Influence of Post Angulation between Coronal and Radicular Segment on the Fracture Resistance of Endodontically Treated Teeth
Satheesh B Haralur1, Anas Abdullah Lahig2, Yahya Ahmed Al Hudiry3, Abdullah Hassan Al-Shehri4, Ahmed Abdullah Al-Malwi5
1 Associate Professor, Department of Prosthodontics, College of Dentistry, King Khalid University, Kingdom of Saudi Arabia.
2 Intern, College of Dentistry, King Khalid University, Abha, Asir, Saudi Arabia.
3 Intern, College of Dentistry, King Khalid University, Abha, Asir, Saudi Arabia.
4 Demonstrator, College of Dentistry, King Khalid University, Abha, Asir, Saudi Arabia.
5 Demonstrator, College of Dentistry, King Khalid University, Abha, Asir, Saudi Arabia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satheesh B Haralur, Associate Professor, Department of Prosthodontics, College of Dentistry, King Khalid University, Kingdom of Saudi Arabia.
E-mail: hb_satheesh@yahoo.com
Introduction
The objectives of coronal restoration in the Endodontically Treated Teeth (ETT) include rehabilitation of aesthetics, function and prevention of coronal leakage. The long axis of root and the coronal segment in the maxillary anterior teeth varies according to the occlusal scheme. The restorative dentist is required to fabricate the post angulation in compatibility to contour of the adjacent teeth.
Aim
To evaluate the influence of the angle between the long axes of core facial surface and the radicular segment of the post on fracture resistance of ETT.
Materials and Methods
Total of 30 maxillary intact canines was root canal treated, sectioned 2 mm above the CEJ. The custom made nickel-chromium endodontic posts were fabricated using direct method. The samples were divided among three groups of 10 each. The angle between coronal segment and radicular segment of post in Group-I, Group-II, Group-III were 5°, 10° and 15° respectively. The teeth samples were cemented with full veneer metal crown and tested under universal testing machine. The static load at the angle of 130° was applied until the fracture to record the fracture strength. The obtained data was statistically analysed with ANOVA and Tukey post-hoc test.
Results
The Group-III showed the highest fracture strength with 666.15 N. The Group-II and Group-I recorded the mean fracture strength at 443.37 N and 276.74 N respectively.
Conclusion
The endodontic post with higher angle between the long axis of facial surface and radicular segment long axis had the positive correlation to the fracture strength in ETT.
Post-endodontic restoration, Root canal therapy, Tooth crown
Introduction
The anterior teeth are critical for aesthetics, occlusal integrity and phonetics of an individual [1]. Compromised smile due to absent, fractured, or discoloured anterior teeth is known to cause the loss of self-esteem [2,3]. The loss or fracture of anterior teeth is most commonly observed in the age group between 15-30 years [4]. The etiologies for the tooth fracture include protruded teeth, fall, contact game injuries and road traffic accidents. The sizable number of tooth fracture occurrences leads to the pulpal injury and substantial tooth structure loss; necessitating root canal treatment. The post is routinely used in restoring the ETT with insufficient coronal tooth structure; it helps in anchoring the coronal restoration to the root canal [5]. Increased susceptibility of ETT for fracture is attributed to the reduced remaining tooth structure volume. The previous caries and restorations, added instrumentation, large-diameter posts are known to cause the loss of tooth structure [6]. The researchers have reported the insertion of the endodontic post and the material used for fabrication greatly influences the masticatory force distribution in ETT [7], consequently impacts its fracture strength.
