Materials and Methods
A screening mammography camp was organized for one week in February 2017 for women aged over 40 years in a tertiary care hospital of Karnataka, India. The event was organized in an effort to increase awareness about breast cancer and its screening among general population. The conduct of the camp was brought to public attention by means of word of mouth and circulation of booklets through health workers. This was done in an effort to encourage women to voluntarily seek medical attention for their problems related to breast if any and also to undergo free mammography in the institute.
A prospective observational study was undertaken with prior Institutional ethical committee clearance. A total of 118 females volunteered to undergo mammography during the duration of this study. Sample size was found adequate as per power based sample size calculation formula. Before subjecting them to mammography, a detailed clinical examination coupled with relevant history taking was done which included breast related symptoms if any, intake of any medications, pregnancy, family history of breast cancer etc. Pregnancy is a contraindication for mammography and hence pregnant females were excluded from the study.
All the females were explained about the procedure and safety of mammography in the light of X-rays used in the procedure.
After taking written informed consent from all the females, an Allengers digital mammography machine was used to carry out bilateral mammography with application of appropriate compression forces. Cranio-caudal and a medio-lateral oblique views were taken for both breasts in all women using the mode of Automatic Exposure Control (AEC). The mammograms were viewed in the console by a Radiologist with five years experience in breast imaging and reported as per ACR-BIRADS 5th edition 2013 specifications [12]. The detailed specifications of ACR-BIRADS are beyond the scope of this study and only relevant points have been highlighted here. Initially breasts were classified based on composition, i.e., near complete fatty breasts [Table/Fig-1] or scattered fibroglandular densities [Table/Fig-2] or heterogeneously dense (if such densities are likely to obscure underlying lesions as in [Table/Fig-3] or extremely dense. Further any mass, asymmetry, architectural distortion, calcifications and ancillary findings were described using terminologies suggested in 5th edition of ACR BIRADS [12]. Wherever heterogeneously dense or extremely dense breasts were found, complimentary sono-mammography was done and a final assessment category of BIRADS was determined and management recommendations were given.
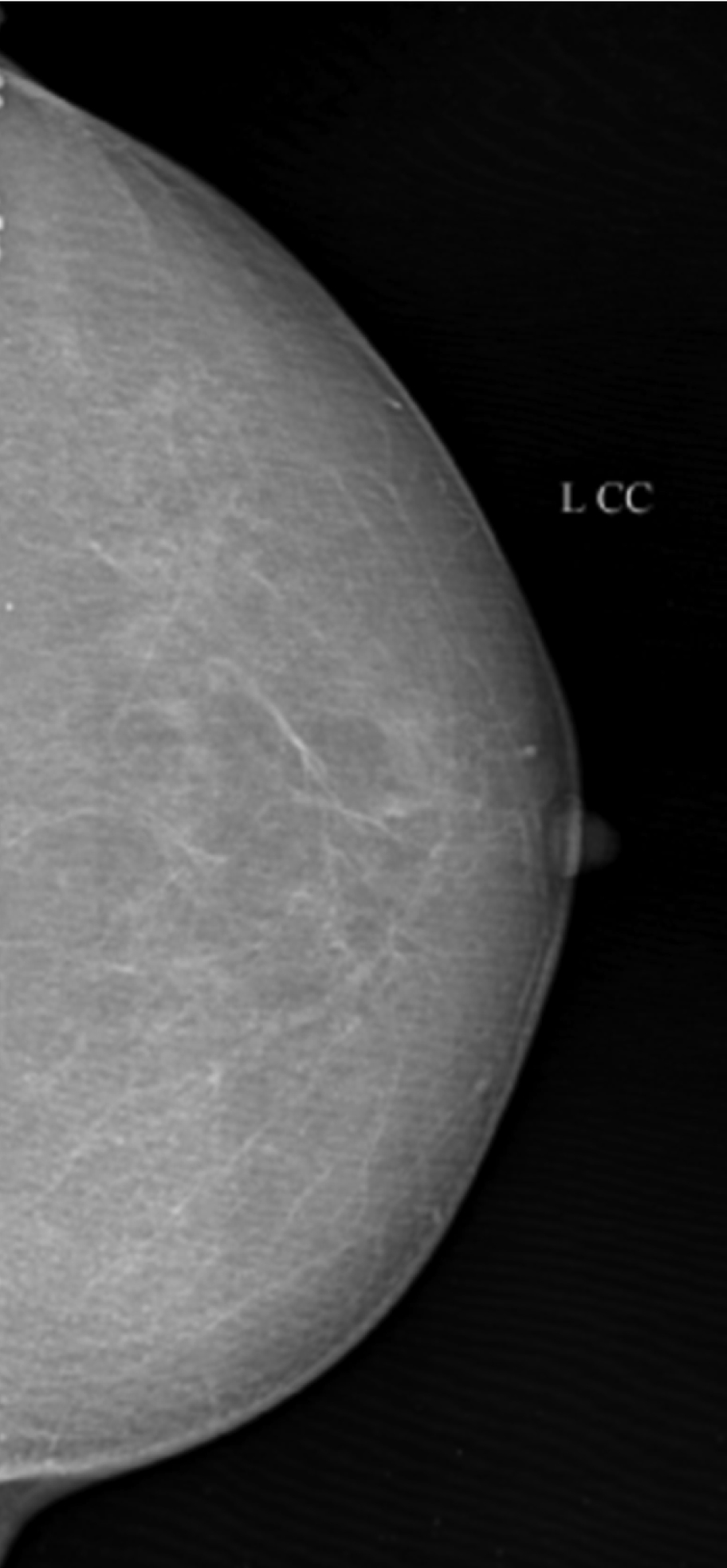
Cranio-caudal view of left breast, composed of almost entirely fatty densities. The final assessment category was ACR-BIRADS 1.
