Neglected Type I Monteggia Fracture Dislocation in Adult
Archit Agarwal1, Inder Pawar2
1 Senior Resident, Department of Orthopaedics, ESIC PGIMER, Basaidarapur, New Delhi, India.
2 Professor, Department of Orthopaedics, ESIC PGIMER, Basaidarapur, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Archit Agarwal, 89 Ram Vihar Near ONGC Hospital, Dehradun-248003, Uttrakhand, India. E-mail : dr.architagarwal@gmail.com
Neglected Monteggia fracture dislocation is one of the challenging case and it becomes more of a therapeutic dilemma especially in adults. Several surgical techniques are described and in spite of this complication rate following surgery is high. This report concerns with management of three-month-old monteggia fracture dislocation in a 30-year-old male. Patient presented with complete loss of movement at elbow. Patient was managed surgically, with internal fixation of ulna and reduction of radial head with radio-capitellar Kirschner wires. Postoperatively at six months, ulna united and patient has achieved flexion from 50 to 115 degrees at elbow and supination pronation arc of 120 degrees. We do not see any indication for procedures directed at the reconstruction of annular ligament. The dilemma remains whether radial head preservation or excision gives better functional range of motion in adult neglected monteggia fracture dislocation.
Elbow trauma, Neglected, Radial head dislocation, Ulna fracture
A 30-year-old male presented to the outpatient clinic with pain and complete loss of movement at elbow since last three months. He gave history of fall three months back for which he took treatment from a quack. Clinically, there was bony deformity on the medial side of forearm. Patient held the elbow in 90 degree flexed and neutral position.
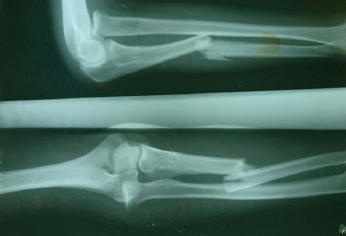
Radial head was palpable anteriorly and no supination pronation was present. There was no flexion and extension at elbow. There was no neurovascular defect. On skiagrams [Table/Fig-1], there was diaphyseal fracture of ulna with anterior angulation and radial head was dislocated anteriorly. Thus, it was labelled as Bado type I monteggia fracture dislocation.
Preoperative x-rays showing Bado type I monteggia fracture dislocation.
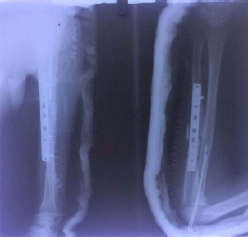
Surgery was planned. Open reduction and internal fixation of ulna was done with 9 hole LC-DCP (Limited Contact- Dynamic Compression Plate) and autologous bone grafting. Radial head did not reduce even after fixation of ulna so by using a different incision (Kocher’s approach) it was exposed. The radial head was not deformed and thick scar tissue filled the radiocapitellar space. After excision of scar tissue the radial head reduced. After reduction, on extension radial head was subluxating so two radio-capitellar Kirschner wires were placed to maintain the radial head reduction. Above elbow slab was given with forearm in 90 degree flexion and full supination [Table/Fig-2].
Postoperative x-rays showing radiocapitellar K wires and fixation of ulna.
At six weeks, Kirschner wires and slab was removed. Patient was followed up then at 3rd and 6th. Postoperatively at six months [Table/Fig-3], ulna united and patient has achieved flexion from 50 to 115 degrees at elbow and a 120 degrees supination pronation arc [Table/Fig-4,5,6]. At each visit check x-ray was done to see for bony union and radiocapitellar congruency. DASH score (Disabilities of Arm, Shoulder and Hand), Broberg-Morrey index score and range of movement were recorded at each visit to see the functional improvement [Table/Fig-7].
Ulna union and reduced radial head at six months..

Flexion-extension at elbow at six months.

Supination at six months.