Suitable coronal restoration over the ETT rehabilitates the aesthetics and function in addition to the prevention of coronal leakage [8]. The optimum crown or restorations in the anterior teeth should simulate the adjacent teeth in its shape, size, contour and colour. The longitudinal axes of the root and the coronal parts are different in the maxillary anterior teeth, the angulation of the root to the crown is known as the collum angle [9]. The researchers are of the opinion, the variations in angle between crown and root is vital for the satisfactory development of the dentition. The crown-root angle of maxillary anterior teeth is described to vary between different occlusal schemes; Class-II division-2 malocclusion reported to have the significantly higher collum angle [10]. In addition to crown- root angle, the labial surface of the anterior teeth is comprised of two planes [11]. The two plane labial surface in the anterior teeth enhances the aesthetic proportion of the teeth by reducing the visible segment. During the restoration of the ETT with post in the anterior teeth, dentists should take the crown- root angle and facial angle of the tooth into consideration. Since the fabrication of the endodontic post, following the long axis of the root will lead to proclined incisal edge position in the crown, incompatible contour and loss of incisal guidance. Hence, it is imperative on the restorative dentist to fabricate the post with similar crown-root angle of the adjacent teeth for optimum rehabilitation.
The effect of the post length, width and the ferrule over the fracture resistance is extensively studied by the researchers. Nevertheless, the effect of different angle between coronal to the radicular segment of the post on the fracture resistance of the ETT needs the further investigation. Hence, this in vitro study was designed to analyse the influence of the different angle between the long axis of core facial surfaces and the radicular section of the post over the fracture resistance in ETT.
Materials and Methods
The study protocol was approved (number SRC/REG/2016-2017/06) by the Institutional Ethical Committee, College of Dentistry, King Khalid University; it was conducted during the second academic semester of 2016. Thirty recently extracted maxillary canines were utilized in the study. The teeth samples included in the study were extracted for the periodontal reasons. Inclusion criteria for the teeth samples was absence of caries, microcracks and restorations. The samples were stored under the distilled water until the preparation for the study at the controlled temperature of 25±30°C. Based on an effect size of 1.4, a power of 80% and a significance level of 5% (p< 0.05), the sample size was determined to be 10 per group, resulting in a total of 30 specimens. The sample size was calculated with the G*Power software (version 3.1; University of Dusseldorf) [12].
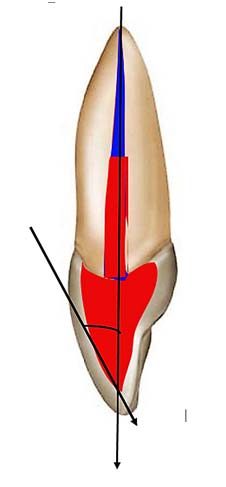
The exclusion criteria included the existence of caries, restorations, microcracks, cervical abrasion and dental anomalies like dens evaginatus, germination. The microcracks were evaluated by scrutinising teeth samples under ×3 microscope. The root surface of the teeth samples were covered by two layers of adhesive tape. Subsequently, they were mounted vertically within polymethyl methacrylate acrylic blocks with help of dental surveyors. About 2 mm of tooth structure above the cementum-enamel junction was maintained during implanting into the acrylic blocks. The adequate size access cavity was prepared and root canals were instrumented up to file no 5 with the Protaper file system (Dentsply Maillefer, Switzerland). The crown down technique was followed for the root canal shaping with intermittent irrigation with 3% sodium hypochlorite solution. The root canal obturation was accomplished with gutta-percha cold lateral condensation technique and AH plus sealer (Dentsply Maillefer, Switzerland). All teeth samples were de-coronated by preserving 2 mm of tooth structure above the cementum-enamel junction. The post space was created by utilising the progressively larger gates gladden, peso reamers up to the size of 4. The post space length preparation was kept uniformly for all the samples at 18 mm. Due care was observed to maintain the minimum of 5 mm gutta-percha as an apical seal. The access cavity undercuts were eliminated for easy removal of set wax pattern. The post space was gently irrigated with 3% sodium hypochlorite solution followed by normal saline. The custom-made post and core were fabricated with the direct technique [13]. The plastic impression post was initially tried in the canal to ensure its entry all the way up to the prepared space. The post space was lubricated with duralay lubricant and root canal was filled with pattern resin (Duralay, GC EUROPE NV Leuven, Belgium) using the bead-brush technique [13]. The plastic impression post was dipped in acrylic monomer and was seated in the root canal up to the full post space length. It was removed post setting with due care and inspected for voids. The excess plastic post top was sectioned by keeping the length of the core uniformly at the height of 6 mm. The core part was completed with duralay wax. The tooth/core preparation for the full veneer crown was completed using large-diameter coarse diamond bur with adequate water spray. The angle between the long axis of the post radicular segment and core facial surface long axis was standardized by using the protractor [Table/Fig-1]. The teeth samples were divided according to the angle between facial surfaces –long axis of the root into three groups of 10 each.