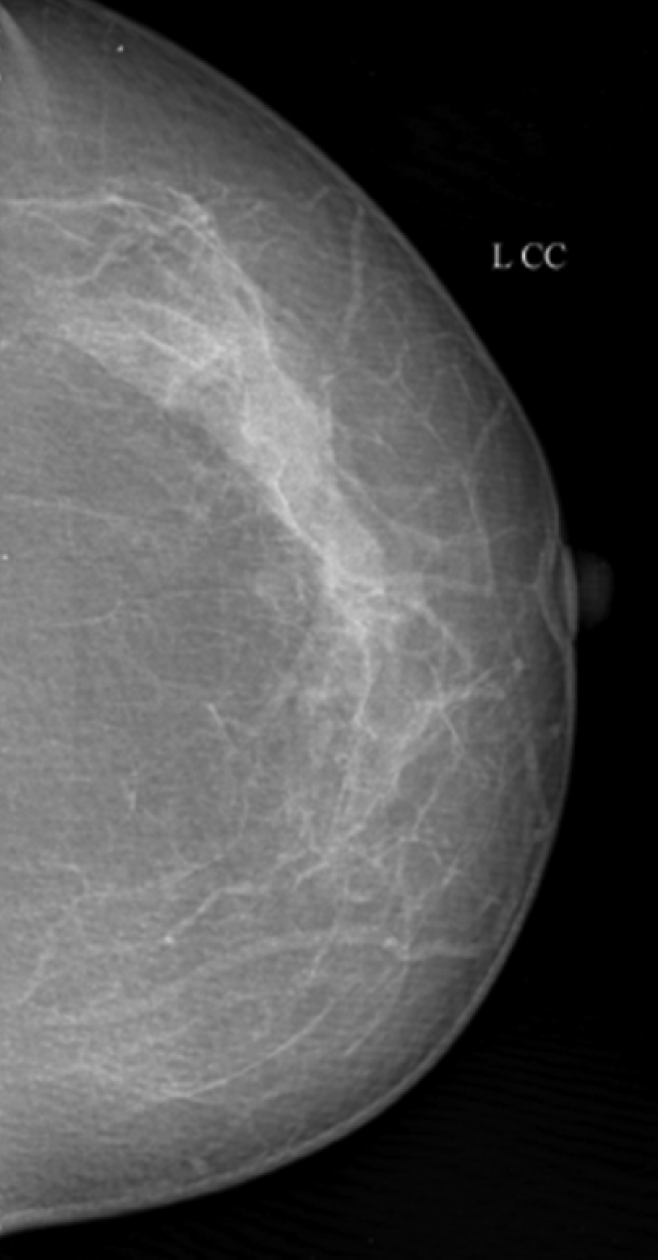
Cranio-caudal view of left breast, composed of scattered fibroglandular densities. The final assessment category was ACR-BIRADS 1.
