Femoral Hypoplasia with Unusual Facies Syndrome
Sreekanth R Shenoy1, Dipankar Mondal2, Manas Ranjan Upadhyay3, Bhupendra Kumar Gupta4, Jatadhari Mahar5
1 Junior Resident, Department of Paediatrics, SVPPGIP and SCB Medical College and Hospital, Cuttack, Odisha, India.
2 Junior Resident, Department of Paediatrics, SVPPGIP and SCB Medical College and Hospital, Cuttack, Odisha, India.
3 Assistant Professor, Department of Paediatrics, SVPPGIP and SCB Medical College and Hospital, Cuttack, Odisha, India.
4 Junior Resident, Department of Paediatrics, SVPPGIP and SCB Medical College and Hospital, Cuttack, Odisha, India.
5 Senior Resident, Department of Paediatrics, SVPPGIP and SCB Medical College and Hospital, Cuttack, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sreekanth R Shenoy, Room no 147, SR Hostel, SCB Medical College, Cuttack-753007, Odisha, India.
E-mail: sreekanthrshenoy80@gmail.com
Femoral facial syndrome is a rare clinical entity characterized by unilateral or bilateral femoral hypoplasia along with various malformations of face. Only few cases have been detected by antenatal ultrasonography so far. We present the case of one-day-old, male child, born to a primi gravida with oligohydramnios and severe growth restriction. The child had unusual facies with posterior cleft palate, non-communicating hydrocephalus and complete absences of left femur, hypoplasia of right femur, bilateral club foot and bilateral undescended testis.
Cleft palate, Diabetes, Oligohydramnios, Short limbs
Case Report
A one-day-old, male child born out of non-consanguineous marriage was admitted with respiratory distress and multiple congenital abnormalities in the form of posterior cleft palate, unusual facial characteristics and abnormal limb morphology. He was born to a G1PoLoAo mother by caesarean section at 36 weeks period of gestation for oligohydramnios. The mother was booked and had regular antenatal check-ups. During antenatal period there was no history of diabetes, first trimester exanthematous illness and feto-toxic medication intake. Antenatal USG done at 32 weeks of pregnancy, showed oligohydramnios and foetal hydrocephalus.
At admission the child had respiratory difficulty with a respiratory rate of 70/minute, subcostal and intercostal retraction, oxygen saturation of 92% in room air. The child had normal pulses in all the four limbs. Heart sounds were normal with a heart rate of 130 beats/ minute without any murmur, per abdomen examination did not reveal any organomegaly, but there was bilateral undescended testis. The child had normal hair, with a head circumference of 32.5cm (25th percentile) with normal sized, non bulging anterior fontanelle (2 × 2 cm). Both eyes were normal and the child had bilateral low set ears with deformed pinna. Nose was short and broad with long philtrum [Table/Fig-1], thin upper lip and posterior cleft palate. Neck was normal with bilateral short arms. Back and spine were normal. Both lower limbs were short, with left limb shorter than right limb by 2 cm with bilateral short thigh and bilateral club foot deformity.
Showing short broad nose with long philtrum, thin upper lip, low set ears and short lower limbs

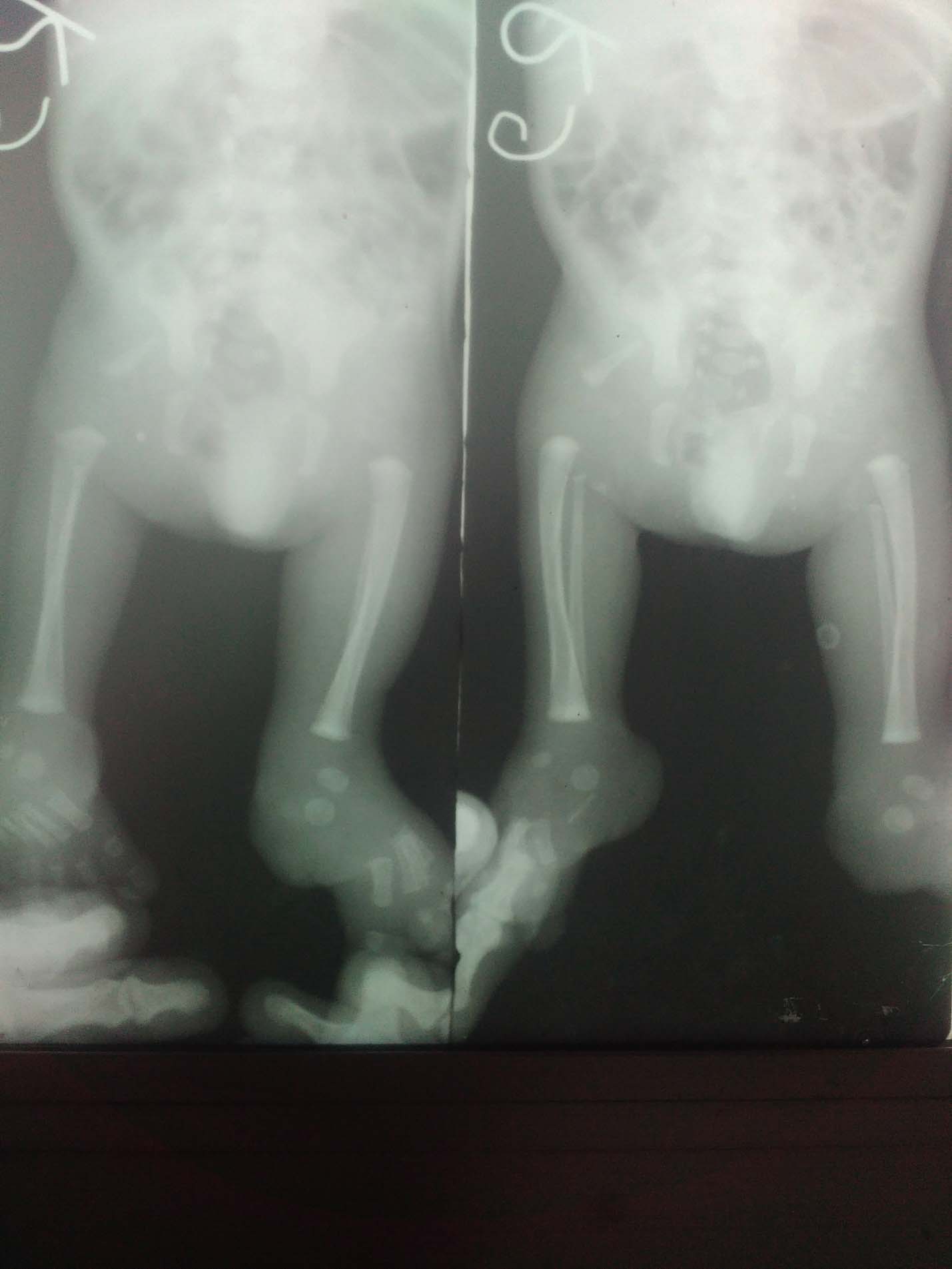
