In recent years, there has been a dramatic increase in the geriatric population worldwide and more old people are alive nowadays than at any time in history. According to a survey done in 2001, there were 71 million elderly persons above 60 years of age in India. This number is expected to increase to 179 million by 2031 [1].
The tendency of ocular diseases to occur increases at around 40 years of age. Ocular morbidity shows a steep increase after the age of 60 years [2]. According to projections, by 2050, 80% of the elderly population will be living in low and middle income countries [3]. Health promotions and curative and rehabilitative services for the visually impaired elderly population should therefore be a priority in the coming years especially in low and middle income countries.
According to a study done by Singh MM et al., among the elderly population in Central India, the most common cause of ocular morbidity at that time was refractive error (40.8%), followed by cataract (40.4%) [2]. However, over the past 20 years we have seen a major increase in cataract surgery rates. Also, the advancements in cataract surgeries and intraocular lenses have ensured better visual outcomes and minimal post operative complications. According to a few recent studies from across the country, corneal disorders and glaucoma are emerging as the major causes of ocular morbidity in the geriatric population [4].
Considering the complicated epidemiology of visual impairment, region specific intervention strategies are required for every community [5]. Therefore, comprehensive studies of the changing trends of geriatric ocular problems are required to reduce the load of ocular morbidity. Hence, this study was undertaken to examine the changing pattern of major causes of blindness and visual impairment in the elderly population of Northern India and to determine the socioeconomic status in relation to ocular morbidities.
Materials and Methods
This population based cross-sectional study was conducted from December 2015 till December 2016 in the field practice area of the peripheral centres of Christian Medical College and Hospital, Ludhiana, North India. The study was approved by the Hospital Ethical Committee. A team from the Department of Ophthalmology and Community Medicine conducted house visits and the subjects were interviewed and examined after obtaining an informed consent. The study population included subjects >60 years of age residing in these areas. The study included 900 eyes of 450 subjects, selected by systematic random sampling from the data base available with the Department of Community Medicine.
Detailed information about the socio demographic characteristics, presence of ocular complaints, relevant past history, family history and history of any systemic disease was recorded. Kuppuswamy’s modified scale was used to determine the socioeconomic status of the subjects [6] Unaided and aided visual acuity was recorded for each subject using Snellen E chart. Presenting visual acuity between 20/60 (6/18) and 20/200 (6/60) in the better eye was defined as visual impairment and a presenting visual acuity of <20/200 (<6/60) in the better eye was defined as blindness. Improvement of vision using pin hole was recorded. Anterior segment examination was done using torch light and magnifying loupe of 6x magnification. Fundus examination with undilated pupils was done for all subjects using direct ophthalmoscope. All patients with history or clinical findings suggestive of retinal diseases or glaucoma underwent dilated fundus examination. Intraocular pressure using Schiotz indentation tonometer was recorded for subjects with history of glaucoma or family history of glaucoma or suspicious optic disc.
Statistical Analysis
Sample size was calculated using OpenEpi, version 3, open source calculator-SSPropor. Sample size comprised of 450 subjects at confidence interval – 97% taken into account, non response of 10% in the community.
The data was entered using Epidata Entry software 3.01 and analysed using Epidata Analysis 2.2.2 from Epidata Association, Denmark. Proportions, Chi-square and Fisher’s exact test were used for summarizing the data [7].
Results
The study included 450 subjects of which 53.6% (241) were females and 46.4% (209) were males.
The age and gender distribution of the subjects is shown in [Table/Fig-1]. Maximum number of subjects were in the 60-69 years age group (62.7%). Out of 450 subjects, 19.3% were diabetics and 32.2% were hypertensives. Visual impairment and blindness was seen in 30% (135) subjects and 8% (36) subjects respectively. There was a statistically significant (p-value <0.001) relationship between increasing age and the number of visually impaired and blind individuals as shown in [Table/Fig-2]. Out of 209 males, 63.1% had normal vision, 30.7% had visual impairment and 6.2% were blind. Out of 241 females, 61.0% were normal, 29.5% were visually impaired and 9.5% were blind. There was no statistically significant difference between distributions of visual acuity according to gender in our study.