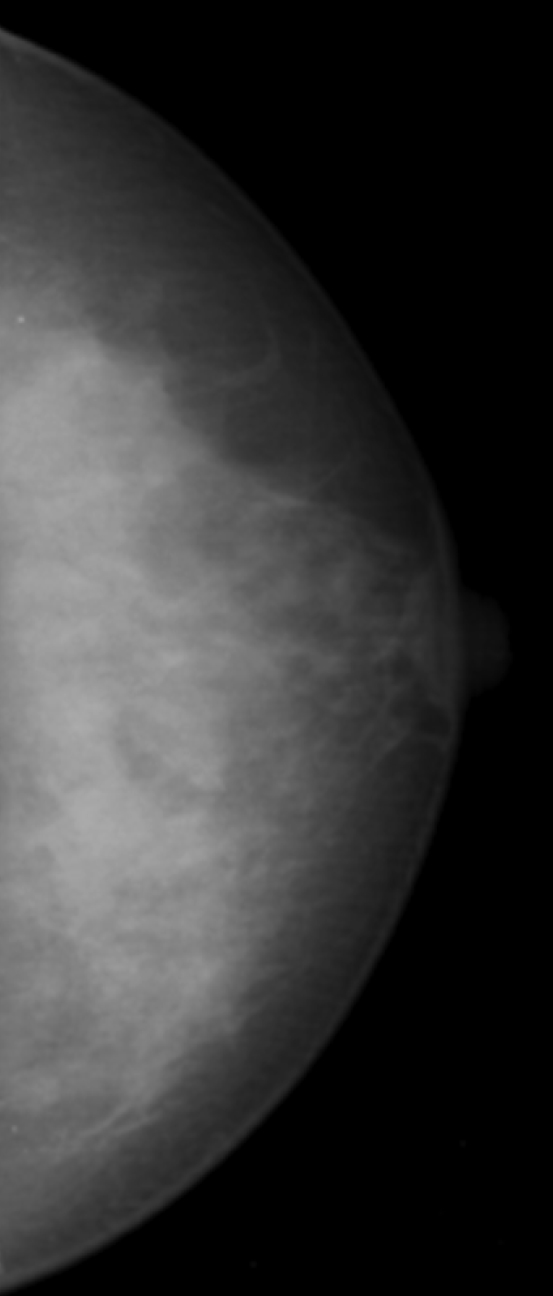
Cranio-caudal view of left breast, composed of heterogeneous densities.
Complimetary sonomammography was performed by the same Radiologist in the same institute using a GE Logiq S6 machine. After explaining the procedure of scanning, the patient was made to lie down supine with adequate exposure. The ipsilateral shoulder was slightly elevated to flatten the breast by placing a pillow underneath the shoulder. A 7.5 -12 Mega Hertz (MHz) linear probes was used to scan the breast radially in clockwise direction. The axillary region was also scanned for any lymph nodes.
Normal mammographs/sonomammographs were considered as BIRADS 1 category [Table/Fig-1,2]. Benign lesions like fat necrosis, intramammary lymph node, involuting fibroadenoma, simple cyst, large calcifications and vascular calcifications [Table/Fig-4] were labeled as BIRADS 2. Non palpable circumscribed masses on mammography (other than benign lesions described above), focal asymmetry, solitary cluster of microcalcifications (five or more calcifications in 2 square cm area), typical fibroadenoma/clustered microcysts /isolated complex cyst on ultrasonography were given a category of BIRADS 3 and advised follow up at six months as per ACR-BIRADS recommendation. Fine linear branching/ pleomorphic /amorphous/coarse heterogeneous calcifications, atypical fibroadenomas, indistinct margins of a mass, complex solid/ cystic mass were recorded as BIRADS 4 and advised to undergo biopsy. Masses with spiculated irregular margins with or without pleomorphic calcifications/ fine linear segmental calcifications were considered as highly suggestive of malignancy or BIRADS 5 and biopsy was performed [Table/Fig-5] [12].
