Implant dentistry is the most contemporary treatment option in replacement of single tooth, multiple teeth or a full mouth rehabilitation. Most important factors for success of implant is the treatment planning, surgical skill and prosthetic preparation techniques [1]. Single tooth implant presents a different clinical situation considering the biomechanics involved in comparison with single natural tooth. There is very limited movement in the range of 10 μm in implants because of lack of periodontal ligament and osseointegration of implant [2].
Misfit of the prosthesis, limited implant movement and lack of implant flexure can cause implant or prosthesis failure. An accurate impression and passive fit of the prosthesis with implant abutment is a primary factor in enhancing the fitting precision, hence ensuring the success of treatment [3].
The idea is to minimize the microrotation of coping inside the picked impression to enhance the accuracy of impression in single tooth implant. Roughening of the surface of pickup impression copings with application of tray adhesive can be done to achieve a firm bonding between coping and impression material [4].
So, considering the importance of accurate impressions for single tooth implant, this study was conducted to achieve satisfactory results while transfer of impressions to the master cast. The present study was aimed at evaluating the difference in microrotation of internal hex of implant and implant analog between the acrylic resin model and three groups of master casts replicating the reference models respectively, using four different surface treatments of impression copings.
Materials and Methods
Fabrication of the samples was done in Himachal Dental College, Sundernagar (Himachal Pradesh, India) and the evaluation of the samples was done at Jawaharlal Nehru Government Engineering College Sundernagar Mandi, (Himachal Pradesh, India). This in vitro study was carried out in following phases: (1) Fabrication of reference model, (2) Fabrication of test specimens and (3) Testing of samples under profilometer to evaluate the rotational accuracy of the implant analog. Test specimens were divided into four groups depending on the type of surface treatment of impression coping as following: Group I (samples with non-modified impression copings), Group II (samples with impression copings coated with adhesive recommended for polyvinylsiloxane impression material), Group III (samples with impression copings modified by placing vertical slots and coating with adhesive for polyvinylsiloxane impression material) and Group IV (samples with impression copings sandblasted with 50 μm aluminum oxide powder and coated with recommended adhesive for polyvinylsiloxane impression material).
Fabrication of Reference Model
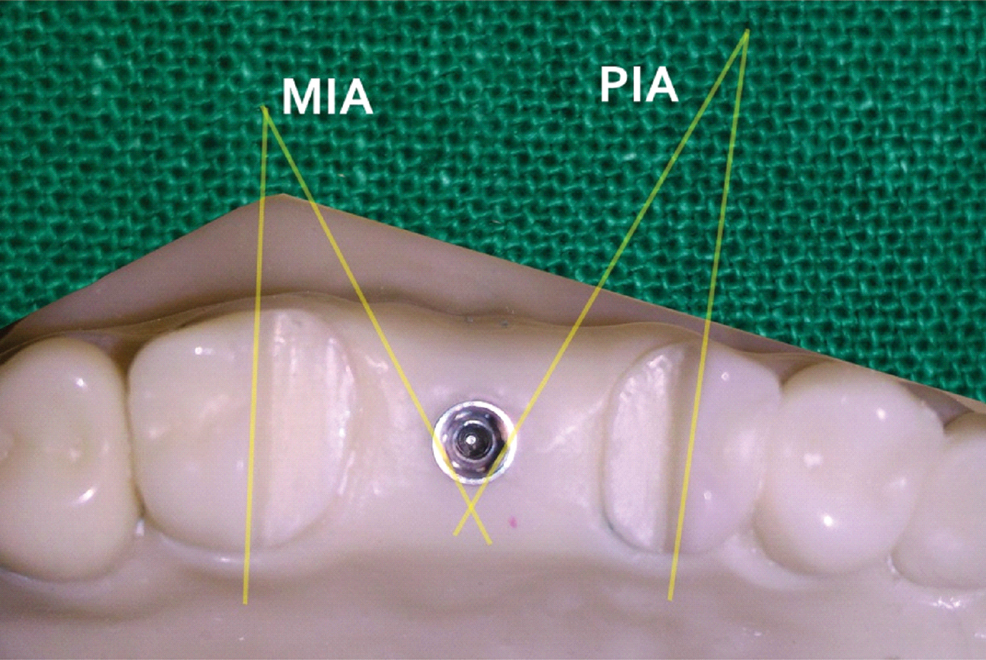
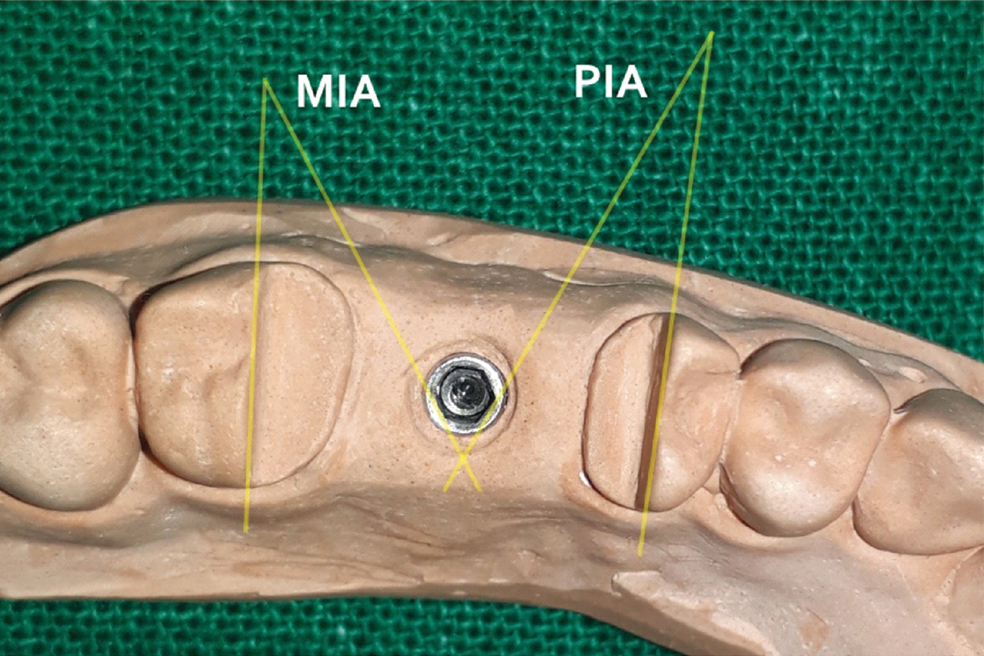
An acrylic resin dentulous model of maxillary arch was fabricated with an internal connection 4 mm x 10.5 mm implant (BioTEC, Dental implant systems, Germany) in 16 region to simulate a clinical situation. For fabrication of the reference cast, tooth 16 was removed from typodont and vacant socket was filled with modeling wax and contoured in shape of ridge. Then putty wash impression (Putty and Affins, Coltene Whaledent) was made of the typodont and was poured in blue inlay wax (Pyrax, Roorkee, India). The wax model of the typodont was retrieved from impression and was checked for any defects. Implant was placed in middle of edentulous region, keeping one of the sides of internal hex horizontal