Picture depicting the angle between core facial surface–root long axis.
Group 1(n=10): Angle between the long axis of facial surface over the core - long axis of radicular segment was at 5°.
Group II (n=10): Angle between the long axis of facial surface over the core - long axis of radicular segment was at 10°.
Group III (n=10): Angle between the long axis of facial surface over the core - long axis of radicular segment was at 15°.
The completed post was immediately invested in phosphate bonded investment (GC Fujivest II GC EUROPE N.V.Leuven, Belgium). The casting was accomplished in conventional method using nickel-chrome alloy. The metal castings were divested, cleaned and cemented using glass ionomer luting cement (KetacCem, 3M ESPE, St. Paul, MN USA). The wax patterns for the full veneer crown were made directly over each tooth sample. The nickel-chromium metal coping were casted in conventional method. The metal coping were cleaned, polished and cemented over corresponding teeth samples using glass ionomer luting cement. The adhesive tape was removed from the root surface and the gained space within the acrylic block was relined using the light body additional silicone. The light body additional silicone relining helped in simulated the cushioning effect of periodontal ligament. The teeth samples were loaded at 3 mm from the incisal edge in palatal surface location and the angle of 1300° using universal testing machine (Instron Corporation, Massachusetts, United States) [Table/Fig-2]. The cross head speed of 0.5 mm/minute was employed for application of load. The static load was applied until the fracture of the teeth samples to record the maximum fracture resistance.
Testing samples for fracture strength under universal testing machine.

Statisyical Analysis
The obtained data was analysed with ANOVA and Tukey’s post-hoc test using SPSS 19 (IBM Corporation, Armonk, New York, USA) at the significance level p=0.05.
Results
The facial surface of core to post long axis angles evaluated during the study were 5° (Group-I), 10° (Group-II) and 15° (Group-III). The [Table/Fig-3] displays the mean average fracture strength values for three groups. The Group-III showed the highest fracture resistance with 666.151 N, followed by Group-II at 443.376 N. The lowest fracture strength was observed in the Group-I at 276.743 N. The increased angle between the long axis of facial surface and radicular segment of the post had a positive impact over the fracture resistance of the ETT.
Mean fracture resistance (Newton) among the groups.
| Groups | Mean | Std. deviation | 95% confidence interval for mean |
|---|
| Lower bound | Upper bound |
|---|
| Group I (50) | 276.7438 | 36.7989183 | 250.419440 | 303.068160 |
| Group II (100) | 443.3765 | 47.8791044 | 409.125852 | 477.627148 |
| Group III (150) | 666.1510 | 69.3557753 | 616.536867 | 715.765133 |
*The mean difference is significant at the 0.05 level.
The one-way ANOVA [Table/Fig-3] analysis indicated the presence of statistically significant difference in fracture strength between the groups with p<0.001. The Tukey multiple comparison tests [Table/Fig-4] was performed to evaluate the difference between the groups. The fracture strength of Group-I had the statistically significant difference in comparison to Group-II and Group-III with p-value<0.001. Similarly, Group-III had the statistically significant difference infracture strength from Group-II at p <0.05. Hence, it was inferred that all groups were significantly distinctive with each other groups with different angle.