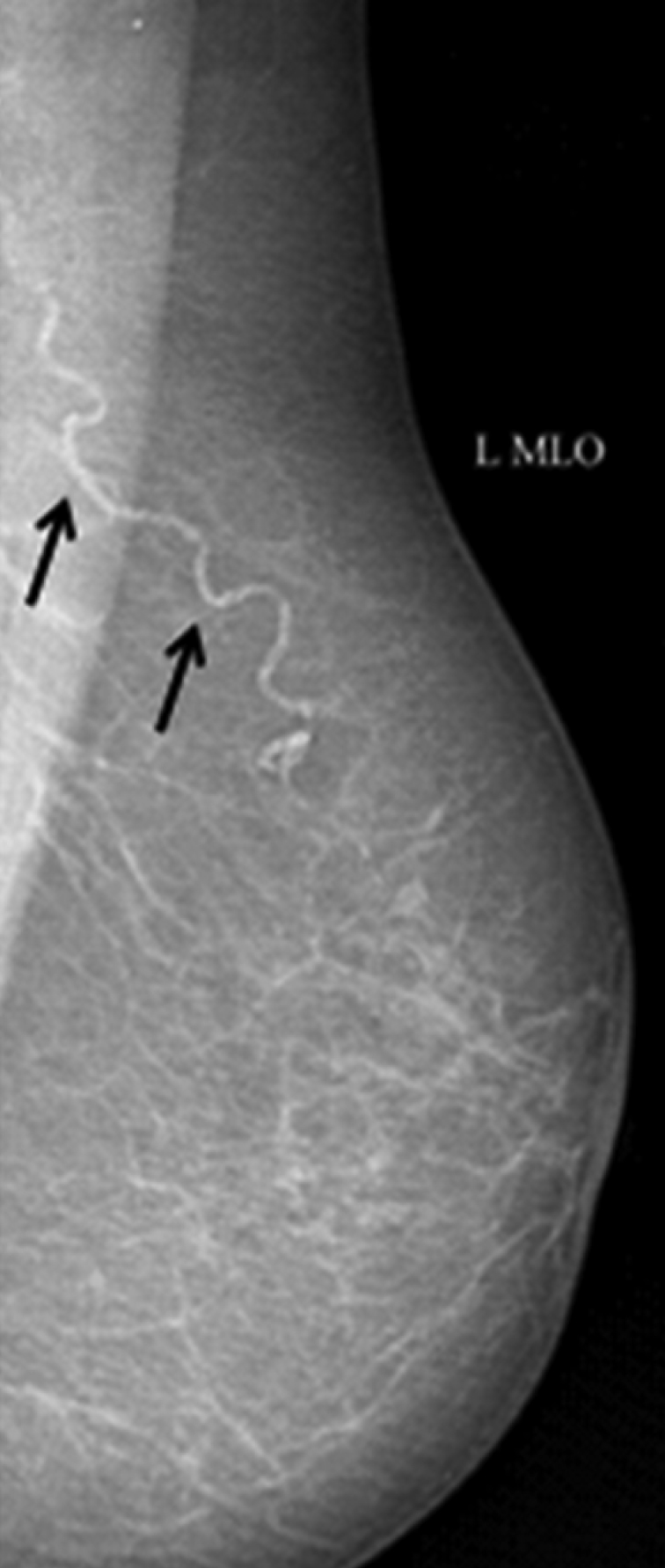
Medio-lateral oblique view of left breast showing vascular calcification (black arrows). A final assessment category of ACR-BIRADS 2 (benign finding) was given.
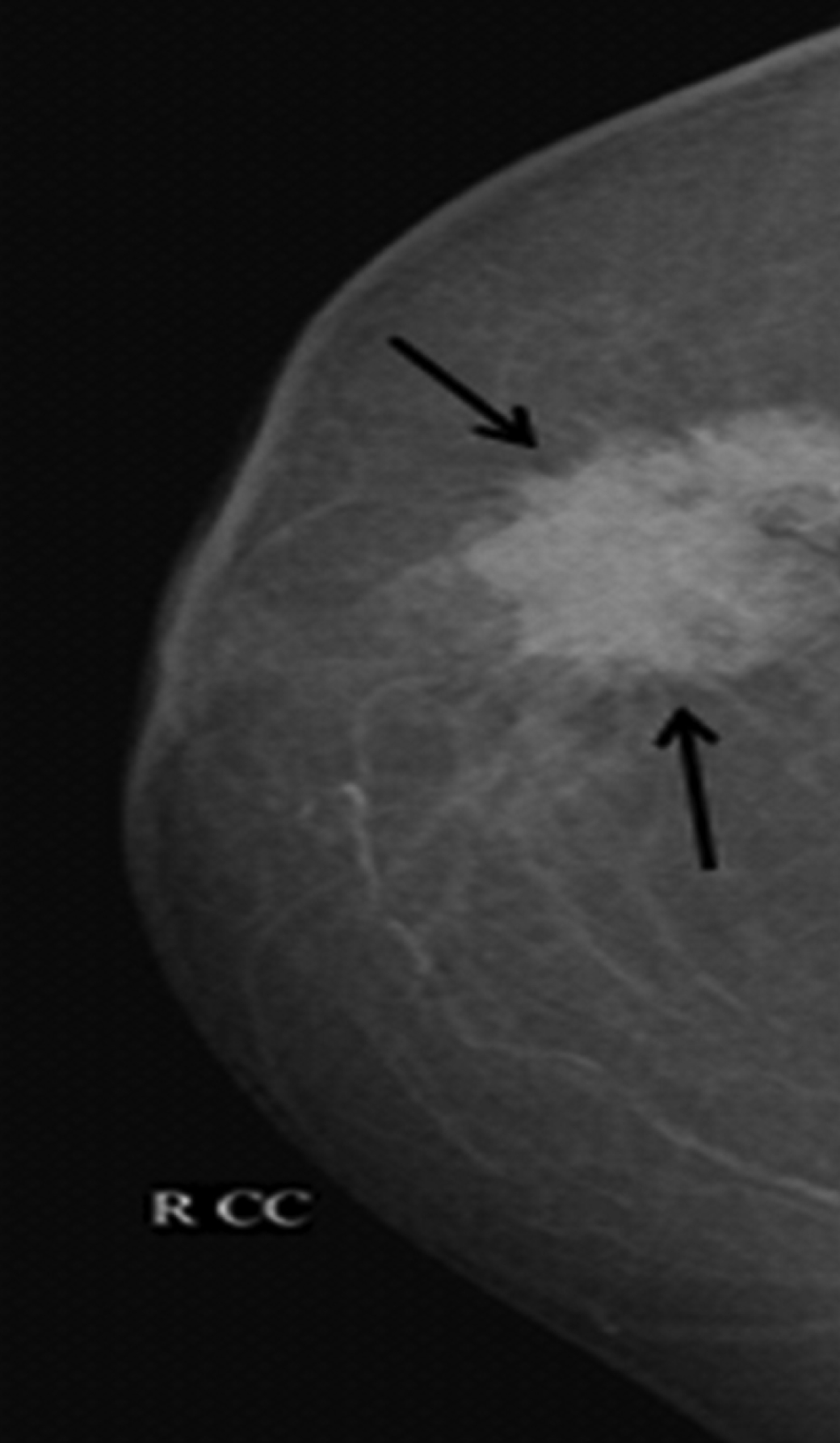
Cranio-caudal view of right breast. A mass lesion with spiculated margins (black arrows) is seen in the lateral quadrant of right breast. This lesion was assessed as ACR-BIRADS 5. Biopsy obtained from the mass revealed ductal carcinoma.
Statistical Analysis
The data was tabulated in Microsoft Excel spreadsheet. Number of women volunteering for mammography, new breast malignancies detected during the duration of camp/study was compared with past statistics of the same institute, to identify the benefits of mammography.
Results
The study included 118 women who ranged from 35 to 64 years of age with a mean age of 49.6 years. Ninety eight of such ladies had no breast related symptoms and had volunteered for mammography, knowing about the screening camp organized for breast cancer in our institution. Four of them, though themselves asymptomatic, gave family history of breast cancer in their 1st degree blood relatives. Though these four ladies were aged under 40 years, they were included in the study as screening mammography should be started 10 years prior to the age of detection in the relative, as per recommendations of ACR-BIRADS. One of these ladies also complained of multiple bilateral breast lumps. The other three ladies were asymptomatic. Of the remaining 20 ladies, seven ladies presented with lump in the breasts noticed six months to one year prior, three of whom had intermittent bloody nipple discharge. The other 13 ladies