to the palatal side edentulous ridge in anterioposterior direction. Tooth 17 and 15 were cut in buccopalatal direction using warm BP blade to get two references planes parallel for measurement of the angles formed with sides of the implant hexagon serving as corresponding second plane of respective side. One angle was formed by the molar plane and the distopalatal side of the implant hexagon (MIA) and the other formed from the premolar plane and the mesiopalatal side of the implant hexagon (PIA). An impression coping was attached to the implant body. The whole wax pattern with implant and attached impression coping was flasked and cured in heat polymerizing PMMA tooth colored resin (DPI Heat Cure, Bombay Burmah Trading Corporation Ltd.). The impression coping was removed and resin model was finished and polished which was used as reference model [Table/Fig-1].

Fabrication of Customized Tray
An impression was made of the reference model and was poured in Type IV dental stone. Double layer wax spacer of total thickness of about 2 mm (Modeling wax, Pyrax, Roorkee, India), was applied to the stone model and tissue stops were cut to allow consistent thickness of impression material. Separating medium was applied and a uniform layer of autopolymerizing PMMA resin was applied extending to the vestibule but not covering the palate. After completion of the curing, the wax spacer was removed and a window was made with tungsten carbide bur in the region of implant to allow access for the impression coping. Four such customized impression trays were made by the same procedure.
Fabrication of Test Specimens
Impression copings were subjected to various surface treatments to achieve different surface modification. In Group I samples, impression copings were left untreated. Group II samples were fabricated with impression copings modified by application of tray adhesive only. Group III samples were fabricated with impression copings modified by placing four vertical grooves evenly spaced around the impression coping and coated with adhesive. Group IV samples were fabricated with impression copings sandblasted using clean 50 μm aluminum oxide powder at 2.5 atmospheric pressure and coated with adhesive [Table/Fig-2,3,4 and 5]. For fabrication of test specimens, the treated impression copings were secured to implant on reference model with hex driver. The impression trays and impression copings were coated with tray adhesive according to the manufacturer’s recommendation before each impression was made. Light body (Affins, ColteneWhaledent) was injected around the implant and impression coping and customized tray loaded with unset putty (Affins, ColteneWhaledent) was placed. After completion of polymerization of impression, hex driver was used to loosen the impression coping and the impression was removed. Impression was checked for any discrepancies. Implant analog was secured to the impression coping and cast was poured with Type IV die stone to make test specimens. [Table/Fig-6]. A total of 60 samples were made (15 samples for each group). The samples were studied under Profile projector (Dynascan ModelPH300E) to evaluate the microrotation of internal hex of the implant analogs. The angles MIA and PIA of reference model were compared with those formed in test specimen [Table/Fig-7,8]. Since these angles involved the distopalatal and mesiopalatal sides of internal hex of implant, any microtation, either clockwise or anticlockwise was detected by profile projector and evaluated for accuracy of its position along its long axis.