Age and gender distribution of the study population.
| Age in years | Female (%) | Male (%) | Number (%) |
|---|
| 60- 69 | 153 (54.3) | 129 (45.7) | 282 (62.7) |
| 70- 79 | 67 (53.2) | 59 (46.8) | 126 (28.0) |
| 80 and above | 21 (50.0) | 21 (50.0) | 42 (9.3) |
| Total | 241 (53.6) | 209 (46.4) | 450 (100.0) |
Comparison of visual acuity in different age groups.
| Age Group (years) | Normal (%) | Impaired (%) | Blind (%) | Total |
|---|
| 60- 69 | 200 (74.9) | 67 (25.1) | 15 (7.0) | 282 (100.0) |
| 70- 79 | 62 (53.0) | 55 (47.0) | 9 (12.7) | 126 (100.0) |
| 80 and Above | 17 (56.7) | 13 (43.3) | 12 (41.4) | 42 (100.0) |
Chi-square= 46.45 df (4) p-value <0.001
Visual morbidity was found to be more in individuals with low socioeconomic status and it was statistically significant in our study (p-value = 0.0015) as shown in [Table/Fig-3].
Effect of socioeconomic status on visual morbidity (Impaired + Blind).
| SES | VA 20/20-20/40 (%) Normal | VA less than 20/60 (%) Impaired + Blind | Odd’s Ratio |
|---|
| I | 7 (2.5) | 1 (0.6) | 1 |
| II | 45 (16.1) | 16 (9.4) | 2.49 |
| III | 68 (24.4) | 29 (16.9) | 2.99 |
| IV | 149 (53.4) | 120 (70.2) | 5.64 |
| V | 10 (3.6) | 5 (2.9) | 3.5 |
| Total | 279 (100.0) | 171 (100.0) | |
Extended Mantel- Haenszel Chi-square for linear trend = 9.98
p-value = 0.0015, SES- Socioeconomic Status, VA- Visual Acuity
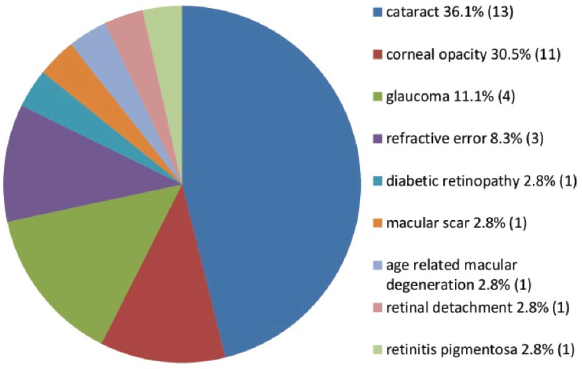
The most common cause of blindness in our study was cataract accounting for 36.1% followed by corneal opacity 30.5%, glaucoma 11.1%, refractive error 8.3%, diabetic retinopathy 2.8%, macular scar 2.8%, Age Related Macular Degeneration (ARMD) 2.8%, retinal detachment 2.8% and retinitis pigmentosa 2.8% [Table/Fig-4].
Causes of blindness in the study population.
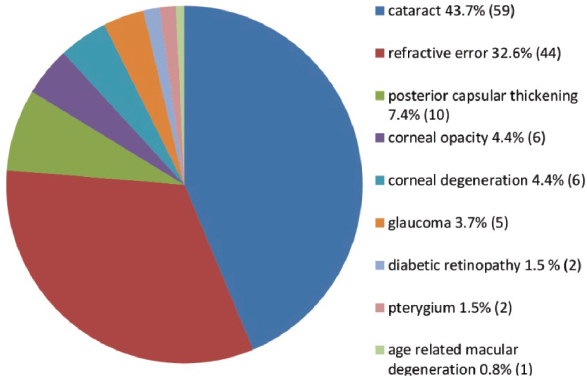
Among the various causes of visual impairment cataract accounted for 43.7%, refractive error 32.6%, posterior capsular thickening 7.4%, corneal opacity and corneal degeneration 4.4% respectively, glaucoma 3.7%, diabetic retinopathy 1.5%, pterygium 1.5%, ARMD 0.8% [Table/Fig-5].