Tukey Post-hoc multiple comparison test for mean fracture strength between the groups.
| Multiple comparisons |
|---|
| Fracture resistance | Mean Difference (I-J) | Std. Error | Sig. | 95% confidence interval |
|---|
| (I) Group | (J) Group | Lower Bound | Upper Bound |
|---|
| Group I (50) | Group II (100) | -170.3765000* | 24.6526650 | <0.001* | -231.635755 | -109.117245 |
| Group III (150) | -393.1510000* | 24.6526650 | <0.001* | -454.410255 | -331.891745 |
| Group II (100) | Group I (50) | 170.3765000* | 24.6526650 | <0.001* | 109.117245 | 231.635755 |
| Group III (150) | -222.7745000* | 23.9951421 | <0.001* | -282.399880 | -163.149120 |
| Group III (150) | Group I (50) | 393.1510000* | 24.6526650 | <0.001* | 331.891745 | 454.410255 |
| Group II (100) | 222.7745000* | 23.9951421 | <0.001* | 163.149120 | 282.399880 |
*. The mean difference is significant at the 0.05 level
Discussion
Several studies have revealed that ETT benefit from the placement of crowns [14]. The endodontic posts are primarily employed to retain the core in grossly destructed tooth. Ideal post core systems are expected to evenly distribute the functional force along the root surface. For better force distribution, the post should be as long as possible without endangering the apical seal [15]. The results from the previous researches indicate the presence of 2 mm ferrule significantly improves the fracture resistance of endodontically treated teeth [16].
The maxillary anterior teeth with two plane labial surface and variation in coronal- root curvature necessitates the fabrication of post with different angulation between coronal and radicular segment. To understand the effect of this difference in angulation between coronal and radicular segment of the post on the fracture resistance of the ETT, we fabricated the nickel-chromium custom posts with the facial surface- radicular segment angulations of 5°, 10° and 15°. Earlier research reports indicate the significant differences in the crown-root angles of maxillary central incisors among various malocclusions [17,18]. The collum angle is described to range from 5°-15° between different malocclusion groups. Hence the custom post with the crown-root angle of 5°, 10° and 15° were selected for evaluation in the study.
The results from the present study revealed that Group-III with facial surface- radicular segment long axis angulation 15° showed the highest fracture resistance of 666.151N in comparison to other two groups with lesser angle. According to the results from the study, the fracture resistance had positive linear correlation with the increased angle between facial angle- root long axes of the post.
The occlusal force direction has the great influence upon the stress distribution pattern of the intraradicular post. The masticatory force in the anterior region is inclined due to the vertical overlap of the incisors. The impact area in the anterior teeth is at the incisal 1/3rd of the tooth and at the average angle of 130° [19]. The oblique force on the maxillary anterior teeth during mastication results in rotational movement with the fulcrum at the cervical region of the dentin; the resultant stress is distributed on the external surface of the post [20]. The rotation movement also results in the compression on the buccal surface and tensile force on palatal surfaces [21]. The tensile strength of the dentin is considerably less than the compressive strength; hence, it predisposes the tooth for fracture [22,23].
Pegoretti A et al., suggested that horizontal loading is one of the major causes of failure for post-core restored ETT [24]. The vertical occlusal force due to shape of the tooth and micro movement permitted by periodontal ligament’s lead to line of force with the centre of rotation in apical third of the root [25,26]. Choy K et al., reported the morphological variations of the roots have a significant impact on the location of the centre of resistance [27]. The lateral force is expressed as torque; it is force multiplied by the perpendicular distance from the centre of rotation. It is expressed in the formula as T= F x D. D is the distance form centre of rotation; F is a resultant line of force [27,28]. The increased angle between coronal and radicular segments result in altering the occlusal impact area and reduces the perpendicular distance from the centre of rotation to the resultant force. Hence, effectively reduces the torque (lateral force) on the root. The torque generated from 130° force application is less in 15° angled post in comparison to the 10° and 5° angled post. As the torque was higher on the 5° angled post (Group-I), they exhibited lower fracture resistance. The metal endodontic posts with the high elastic modulus in comparison to dentin lead to the concentration of the forces on lingual surface of the post [29]. Therefore, few researchers suggest the use of intraradicular post with physical properties similar to the dentin to help in distribution of forces [30,31]. The present research result suggests the custom-made post similar in angulation with adjacent teeth is biomechanically more resistant for fracture. Further researches are needed to evaluate the effect of crown/radicular angulation in the post fabricated from different materials like zirconia, ceramic.