Investigations: Haemoglobin-16 mg/dl, Total Leukocyte Count (TLC)-13000/cc, Neutrophils-79%, Lymphocytes-16%, Eosinophils-4%, Monocytes-1%, CRP (quantitative) 1.48 mg /dl. Infantogram [Table/Fig-2] showed absent left femur and severe hypo plastic right femur, wide obturator foramen, ill formed acetabulum, shortening of sacral bodies, right superior radio ulnar joint dislocation. Trans cranial USG showed non-communicating hydrocephalus with poorly visualized corpus callosum. Trans abdominal USG showed bilateral small low placed kidneys.
Infantogram showing absence of left femur and small right-sided femoral bone.
Child was managed conservatively with injection ampicillin and gentamycin for five days, IV fluid and gradual build-up of expressed breast milk by tube feeding. Child was passing urine and stool normally during the hospital stay. He was discharged on request and subsequently lost to follow up.
Discussion
Femoral Facial Syndrome (FFS) or Femoral Hypoplasia-Unusual Facies Syndrome (FHUFS) is a rare syndrome, first reported in 1961 by Franz CH and O’Rahilly R consisting of asymmetrical hypoplasia of femur associated with abnormal facial charecterestics [1]. Further case reports on the same were put forth by Jones KL et al., and by DeanH DL et al., [2,3]. The aetiology of FFS is unknown. It closely resembles caudal dysplasia syndrome or sironomelia which occurs due to insufficient mesoderm in the caudal part of the embryo causing lumbosacral defects, lower limb dysplasia, renal agenesis, but facial anomalies are absent [4]. A disruption of normal carbohydrate homeostasis at a critical point of embryogenesis may be contributing in the development of femoral hypoplasia-unusual facies syndrome as well as in the development of caudal regression syndrome [5]. Although there have been reports of FFS with autosomal dominant inheritance, multifactorial inheritance is actually much more likely and most cases appears to be sporadic [6]. In 1984, Burn J et al., described case series of 13 patients with femoral hypoplasia of which six were consistent with a diagnosis of femoral facial syndrome [7]. Of these one was attributed to foetal constraint due to oligohydramnios, three were attributed to maternal diabetes, two were of undetermined aetiology. There are case reports suggesting an autosomal dominant pattern of inheritance [8]. In most of the reported cases there is associated maternal diabetes [9]. The syndrome consists of asymmetrical hypoplasia of femur associated with unusual facies with short nose long philtrum thin upper lip, micrognathia, cleft palate, low set poorly formed pinna, radioulnar joint anomalies, pelvic anomalies, cryptorchidism, polycystic or absent kidneys. Central nervous system anomalies in the form of corpus callosal agenesis have been reported [10]. Other features may include renal hypoplasia; genital anomalies including cryptorchidism, microphallus, hypoplastic labia, absent uterus and vagina with normal ovaries, bilobed lungs and hydrocephalus [11]. Verma A et al., reported additional features of the femoral facial syndrome in the form of encephalocoele, bilateral complete cleft lip, bilateral absence of fifth metatarsal and toe and penoscrotal hypospadias [12]. One case has been reported to be associated with autistic spectrum disorder [13]. In our case, there was associated severe oligohydramnios with associated dislocated right radio ulnar joint, bilateral club foot, bilateral small kidney which shows the extended spectrum of this disorder.