Causes of visual impairment in the study population.
The ocular morbidity rate was 2.13 lesions per eye. The number of lesions/eye was 2.18, 2.24 and 1.71 in the age groups 60-69 years, 70-79 years, 80 years and above respectively.
Discussion
Population ageing is a global phenomenon. Today, India is in a phase of demographic transition. There is a transition from high birth and death rate to lower birth and death rate [8]. This will eventually lead to a transformation in the age structure of our population. In India the elderly population has increased from 20 million in 1951 to 57 milllion in 1991 [9]. This number is expected to increase to 179 million by 2031 [1]. Most of this increase in elderly population is from the unorganized sector with no social security [9].
India has thus acquired the label of “an ageing nation” with 7.7% of its population being more than 60-year-old. Therefore, there is an urgent need for health education programs and studies targeting geriatric population.
In our study, blindness was seen in 8.0% (36) and visual impairment in 30% (135) of the individuals. Similar results were shown in a study done by Pisudde PM et al., [10]. The prevalence of blindness (12.2%) and low vision (32%) as reported in a study by Singh MM et al., in 1997 was higher than our study [2]. The main causes of visual morbidity in their study were cataract and refractive error. The prevalence of blindness has decreased since the 90’s, as is also evident from the study by Haq I et al., [5]. Our study also supports these statistics. The reason for this decrease in prevalence of blindness could be that cataract and refractive errors due to surgical aphakia, the main causes of ocular morbidity in the 90’s are being effectively dealt with now, due to the various advancements in cataract surgery and intraocular lenses. Free and subsidized cataract surgical services and improved intraocular lens are being provided by the government and NGO sector as well.
The need of the hour is to deal with other causes leading to blindness and visual impairment along with cataract.
Amongst the various causes of blindness in the elderly population cataract accounted for 36.1% in our study. Blindness due to cataract seen in studies done by Puri DS et al., Murthy GV et al and Li J et al., was 53.8%, 82.6%, 70.5% respectively [11-13]. The difference as discussed earlier is most likely due to improved cataract surgical rate and better availability of ophthalmic services.
The second most prevalent cause of blindness in many less developed countries is corneal diseases but epidemiological data is limited [14].
In India, it is estimated that there are approximately 6.8 million people who have vision less than 6/60 in at least one eye due to corneal diseases; of these, about a million have bilateral involvement. It is expected that the number of individuals with unilateral corneal blindness in India will increase to 10.6 million by 2020 [14]. In our study, it was seen that 30.5% blindness was due to corneal diseases. Corneal blindness has significantly increased in elderly population from 3% in 1997 [2] to 14.7% in 2001 [15]. The major causes of corneal morbidity in the elderly include trachomatous keratopathy, corneal degenerations and trauma-induced infectious keratitis. To effectively plan a preventive, promotive and rehabilitative blindness control strategies a Continued assessment of the burden of corneal blindness with periodic review of trends is required.
Glaucoma accounted for 11.1% of blindness in our study. In a study done by Vijaya L et al., in rural south India glaucoma accounted for 4.29% of blindness [16]. According to Andhra Pradesh Eye Disease Study the rate of bilateral blindness because of primary open angle glaucoma was 11.1% and angle closure glaucoma was 16.6% [17,18]. The difference in the rate may be due to difference in the age groups in these studies, also in many rural areas, accurate diagnosis and effective treatment for glaucoma is still out of reach and so is underestimated. The National Blindness survey 2001 showed that glaucoma is the third major cause of blindness in India and responsible for 5.9% of blindness (VA <6/60). There has been a more than threefold increase in proportion of glaucoma blindness compared to that found in the previous National survey in 1986-1989 [19] and similar results were seen in our study. Thus, for glaucoma awareness in the community, health education campaign is needed, in which the patients should be motivated and guided for regular follow-up and continuation of treatment. Complicated cases should be referred to tertiary level hospitals.