Limitation
The limitations for the study included the smaller sample size and it is difficult to replicate the intraoral conditions during in vitro studies. The force applied in study was the static-load until the fracture, while the masticatory force is cyclic loading nature.
Conclusion
Within the limitation of the study, following conclusions were drawn. The angle between the long axis of core facial surface and the radicular segment of the post has significant influence on the fracture resistance of the ETT. The post with the higher angle between the long axis of core facial surface to radicular segment possessed more fracture resistance than its counterpart with a smaller degree. The custom-made post similar in angulation to the natural adjacent teeth is beneficial both aesthetically and biomechanically for better force distribution.
*The mean difference is significant at the 0.05 level.
*. The mean difference is significant at the 0.05 level
[1]. Ingber FK, You are never fully dressed without a smileJ Esthet Restor Dent 2006 18(2):59-60. [Google Scholar]
[2]. Davis LG, Ashworth PD, Spriggs LS, Psychological effects of aesthetic dental treatmentJ Dent 1998 26(7):547-54. [Google Scholar]
[3]. Dong JK, Jin TH, Cho HW, Oh SC, The esthetics of the smile: a review of some recent studiesInt J Prosthodont 1999 12(1):09-19. [Google Scholar]
[4]. Hegde MN, Sajnani AR, Prevalence of permanent anterior tooth fracture due to trauma in South Indian populationEur J Gen Dent 2015 4:87-91. [Google Scholar]
[5]. Cheung W, A review of the management of endodontically treated teeth. Post, core and the final restorationJ Am Dent Assoc 2005 136(5):611-19. [Google Scholar]
[6]. Oliveira FdC, Denehy GE, Boyer DB, Fracture resistance of endodontically prepared teeth using various restorative materialsJADA 1987 115:57-60. [Google Scholar]
[7]. Spazzin AO, Galafassi D, de Meira-Junior AD, Braz R, Garbin CA, Influence of post and resin cement on stress distribution of maxillary central incisors restored with direct resin compositeOper Dent 2009 34(2):223-29. [Google Scholar]
[8]. Saunders WP, Saunders EM, Coronal leakage as a cause of failure in root-canal therapy: A reviewDent Traumatol 1994 10:105-08. [Google Scholar]
[9]. Harris EF, Hassankiadeh S, Harris JT, Maxillary incisor crown-root relationships in different angle malocclusionsAm J Orthod Dentofacial Orthop 1993 103:48-53. [Google Scholar]
[10]. Shen Y-W, Hsu J-T, Wang Y-H, Huang H-L, Fuh L-J, The collum angle of the maxillary central incisors in patients with different types of malocclusionJournal of Dental Sciences 2012 7(1):72-76. [Google Scholar]
[11]. Stanley J, Nelson in: Wheeler’s Dental Anatomy, Physiology and Occlusion 2013 10th edSt. LouisElsevier/Saunders:97-110. [Google Scholar]
[12]. Faul F, Erdfelder E, Buchner A, Lang AG, Statistical power analyses using G*Power 3.1: Tests for correlation and regression analysesBehavior Res Methods 2009 41:1149-60. [Google Scholar]
[13]. Rosenstiel SF, Land MF, Fujimoto J, Contemporary fixed prosthodontics 2016 5th edSt. Louis, MoMosby/Elsevier:130-35. [Google Scholar]