Resin model with unmodified impression coping (Group I).

Resin model with unmodified impression coping with tray adhesive application (Group II).
Resin model with impression coping with vertical slots and tray adehsive application (Group III).
Resin model with sandblasted impression coping and tray adhesive application (Group IV).
Die stone experimental sample model with implant analog in place.

Reference angles formed by molar plane and premolar plane with internal hex implant.
Angles formed by molar plane and premolar plane with internal hex implant analog.
Statistical Analysis
The obtained data was analyzed by using One-way ANOVA test and Student’s unpaired t-test to determine which group produced more accurate impressions.
Results
The value for resin master model for MIA and PIA was 22.9811° and 26.9014° respectively. The mean MIA and PIA values of the impression copings from all the groups as compared to the master resin model were analysed. The mean values for the various groups showed MIA and PIA varied from highest value 23.46247° and 26.42003° respectively in Group I and least in Group IV with values 22.5759° and 27.3066° for MIA and PIA respectively. Group IV showed minimum deviation in comparison to the master model. This can be shown as percentage difference of mean values [Table/Fig-9]. One-way ANOVA did not revealed any significant differences for both the MIA and the PIA between the definitive casts obtained from the Groups I, II, III and IV [Table/Fig-9]. Student’s unpaired t-test revealed no significant difference in the mean MIA and PIA of non-modified group (Group I) and modified groups (Group II, III and IV) when compared with standard measurement of resin master model [Table/Fig-10].
One-way ANOVA of Molar Implant Angles (MIA) and Premolar Implant Angles (PIA) measured on the definitive casts obtained with four different surface treatments.
| Angles | Group | N | Mean | SD | Min. | Max. | ANOVA |
|---|
| F | p-value |
|---|
| MIA | I | 15 | 22.26 | 2.23 | 18.11 | 26.13 | 1.18 | 0.33 |
| II | 15 | 22.42 | 2.01 | 19.21 | 25.79 |
| III | 15 | 23.41 | 1.81 | 20.33 | 25.69 |
| IV | 15 | 22.58 | 0.96 | 21.12 | 23.70 |
| PIA | I | 15 | 27.62 | 2.23 | 23.75 | 31.78 | 1.18 | 0.33 |
| II | 15 | 27.46 | 2.01 | 24.10 | 30.68 |
| III | 15 | 26.48 | 1.81 | 24.19 | 29.55 |
| IV | 15 | 27.31 | 0.96 | 26.18 | 28.77 |
| MIA(% change) | I | 15 | 3.13 | 9.72 | -13.69 | 21.22 | 1.18 | 0.33 |
| II | 15 | 2.45 | 8.77 | -12.20 | 16.43 |
| III | 15 | 1.84 | 7.88 | -11.79 | 11.54 |
| IV | 15 | 1.76 | 4.18 | -3.14 | 8.12 |
| PIA (% change) | I | 15 | 2.67 | 8.30 | -18.13 | 11.70 | 1.18 | 0.33 |
| II | 15 | 2.09 | 7.49 | -14.04 | 10.43 |
| III | 15 | 1.58 | 6.73 | -9.86 | 10.07 |
| IV | 15 | 1.51 | 3.57 | -6.94 | 2.68 |
Student’s unpaired t-test of Molar Implant Angles (MIA) and Premolar Implant Angles (PIA) measured on the definitive casts obtained with four different groups.