The most common cause of visual impairment in our study was cataract (43.7%) followed by refractive error (32.6%). Our results were similar to the studies done by Murthy GV et al., (50.3%) in Gujarat and Li J et al., (53%) in China [12,13].
The number of patients with cataract is decreasing because of increased cataract surgical rate, however, the most common complication that is posterior capsular thickening remains a significant problem which was responsible for 7.4% visual impairment in our study and 4% in a study done by Nangia V et al., resulting in suboptimal outcome of cataract surgery [20].
Diseases of cornea are increasingly becoming a common cause of visual morbidity. In our study corneal opacity (4.4%) and corneal degeneration (4.4%) were responsible for 8.8% of visual impairment. In a study done by Haq I et al., the prevalence of corneal opacity was 4.2% [5]. In another study by Dandona L et al., visual impairment caused by corneal diseases accounted for 11.5% [21]. The difference in the prevalence rate in our study and study done by Haq I et al., and Dandona L et al., could be because of difference in age groups.
Glaucoma accounted for 3.7% visual impairment in our study and similar result was seen in the Botucatu Eye Study where glaucoma accounted for 2.2% of visual impairment [22]. A high incidence of pterygium was found in our study. This could be because people living in Punjab (Northern India) are mostly agriculturists and hence the duration of sun exposure throughout life is quite high.
A comparison of various studies on visual impairment and blindness done in India is shown in [Table/Fig-6] [2,3,5,10,12,15,20,23-25].
Comparison of various studies on blindness and visual impairment in India [2,3,5,10,12,15,20,23-25].
| Study | Year | Region | Sample Size | Age Group (years) | Low vision/ visual impairment (prva<6/ 18 - >6/60) | Blindness prva<6/60 | Ocular Morbidity rate (lesions per eye) | Causes of visual impairment and blindness |
|---|
| Singh MM et al., [2] | 1997 | Rural Central India | 903 | >50 | 32% (PRVA: 6/ 18-CF3m) | 12.2% (PRVA<CF3m) | 1.21 | RE:40.8%; Cataract:40.4%; Aphakia:11.1%;Pterygium:5.2%; Glaucoma:3.1%; CO:3.0% |
| Murthy GV et al., [15] | 2001 | Rural Bharatpur Rajasthan | 4,728 | >50 | | 11.9% | - | Cataract: 67.5%; Uncorrected Aphakia+RE:18.4% |
| Haq I et al., [5] | 2009 | Aligarh | 700 | >20 | 7.8% | 5.3% | - | Cataract: 21.7%; RE:13.5%; CO:4.2%; Glaucoma:0.9% |
| Murthy GVS et al., [12] | 2010 | Gujarat | 5,158 | >50 | 29.3% | 6.9% | - | Cataract: 82.6%; Retinal Ds:8.9%Causes of visual impairment: Cataract:50.3%; RE:35.4% |
| Singh A et al., [23] | 2012 | Allahabad | 9,736 | All age groups | - | 6.95% BCVA<3/60 | - | Cataract:41.89; uncorrected RE; 21.59%;Xerophthalmia:10.20%; Glaucoma:4.83%; Infective ds of eye:4.73%Elderly >60 yrs of age group Cataract/Aphakia/Pseudophakia:80.77%; Uveitis:16.67%; RE:14.43%;CO:14.29%; Infective ds of eye:11.36%;Glaucoma:4.44%; Xerophthalmia:4.21%;Others:17.86% |
| Nangia V et al., [20] | 2013 | Rural Central India | 4,711 | >30 | 27% | 2.5% | - | Cataract:75%; Posterior Capsular Opcification:4%;Surgical complications:2%; ARMD:2%; Macular Ds:1%;Glaucoma:1% |
| Marmamula S et al., [24] | 2013 | Andhra Pradesh | 494 | >50 | 35.6% | 21% | - | Cataract:57.1%; RE:26.4%; Posterior segment Ds:12.1% |
| Khadse A [25] | 2014 | Central India | 525 | All age groups | 40.38% | | - | Cataract:42.86%; CO:42.86%; RE:14.28% |