[14]. Baba NZ, Goodacre CJ, Daher T, Restoration of endodontically treated teeth: the seven keys to successGen Dent 2009 57(6):596-603.quiz 4-5, 595, 679 [Google Scholar]
[15]. Fernandes AS, Shetty S, Coutinho I, Factors determining post selection: a literature reviewJ Prosthet Dent 2003 90(6):556-62. [Google Scholar]
[16]. Ng CC, Dumbrigue HB, Al-Bayat MI, Griggs JA, Wakefield CW, Influence of remaining coronal tooth structure location on the fracture resistance of restored endodontically treated anterior teethJ Prosthet Dent 2006 95(4):290-96. [Google Scholar]
[17]. McIntyre GT, Millett DT, Crown-root shape of the permanent maxillary central incisorAngle Orthod 2003 73:710-15. [Google Scholar]
[18]. Williams A, Woodhouse C, The crown to root angle of maxillary central incisors in different incisal classesBr J Orthod 1983 10:159-61. [Google Scholar]
[19]. Dawson PE, Functional occlusion: from TMJ to smile design 2007 St. Louis, MoMosby/Elsevier:370-71. [Google Scholar]
[20]. Meira JB, Espósito CO, Quitero MFZ, Poiate IA, Pfeifer CS, Tanaka CB, Elastic modulus of posts and the risk of root fractureDent Traumatol 2009 25:394-98. [Google Scholar]
[21]. Toksavul S, Toman M, Uyulgan B, Schmage P, Nergiz I, Effect of luting agents and reconstruction techniques on the fracture resistance of prefabricated post systemsJ Oral Rehabil 2005 32:433-40. [Google Scholar]
[22]. Bowen RE, Rodriguez MS, Tensile strength and modulus of elasticity of tooth structure and several restorative materialsJ Am Dent Assoc 1962 64:378-87. [Google Scholar]
[23]. Kinney JH, Marshall SJ, Marshall GW, The mechanical properties of human dentinA critical review and re- evaluation of the dental literature. Crit Rev oral Bio Med 2003 14:13-29. [Google Scholar]
[24]. Pegoretti A, Fambri L, Zappini G, Bianchetti M, Finite element analysis of a glass fibre reinforced composite endodontic postBiomaterials 2002 23:2667-82. [Google Scholar]
[25]. Weinberg LA, Force distribution in splinted posterior teethOral Surg Oral Med Oral Pathol 1957 10:1268-76. [Google Scholar]
[26]. Weinberg LA, Force distribution in splinted anterior teethOral Surg Oral Med Oral Pathol 1957 10(5):484-94. [Google Scholar]
[27]. Choy K, Pae EK, Park Y, Kim KH, Burstone CJ, Effect of root and bone morphology on the stress distribution in the periodontal ligamentAm J Orthod Dentofacial Orthop 2000 117:98-105. [Google Scholar]
[28]. Weinberg LA, The biomechanics of force distribution in implant-supported prosthesesInt J Oral Maxillofac Implants 1993 8(1):19-31. [Google Scholar]
[29]. Barjau-Escribano A, Sancho-Bru JL, Forner-Navarro L, Rodríguez-Cervantes PJ, Pérez-Gónzález A, Sánchez-Marín FT, Influence of prefabricated post material on restored teeth: fracture strength and stress distributionOper Dent 2006 31(1):47-54. [Google Scholar]
[30]. Watanabe MU, Anchieta RB, Rocha EP, Kina S, de Almeida EO, Freitas AC Junior, Influence of crown ferrule heights and dowel material selection on the mechanical behavior of root-filled teeth: a finite element analysisJ Prosthond 2012 21(4):304-11. [Google Scholar]
[31]. Akkayan B, Gulmez T, Resistance to fracture of endodontically treated teeth restored with different post systemsJ Prosthet Dent 2002 87(4):431-37. [Google Scholar]