A Rare Case of Giant Solitary Neurofibroma of Abdominal Wall Masked by Pregnancy
Madhumita Patel1, Kumari Usha Rani2, Manjula Sharma3, Amar Bhatnagar4
1 Ex Senior Resident, Department of Obstetrics and Gynaecology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
2 Associate Professor and Senior Specialist, Department of Obstetrics and Gynaecology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
3 Professor and Consultant, Department of Obstetrics and Gynaecology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
4 Professor and Head, Department of Oncosurgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kumari Usha Rani, Associate Professor and Senior Specialist, Department of Obstetrics and Gynaecology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi-110016, India.
E-mail: drmadhumitapatel11@gmail.com, usharani10066@yahoo.com
Various types of neurogenic tumours can involve the abdomen. Retroperitonial space is most commonly affected but other sites can also be involved. Mostly younger age group is affected and malignant transformation is rare. CT and MRI are helpful in making diagnosis and planning surgery. Complete surgical excision is treatment of choice. Final diagnosis is made by histopathology and immunohistochemistry report. We report a rare case of giant solitary benign neurofibroma of anterior abdominal wall in 25-year-old multiparous women reported on day 15 of vaginal delivery with large abdominal mass which was masked before because of pregnancy.
Benign neurogenic tumour, Postpartum, Unencapsulated tumour
Case Report
A 25-year-old multiparous woman reported to the emergency ward of Obstetrics and Gynaecology with large abdominal mass on post natal day 15 of full term vaginal delivery. She had noticed a small mass one year ago which was initially the size of a lemon. It was painless but gradually increased in size. However, since within two months of noticing the mass, she was pregnant, she did not realize the increase in size of mass and ignored the same. Thereafter, she had an uneventful full term vaginal delivery. Post delivery she observed that mass was growing rapidly and was also causing pain. She also developed ulceration over the mass. She reported to hospital 15 days after delivery.
Her past medical, surgical and family history was uneventful. On examination, a large firm and tender mass occupying whole of the abdomen with overlying necrotic skin was observed [Table/Fig-1]. On vaginal examination, uterus and adnexa could not be commented because of painful huge abdominal mass.
Large abdominal mass (Post natal day 15).

Ultrasound was done which revealed large abdomino pelvic mass with heterogeneous texture but organ of origin could not be commented upon. Consequently, MRI abdomen was done which revealed a round well defined 40 x 20 x 20 cm mass arising from muscle of anterior abdominal wall with areas of superficial ulceration. Posteriorly the mass was displacing the peritoneum and its contents; however plane between the mass and peritoneum was maintained. Findings were suggestive of soft tissue tumour of anterior abdominal wall, and provisional diagnosis of desmoid tumour was made. Uterus and adnexa were normal in morphology.
Patient was taken up for wide excision of tumour along with oncosurgeon in view of clinical suspicion of malignancy. Preoperative laboratory investigations were within normal limits.
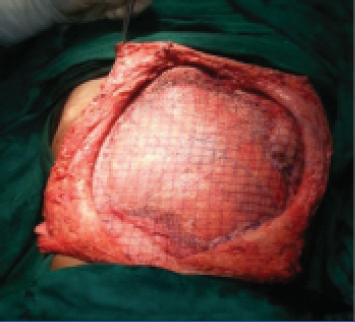
Intraoperatively 50 x 30 x 30 cm size of fungating growth was seen which was arising from anterior abdominal wall. It was covering almost the entire abdominal wall. Wide local excision of the mass was done along with full thickness abdominal wall [Table/Fig-2,3]. The defect was closed with onlay composite mesh [Table/Fig-4].
Surgical dissection of mass.

Complete surgical excision.

Grossly the tumour was ovoid in shape, firm in consistency and was covered by a smooth glistening layer. Cut sections showed gray tan glistening tumour with focal areas of necrosis and haemorrhage [Table/Fig-5].
Surgical specimen (cut section view).