Conclusion
Femoral hypoplasia with unusual facies is a rare syndrome and may be associated with maternal diabetes or severe oligohydramnios. In our case oligohydramnios appears to be the cause. Antenatal ultrasonogram can be useful in the diagnosis by showing absent or short femur and foetal micrognathia. Femoral facial syndrome has varied clinical presentations. Apart from the characteristic femoral hypoplasia and facial clefting, bilateral club foot, dislocation of radioulnar joint can also be the presentation. Oligohydramnios may be the cause in the present case. It was also associated with bilateral small kidneys.
[1]. Franz CH, O’Rahilly R, Congenital skeletal limb deficienciesJ Bone & Joint Surg 1961 43A:1202-24. [Google Scholar]
[2]. Jones KL, Jones MC, Campo MD, Femoral hypoplasia-unusual facies syndromesmith’s recognizable patterns of human malformation 2013 7th EditionElsevier Saunders:410-13. [Google Scholar]
[3]. Daentl DL, Smith DW, Scott Cl, Hall BD, Gooding CA, Femoral hypoplasia-unusual facies syndromeJ Pediatr 1975 86:107-11. [Google Scholar]
[4]. Palit S, Ghosh S, Basu M, Mondal AK, Gayan S, Sengupta A, Femoral hypoplasia-unusual facies syndrome with atypical features: a rare case reportJ Anat Soc India 2004 53(1):22-24. [Google Scholar]
[5]. Tadmor OP, Hammerman C, Rabinowitz R, Fisher D, Itzchaki M, Aboulafia Y, Femoral hypoplasia-unusual facies syndrome: prenatal ultrasonographic observationsFetal Diagn Ther 1993 8(4):279-84. [Google Scholar]
[6]. Paladini D, Maruotti GM, Sglavo G, Penner I, Leone F, D’Armiento MR, Diagnosis of femoral hypoplasia–unusual facies syndrome in the fetusUltrasound Obstet Gynecol 2007 30(3):354-58. [Google Scholar]
[7]. Burn J, Winter RM, Baraister M, Hall CM, Fixsen J, The femoral hypoplasia-unusual facies syndromeJournal of Medical Genetics 1984 21:331-40. [Google Scholar]
[8]. Lampert RP, Dominant inheritance of femoral hypoplasia- unusual facies syndromeClin Genet 1980 17:255 [Google Scholar]
[9]. Johnson JP, Carey JC, Gooch WM, Petersen J, Beattie JF, Femoral hypoplasia—unusual facies syndrome in infants of diabetic mothersJ Pediatr 1983 102(6):866-72. [Google Scholar]
[10]. Orphanet: Femoral hypoplasia- unusual facies syndrome. [cited 2017 June 12]. Available from: http://www.orpha.net [Google Scholar]
[11]. Mundlos S, Horn D. Femoral-Facial Syndrome. In: Limb Malformations [Internet]. Springer Berlin Heidelberg; 2014 [cited 2017 Jun 14]. pp. 179–80. Available from: http://link.springer.com/chapter/10.1007/978-3-540-95928-1_69 [Google Scholar]
[12]. Verma A, Jain N, Jain K, Additional malformations in femoral hypoplasia with unusual facies syndromeIndian J Pediatr 2002 69(6):531-32. [Google Scholar]
[13]. Vecchio D, Salzano E, Vecchio A, Di Filippo T, Roccella M, A case of femoral-facial syndrome in a patient with autism spectrum disordersMinerva Pediatr 2011 63(4):341-44. [Google Scholar]