Range of movement and functional scores at different visits postoperatively.
| Parameter | 6 weeks Post Op | 12 weeks post op | 24 weeks post op |
|---|
| Flexion at elbow | 60 to 70 degrees | 60 to 110 degrees | 55 to 115 degrees |
| Supination pronation arc. | 30 degrees | 90 degrees | 120 degrees |
| DASH score | 68.3 | 45.8 | 25 |
| Broberg-Morrey index | 24 | 57 | 74.5 |
Regular active and passive physiotherapy were done. Continuous Passive Motion (CPM) machines were used during first three months of rehabilitation. Paraffin wax bath along with joint mobilization techniques improved the range of motion at elbow joint. The stiffness was mostly due to soft tissue involvement so ‘Hold-relax’ exercises and ‘Contract-relax exercises were used. Static and dynamic splints were not used as loss of range of motion was mostly due to articular involvement. Such splints are effective when there is predominantly soft tissue involvement. Patient compliance is also a problem with such splints as they lead to continuous pain due to muscle spasms. No invasive intervention was done to increase the range of motion. Manipulation under anaesthesia was not tried keeping in view the complication of iatrogenic fracture post manipulation. Consent from patient was taken for publication of x-rays and his pictures.
Discussion
Fracture of proximal ulna with anterior dislocation of radial head was described by Monteggia GB in 1814 [1]. Later in 1909 Perin J described this fracture pattern as monteggia fracture dislocation[2]. Later Bado JL classified it further into four types according to angulation of the ulna fracture and direction of the radial head dislocation. In adults, type II is more common (80%) [3] [bado]. Type 1 lesions are more common in children [1]. Monteggia fracture dislocations represent approximately less than 5% of forearm fractures [4]. Several reports of chronic monteggia lesions in children have been published [5,6]. These were the ones in which pattern of injury was not recognised or were undertreated. In this article we describe our experience of managing neglected monteggia fracture dislocation in an adult.
Very few reports of chronic monteggia in adults have been published [7,8] and they have described different management options. In a study of four cases of chronic monteggia in adults, Boyd’s approach was used to salvage the radial head and fix the ulna with a plate. They used first distal screw in distraction mode in order to lengthen the ulna. In our case, we used a different approach to expose the radial head and transfixed it to capitellum with K wires. Ulna was not lengthened and plate was applied in compression mode [7]. Treatment of chronic radial head dislocation is still controversial. Several techniques like ligament reconstruction and ulnar osteotomy have been proposed for management for chronic monteggia lesions. In cases of complex monteggia fracture dislocations, careful reconstruction of the proximal ulna including the olecranon and coronoid may be required [4]. Ulna length has been considered as one of the very important factor which would affect the functional outcome eventually. This is so because radius and ulna act as one unit while supination and pronation. Therefore, ulnar osteotomy plays an important role in management of monteggia fracture dislocation [5]. In vivo three dimensional kinematics of radial head dislocation in type I and IV monteggia fracture dislocation has been studied. According to them in type I lesions radial head was relatively stable due to isometricity of the interosseous membrane. This supported the concept of maintaining the ulnar length by ulnar bending osteotomy [9]. Annular ligament reconstruction has continued to be another topic of debate in management of chronic lesions. In a comparative study between the ones managed with annular ligament reconstruction and others without, it was concluded that it is not always necessary [6]. Ligament reconstruction has been advised when there is considerable coronal translation of the radial head [5]. In our case, there was anterior dislocation and after reduction and fixation of ulna intraoperatively there was no coronal translation of the head.
Usually after reduction and fixation of ulna, radial head gets reduced but at times when the radial head does not get reduced, buttonholing through the annular ligament or anconeus muscle should be suspected. In such cases, a separate radial approach is advisable. A combined approach to proximal ulna and radius has higher risk of radioulnar synostosis [4]. Neglected cases of montaggia fracture dislocation have been reported to be associated with posterior interosseous nerve palsy. But this mostly recovers after anatomical reduction of radial head as mostly it is a neuropraxia injury [10]. Radiocapitellar fixation with temporary K wire is not advocated by some because of risk of pin migration and damage to articular cartilage [11]. The present case did not have such complication.
