagic and it contained few spermatogonia alone. Moreover, microfilariae were not detected in venous blood smears. The patient was diagnosed as a case of chronic filarial orchitis. This patient did not have any testicular swelling. No other positive finding was detected in this patient. He was treated with diethylcarbamazine 100 mg for six weeks and doxycyclin 200 mg for seven days. This patient could not be followed further.
a) Shows microfilaria, spermatogonia and few inflammatory cells (H&E-20X). b) Shows a microfilaria and few inflammatory cells (H&E-40X). The curves of microfilaria were round with broad cephalic end. c) Larvae had double row of nuclei (H&E-100X). d) Nuclei did not extend upto the tip of tail end of parasite, suggesting a diagnosis of Wuchereria bancrofti (H&E-40X).
Discussion
A few cases have been reported earlier where microfilariae were aspirated in testicular aspirate [1]. In the current case, microfilariae were aspirated in right testicular aspirate without having microfilariae in left testicular aspirate and in venous blood smears. However, filariasis has been reported earlier without microfilariaemia [2]. Elevated levels of IgE are known to develop following exposure to filarial infection [3]. Small amounts of IgE antibody may persist for many years [3]. Specific IgE antibody may have a role in clearance of microfilariae from circulation. Wucheraria bancrofti also carry Wolbachia endosymbionts which may help the parasite to survive [4]. It appears that lymphangiectasia (dilated lymphatics) develops due to adult worms of Wuchereria and their products while fibrosis develops following immune inflammation [5].
Conclusion
Thus, in the present case of a patient with azoospermia the smear examination showed large number of microfilariae of W. bancrofti, suggesting possible role of lymphatic dilatation and fibrosis in chronic filarial orchitis. Further, elimination of Wolbachia following doxycyclin treatment results in improvement in filarial lymphedema. Recovery from oedema occurs subsequent to formation of new lymphatics.
[1]. Ahmad SS, Hassan MJ, Akhtar K, Arif SH, Naim M, Rahman K, Microfilariae in testicular fine aspiration cytologyJK Science 2004 10(4):199-200. [Google Scholar]
[2]. Sivakumar S, Role of fine needle aspiration cytology in detection of microfilariae: Report of 2 casesActa Cytol 2007 51:803-06. [Google Scholar]
[3]. Mitre E, Nutman TB, IgE memory: Persistence of antigen-specific IgE responses in human filarial infectionJ Allergy Clin Immunol 2006 117:939-45. [Google Scholar]
[4]. Anthony RM, Rutizky LI, Urban JF, JuniorStadacker MJ, Gause WC, Protective immune mechanisms in helminth infectionsNature Reviews 2007 7:975-87. [Google Scholar]
[5]. Bennuru S, Nutman TB, Lymphatics in human lymphatic filariasis: In vitro models of parasite-induced lymphatic remodeling 2009 7(4):215-19. [Google Scholar]