Facial esthetics, Maxillary, Surgical
A 20-years-old male patient reported with chief complaint of enlargement of upper lip since last 10 years giving an unesthetic appearance and causing cosmetic problem for the patient.
On examination, the double lip was not visible at rest but became evident when the patient smiled or showed his teeth or attempted to stretch his lip. There was a midline constriction band between two bulges of the labial mucosa due to attachment of upper labial frenum [Table/Fig-1].
Preoperative view showing maxillary double lip.

There was no family history of double lip. The patient’s medical and dental histories were noncontributory and he did not report any abnormal parafunctional oral habits and there was no previous history of trauma to the area.
The patient reported with difficulty in speech and mastication, caused by the excess tissue. Oral examination revealed folds of redundant mucosal tissue occurring bilaterally on the mucosal surface of the upper lip [Table/Fig-2].
Preoperative close-up view showingfold of excess maxillary labial mucosal tissue.

The overlying mucosa was intact and of normal appearance. The lower lip was normal. The tissue was of soft consistency, mobile, fluctuant and non-painful when palpated. No other congenital defect was present and the remainder of the head and neck examination was also not relevant. There was no blepharochalasis (drooping) of the upper eyelids and no thyroid enlargement. So, the diagnosis of Ascher’s syndrome was ruled out.
A provisional diagnosis of congenital bilateral upper double lip was made, and surgical excision was suggested to the patient. The surgery was planned using transverse elliptical incisions.
The infraorbital nerve block was used bilaterally instead of local infiltration to avoid tissue distortion of the mass. The mass was demarcated and excised by transverse elliptical incisions from both commissures to the midline using sharp dissection taking care that normal lip tissue is not excised to avoid loss of lip dimension postoperatively [Table/Fig-3,4,5 and 6].
Diagrammatic illustration of surgical incision.

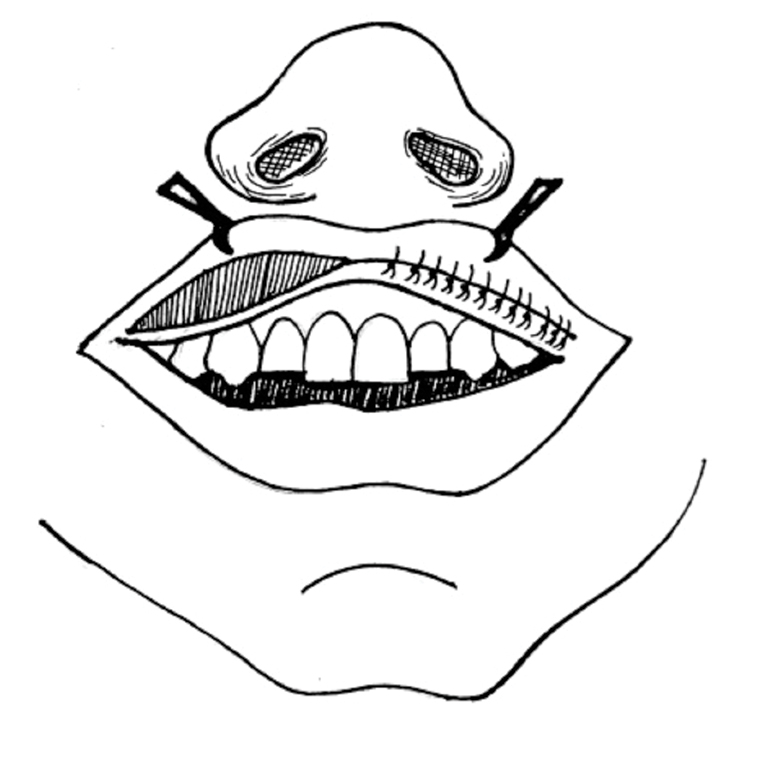
Diagrammatic illustration of suturing.
Surgical excision of the redundant labial mucosa on left side.

Surgical excision of the redundant labial mucosa on right side.

The surgical site was closed using 5-0 vicryl™ suture (Ethicon Johnson and Johnson Ltd.) [Table/Fig-7].
Suturing done using 5-0 vicryl suture.

Patient was instructed to avoid any trauma to the surgical area and to avoid any food that can cause stretching of the lip or tension on the suture line for three weeks.
Histopathologic examination of the excised specimen showed parakeratinised stratified squamous epithelium overlying dense fibrous connective tissue stroma. Numerous hyperplastic mucous glands and endothelial lined blood vessels dispersed throughout the stroma along with a few muscle fibres [Table/Fig-8].
Histopathological picture showing parakeratinised stratified squamous epithelium overlying dense fibrous connective tissue stroma with numerous hyperplastic mucosal glands.

The patient was reviewed after one week, then after one month and finally after three months of the treatment, healing was uneventful and no surgical complications or recurrence were noted. The patient was comfortable and satisfied with the outcome of the treatment [Table/Fig-9,10].
Postoperative view at one month showing good cosmetic results.

Postoperative view at three months showing no recurrence.

Discussion
Double lip is an oral anomaly which may be either congenital or acquired. It consists of a fold of excess or redundant tissue on the mucosal side of the lip. Often the tissue will project beyond the vermilion of the lip and take the form of a “cupid’s bow” when the upper lip is tensed or, in the case of the lower lip, it will form bilateral bulbous masses which project intraorally. The upper lip is involved more often than the lower, and rarely both the upper and lower lips are involved [1].
The upper lip mucosa, during development, consists of two transverse zones: an outer cutaneous zone (pars glabra) and an inner mucosal zone (pars villosa) [2]. The congenital form of double lip is thought to arise during the second or third month of gestation from a persistence of the sulcus between them [3]. The acquired form of double lip may occur due to trauma or any oral habit, and may develop in association with Ascher’s syndrome.
Clinically, double lip needs to be differentiated from other types of chronic enlargements of the lip. Macrocheilia may be neoplastic in nature, circulatory, or inflammatory. All these conditions, however, are associated with a uniformly enlarged lip without a transverse furrow dividing the vermilion portion of the lip [4].
The treatment of congenital double lip is indicated for esthetic concern as in our case or when excess tissue interferes with mastication or speech or leads to habits as sucking or biting the redundant tissue. Several surgical techniques have been described to repair double lip: W-plasty, electrosurgical excision and triangular excision, elliptical excision and laser [5]. The surgery resulted in good cosmetic results and no relapse was observed.
[1]. Barnett ML, Bosshardt LL, Morgan AF, Double lip and double lip with blepharochalasis (Ascher’s syndrome)Oral Surg Oral Med Oral Pathol 1972 34(5):727-33. [Google Scholar]
[2]. Ali K, Ascher syndrome: a case report and review of the literatureOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 :103,e26-e28. [Google Scholar]
[3]. Martins WD, Westphalen FH, Sandrin R, Campagnoli E, Congenital maxillary double upper lip: Review of the literature and report of a caseJ Can Dent Assoc 2004 70:466-68. [Google Scholar]
[4]. Schwimmer A, Dym H, Barr C, Surgical repair of a double lipJADA 1979 99:993-94. [Google Scholar]
[5]. Kanneboina LMY, Hadge P, Desai H, Smile makeover with double lip correction - case reportInternational Journal of Oral Care and Research 2015 3(3):86-88. [Google Scholar]