| One-sample test |
|---|
| Test value = 22.98 |
|---|
| Groups | Reference angle | t | df | Sig. (2-tailed) | Mean difference | 95% Confidence interval of the difference |
|---|
| Lower | Upper |
|---|
| I | MIA | -1.245 | 14 | 0.234 | -0.71797 | -1.9549 | 0.5190 |
| II | -1.079 | 14 | 0.299 | -0.56119 | -1.6768 | 0.5545 |
| III | .909 | 14 | 0.379 | .042509 | -0.5780 | 1.4282 |
| IV | -1.627 | 14 | 0.126 | -0.40401 | -0.9366 | 0.1286 |
| Test value = 26.90 |
| I | PIA | 1.249 | 14 | 0.232 | 0.72049 | -0.5165 | 1.9575 |
| II | 1.084 | 14 | 0.297 | 0.56375 | -0.5519 | 1.6794 |
| III | -.904 | 14 | 0.382 | -0.42258 | -1.4257 | 0.5806 |
| IV | 1.638 | 14 | 0.124 | 0.40675 | -0.1258 | 0.9393 |
* Non Significant
Discussion
Among the various steps involved in fabrication of implant prosthesis, accurate impression and working casts are essential to conventional prosthodontic procedures. In implant dentistry, the goal in making impression is to record and precisely transfer the position of implant in relation to its spatial orientation. Most of implants have an internal or external geometrical configuration that helps securing the implant analog to precise position by preventing rotation [4,5].
The direct or the open tray impression technique was used in the present study which involves unscrewing of the implant analog intraorally after the impression material has set and then securing the implant analog to its position before pouring the working cast. This step is very critical, failure to which can lead to further complications.
Various studies have shown that there is always some possibility of rotation of the impression coping which can lead to error in precise fitting of the prosthesis. This led to the idea of improving the retention and stability of impression coping by altering the surface of impression coping. Surface treatments have proved to cause surface roughness increasing the surface area which indeed leads to better mechanical interlocking thereby resulting in more retention. This justifies why incorporating the external surface of impression copings with surface treatments leads to improved retention between the coping and the impression material, thus minimizing the risk of rotational movement during impression making [3,6]. Considering this fact, more studies were required to validate the use and benefits of surface treating impression copings for accurate records of transfer copings. So, this study was carried out which aimed at investigating the transfer of the orientation of the internal hex of implant to the working cast using direct transfer impression technique with different surface treatment of impression copings.
The results of the study found no significant difference in the mean PIA and mean MIA of non modified group (Group I) and modified groups (Groups II, III and IV) when compared with standard measurement of resin master model.
In the present study, the mean MIA and PIA values of the experimental group’s master casts showed variations from those recorded on the resin master model. This gives an idea that there is always a possibility of microrotation while using transfer copings which can lead to three-dimensional spatial inaccuracies in the master casts. The results also show that the surface modification definitely reduces the error of microrotation and hence improves the accuracy of the master cast. Group in which copings were sandblasted and adhesive was applied showed minimum deviation from the acrylic resin model while maximum deviation was shown by the samples of group where the impression copings were not subjected to any surface treatment.
The percentage change in MIA and PIA among the four groups showed highest variation in non-modified group and least in sandblasted followed by adhesive coated samples [Table/Fig-9]. This reveals that homogeneity in Group IV was more as compared to other groups which further indicate that this group produces casts which are more accurate and closest to that of the resin master model.
The mean MIA and mean PIA between non modified group and the modified group were compared. No significant difference was found. However, in copings sandblasted and adhesive coated copings there is least variation indicated by the standard deviation as shown in [Table/Fig-10]. Though, all the modifications had shown better results with less degree of microrotation.
From the results, it can be assumed that the sand blasting of the impression coping followed by coating of adhesive for polyvinylsiloxane impression material had an edge over the non modified copings and other modifications of copings, which was in agreement with the earlier study done by Vigolo P [3], probably because of increased contact by roughened surface and application of adhesive to increase bonding of impression material with the coping [3,6]. This reduction in error will consequently lead the lab technician to fabricate prosthesis with precision with reduced chances of error clinically. Similar but non significant results were found with other groups also.
Limitation
Possible limitations of the present study design were that the measured distortions did not completely evaluate the actual three-dimensional distortion of the impressions. Only the discrepancies in axial rotations of the components were detected and not the angulation of the implant body. Under clinical conditions, these differences may vary if the discrepancies are present in other spatial planes. Thus, such discrepancies may clinically result in a improper fit of the prosthesis. Therefore, further studies may be required to evaluate and rectify the problem in more depth considering the limitation of previous and our present study to achieve practically relevant methods for the clinical applications. The study suggests the use surface modification of impression coping for open tray technique for single implant cases to achieve master cast for prosthesis that have better passive fit intraorally hence, mechanically and biologically in harmony.
Conclusion
Within the limitations of this study, the some conclusions were drawn. Though, statistically non-significant, all types of surface treatments of the impression copings showed more accurate transfer than those without any modification. Sandblasted and adhesive coated impression copings showed minimum amount of rotation followed by vertical slots incorporated and adhesive coated impression copings. Surface treatment can help to achieve more accurate master casts.
* Non Significant