Histopathological examination revealed an unencapsulated tumour which was composed of sheets and fascicles of tumour cells. The cells had spindle shaped nuclei with kinking of nuclear ends, few hypocellular and myxoid areas were also seen. Areas of haemorrhage and necrosis were present; however no significant mitosis was seen. These features were suggestive of benign neurogenic tumour.
This report was further supplemented by immunohistochemical analysis. On immunohistochemistry tumour cells were negative for SMA (ruled out soft tissue tumours of muscular origin like leiomyoma or desmoid tumour) and CD34 but showed focal positivity for S-100 which confirmed tumour of neural tissue (CD34 and S-100 both are marker of neurogenic tumour). Combined histopathology and immunohistochemistry reports were suggestive of benign neurofibroma.
Postoperative period was uneventful and there was no relapse till one year of follow up.
Discussion
Neurogenic tumours of abdominal wall are very rare and their association with pregnancy is even rare. There are various types of neurogenic tumour which can affect abdomen and they are classified as being of ganglion cell origin (ganglioneuromas, ganglioneuroblastomas, neuroblastomas), paraganglionic system origin (pheochromocytomas, paragangliomas), or nerve sheath origin (neurilemmomas, neurofibromas, neurofibromatosis, malignant nerve sheath tumours) [1-3]. In abdomen, these tumours are located mostly in retroperitoneal space, especially in the paraspinal areas and adrenal glands. However urinary bladder, gallbladder, bowel and abdominal wall are few other sites in the abdomen which are involved occasionally [3]. Majority of neurogenic tumours are benign and found in younger population.
A neurofibroma is a benign nerve sheath tumour in the peripheral nervous system. Neurofibromas are either solitary or associated with Neurofibromatosis type 1(NF-1) which is an autosomal dominant genetically inherited disease. When associated with NF-1, neurofibromas have tendency to grow larger and with high malignant potential [4]. Here we have reported a rare case of giant solitary benign neurofibroma of abdominal wall in 25-year-old postpartum women where its signs and symptoms were masked because of pregnancy. Very few cases of neurofibroma of abdominal wall have been reported so far [5] and on reviewing literature we have not found any case report of giant solitary neurofibroma of abdominal wall associated with pregnancy.
Neurofibroma and Neurilemmomas both are benign nerve sheath tumors which may be positive for CD34 or S100 or both. It can be differentiated by its characteristic features. Neurofibromas are unencapsulated tumours and nerve fibers runs through the tumour whereas neurilemmomas are capsulated tumours and nerve fibers course over the surface of tumour [6]. Grossly these are firm masses of varying sizes and histopathologically they are composed of cells of nerve sheath which are schwann cells, perineural cells, fibroblasts, myxoid matrix or mast cells [7].
Neurofibromas are further divided into three types which are solitary, diffused and plexiform. Solitary neurofibromas originate from cutaneous nerves and never associated with neurofibromatosis, diffuse one arises mostly from nerves in the subcutaneous tissue of head and neck and plexiform neurofibromas are diffuse masses with tortuous extensions along the parent nerve [8,9]. Symptoms depend upon size and location of the tumour, cutaneous tumour causes surface deformation while deeper masses causes destruction due to pressure exerted to nearby organs as well as neurological symptoms [10,11].
Different types of soft tissue tumours (tumour of muscles, ligaments, nerves and blood vessels) can be differentiated using immunohistochemical studies. Smooth muscle lesions like leiomyoma or leiomyosarcoma and myofibroblastic tumours like desmoid tumour are positive for SMA while for the identification of tumours of nerve cells; S-100 protein is a preferred marker [12].
Various soft tissue tumours which are CD34 positive are vascular tumours, DFSP, Solitary fibrous tumour, GIST, Spindle cell/ pleomorphic lipomas, some neural tumours and epithelioid sarcoma [13]. In a study conducted by Park JY et al., 73% neurofibromas were CD34 positive while it was negative in our case [14].
Conclusion
In case a female patient reports with abdominal mass; tumours arising from muscles, nerves, lymphatics and fat tissues should be kept in mind along with uterine, adnexal and other pelvic tumours. Neurogenic tumour of abdomen is rarely malignant. Radiologically these tumour manifests as a well-defined, smooth or lobulated mass. CT/ MRI findings of both benign and malignant tumours are similar except there is distant metastasis in malignant tumours. Complete surgical excision of these masses is advocated.
[1]. Shimada H, Ambros IM, Dehner LP, Hata J I, Joshi VV, Roald B, The international neuroblastoma pathology classification (the Shimada system)Cancer 1999 86:364-72. [Google Scholar]
[2]. Shields TW, Reynolds M, Neurogenic tumours of the thoraxSurg Clin North Am 1988 68:645-68. [Google Scholar]
[3]. Enzinger FM, Weiss SW, Soft tissue tumours 1988 2nd edSt Louis, MoMosby-Year Book:719-860. [Google Scholar]
[4]. Tahririan MA, Hekmatnia A, Ahrar H, Heidarpour M, Hekmatnia F, Solitary giant neurofibroma of thighAdv Biomed Res 2014 3:158 [Google Scholar]
[5]. Barajas-Gamboa JS, Flórez-Salamanca L, Solitary neurofibroma in the abdominal wall of a patient without neurofibromatosis:Case reportBiomédica [Internet] 2009 29(4):501-05. [Google Scholar]
[6]. Tsai CJ, Case report: Unusual ultrasonographic appearance of a solitary retroperitoneal neurofibromaBr J Radiol 1994 67:210-11. [Google Scholar]
[7]. Weiss SW, Goldblum JR, Weiss SW, Goldblum JR, Benign tumours of peripheral nervesEnzinger and Weiss’s Soft Tissue Tumours 2008 5th edSt. Louis, MoMosby:769-84. [Google Scholar]
[8]. Lin J, Martel W, Cross sectional imaging of peripheral nerve sheath tumours: Characteristic signs on CT, MR imaging, and sonographyAJR Am J Roentgenol 2001 176:75-82. [Google Scholar]
[9]. Chennakeshaviah G, Ravishankar S, Maggad R, Manjunath GV, Solitary giant intramuscular myxoid neurofibroma resulting in an above elbow amputationCase Reports in Pathology 2012 2012:353215 [Google Scholar]
[10]. Shaida A, Yung M, Neurofibroma of the pinnaEar Nose Throat J 2007 86:36-38. [Google Scholar]
[11]. Venadero F, Rodríguez M, Merelo V, Cervantes A, Ramos A, Solitary neurofibroma. Two cases reportRev Cent Dermatol Pascua 2004 13:99-102. [Google Scholar]
[12]. Shelat VG, Li K, Naik S, Ng CY, Rao N, Rao J, Abdominal schwannomas: Case report with literature reviewInt Surg 2013 98:214-18. [Google Scholar]
[13]. Al-Daraji W, Husain E, Zelger BG, Zelger B, A practical and comprehensive immunohistochemical approach to the diagnosis of superficial soft tissue tumoursInternational Journal of Clinical and Experimental Pathology 2009 2:119-31. [Google Scholar]
[14]. Park JY, Park H, Park NJ, Park JS, Sung HJ, Lee SS, Use of Calretinin, CD56, and CD34 for differential diagnosis of schwannoma and neurofibromaThe Korean Journal of Pathology 2011 45:30-35. [Google Scholar]