| Pisudde PM et al., [10] | 2015 | Maharashtra | 974 | >50 | 29.3% | 7.2% | - | RE: 85%; Cataract: 36.3%; Dry eye: 12.7%; DR:8.9%;CO: 6.9%; ARMD: 6.6%; Glaucoma: 5.6% |
| Kumar J et al., [3] | 2016 | Bundelkhand | 820 | >50 | 37% | 13.7% | 1.24 | RE:43.4%; Cataract:41.0%; Pterygium:18.8%;Aphakia:14.2; Glaucoma:3.7%; CO:3.2% |
| Present study | 2017 | Northern India | 450 | >60 | 30% | 8% | 2.13 | Cataract:36.1%; CO:30.5%; Glaucoma:11.1%;RE:8.3%DR:2.8%; Macular scar:2.8%; ARMD:2.8%;RD:2.8%; RP:2.8%Causes of visual impairment: Cataract:43.7%; RE:32.6%; Posterior CapsularOpcification; 7.4%; CO:4.4%;Glaucoma:3.7%; DR:1.5%; Pterygium:1.5%;ARMD:0.8% |
RE- Refractive Error, CO- Corneal Opacity, DR- Diabetic Retinopathy, ARMD- Age Related Macular Degeneration, PRVA- Presenting Visual Acuity, BCVA- Best Corrected Visual Acuity RD- Retinal Detachment, RP- Retinal Pigmentosa, ds- disease, CF3m-Counting fingers at three metres.
As shown in [Table/Fig-6], cataract and refractive errors were considered the leading causes of blindness. Today, as these morbidities are being dealt with promptly their prevalence has come down. Corneal diseases and glaucoma are emerging as the leading causes of blindness as shown in the recent studies (Singh A et al., Marmamula S et al.,) including our study [23,24]. The focus now needs to shift on these emerging causes of blindness. Hence, the health strategies and government policies need to focus on these more than cataract and refractive errors.
Epidemiological data on major blinding conditions are essential. Our study highlights an alarming high prevalence of blindness due to corneal diseases and glaucoma in Northern India which needs long term strategies. Development of screening procedures using simple diagnostic criteria can be utilized for training of paramedical workers and ophthalmic assistants for early detection of these conditions, timely referral and treatment.
Limitation
Sample size in the present study is less.
Conclusion
Pattern of ocular morbidity varies with age. There is limited data on the changing trends in the prevalence of blindness in the elderly population. Treatable blindness particularly due to cataract and refractive error has been reduced drastically. Though, these two conditions still are the major causes of visual impairment and blindness. Thus, it is apparent that cataract and refractive error should remain high priority in prevention of blindness programmes in India. However, increased emphasis is also necessary to eliminate corneal blindness and irreversible blindness due to glaucoma as these are fast emerging as the major causes of blindness in geriatric population as evident from our study and several other studies. This herald a need to define the priorities for eye care services based on the current population-based data. Short term emphasis should be placed on cataract and refractive errors and long term emphasis should include glaucoma and corneal diseases as well. People should be educated about their causes, preventive measures and appropriate treatment.
Chi-square= 46.45 df (4) p-value <0.001
Extended Mantel- Haenszel Chi-square for linear trend = 9.98p-value = 0.0015, SES- Socioeconomic Status, VA- Visual Acuity
RE- Refractive Error, CO- Corneal Opacity, DR- Diabetic Retinopathy, ARMD- Age Related Macular Degeneration, PRVA- Presenting Visual Acuity, BCVA- Best Corrected Visual Acuity RD- Retinal Detachment, RP- Retinal Pigmentosa, ds- disease, CF3m-Counting fingers at three metres.