DASH score helps to describe the disability experienced by people with upper-limb disorders and also to monitor changes in symptoms and function over time. A higher score indicates greater disability [12]. In a study, 17 cases of type II monteggia fracture dislocation had a mean standardised DASH score of 23 (0 to 70) and the mean Broberg- Morrey functional index score of 83 (32.5 to 100) after follow-up, at 29 months [13]. In our case, at six months the DASH score is 25 and Broberg-Morrey score 74.5. It is expected to see improvement in functional ability of patient with time. In a cadaveric study, it has been found that after radial head excision tension in the interosseous membrane almost doubled [14]. Also, it has been advocated to excise the radial head only in those monteggia lesions where there was radial head fracture [8]. In present case, the radial head was not excised. Postoperatively, patient has not managed to regain complete range of motion, even though his DASH score and Broberg-Morrey score have shown constant improvement. To find out if radial head excision at the time of ulna fixation would have given better functional results in a neglected case, further research has to be done. However, the rarity of such neglected cases in present day scenario makes it difficult to do a comparative study between two (radial head excised/ not excised) larger groups of patients.
Conclusion
In adults where no growth/remodelling potential is left, procedures like fixation of ulna in angulation, ulna lengthening is not required. There appears to be an indication for procedures directed at the reconstruction of annular ligament. The dilemma remains whether radial head preservation or excision gives better functional range of motion in adult neglected monteggia fracture dislocation.
[1]. Monteggia GB, Monteggia GB, Lussazioni delle ossa delle estremita superioriInstituzioni Chirurgiches 1814 52ndMilan, ItalyMaspero:131-133. [Google Scholar]
[2]. Perrin J, Perrin J, Les fractures du cubitus accompagnees de luxation de l’extremite superieur du radiusThese de Paris 1909 G SteinheilParis, France [Google Scholar]
[3]. Bado JL, The Monteggia lesionClin Orthop Relat Res 1967 50:71-86. [Google Scholar]
[4]. Streubel PN, Pesantez RF, Court-Brown CM, Heckman JD, McQueen MM, Ricci WM, Tornetta P, IIIMcKee M, Diaphyseal fractures of the radius and ulna. Rockwood and Green’s Fractures in Adults 2014 18th edPhiladelphia, PAWolters Kluwer Health/Lippincott Williams & Wilkins:1139-67. [Google Scholar]
[5]. Goyal T, Arora SS, Banerjee S, Kandwal P, Neglected Monteggia fracture dislocations in children: a systematic reviewJournal of Pediatric Orthopaedics B 2015 24(3):191-99. [Google Scholar]
[6]. Bhaskar A, Missed Monteggia fracture in children: Is annular ligament reconstruction always required?Indian Journal Of Orthopaedics 2009 43(4):389 [Google Scholar]
[7]. Jepegnanam TS, Salvage of the radial head in chronic adult Monteggia fractures. Report of four casesJ Bone Joint Surg Br 2006 88(5):645-48. [Google Scholar]
[8]. Ring D, Jupiter JB, Simpson NS, Monteggia fractures in adultsJ Bone Joint Surg Am 1998 80(12):1733-44. [Google Scholar]
[9]. Miyake J, Moritomo H, Kataoka T, Murase T, Sugamoto K, In vivo three-dimensional motion analysis of chronic radial head dislocationsClinical Orthopaedics and Related Research® 2012 470(10):2746-55. [Google Scholar]
[10]. Ristic S, Strauch RJ, Rosenwasser MP, The assessment and treatment of nerve dysfunction after trauma around the elbowClinical Orthopaedics And Related Research 2000 370:138-53. [Google Scholar]
[11]. Datta T, Chatterjee ND, Pal AK, Das SK, Evaluation of outcome of corrective ulnar osteotomy with bone grafting and annular ligament reconstruction in neglected Monteggia fracture dislocation in childrenJ Clin Diagn Res: JCDR 2014 8(6):LC01 [Google Scholar]
[12]. Jester A, Harth A, Wind G, Germann G, Sauerbier M, Disabilities Of The Arm, Shoulder and Hand (DASH) questionnaire: determining functional activity profiles in patients with upper extremity disordersJ Hand Surg 2005 30B:23-28. [Google Scholar]
[13]. Strauss EJ, Tejwani NC, Preston CF, Egol KA, The posterior Monteggia lesion with associated ulnohumeral instabilityBone & Joint Journal 2006 88(1):84-89. [Google Scholar]
[14]. Lanting BA, Ferreira LM, Johnson JA, Athwal GS, King GJ, The effect of excision of the radial head and metallic radial head replacement on the tension in the interosseous membraneBone Joint J 2013 95(10):1383-87. [Google Scholar]