complained of vague mastalgia. All these 20 ladies were hesitant to seek medical attention till they were coaxed by health workers to visit the institute for mammography camp. They also claimed that they would not have sought medical care in immediate future, if not for the camp.
Seventy three ladies were found to have scattered fibroglandular densities on mammography and another 15 almost entirely fatty composition as depicted in [Table/Fig-6]. The rest 30 ladies with heterogenous and extreme dense breast composition were further evaluated with sono-mammography to look for any pathologies, as such densities are likely to obscure any subtle lesions. Of them, 10 ladies were given a final ACR-BIRADS assessment category of BIRADS 1, nine ladies were given an assessment category of BIRADS 2, nine cases showed lesions requiring frequent follow up and were given BIRADS 3 and two cases of heterogeneously dense breasts were found to have suspicious lesions on ultrasonography and were categorized as BIRADS 4 and were advised biopsy, which revealed malignancies.
Breast composition on mammography.
| Breast composition | Number of ladies |
|---|
| Almost entirely fatty | 15 |
| Scattered fibroglandular densities | 73 |
| Heterogeneous densities | 24 |
| Extremely dense | 06 |
Of the eight cases with categories BIRADS 4 and 5, seven cases underwent biopsy in the institution and six of them were confirmed to have malignancies. One other female was referred to another centre for stereotactic mammography guided biopsy, as facilities for same were not available in our institution. The number of females with their final ACR-BIRADS assessment categories is depicted as per [Table/Fig-7].
ACR-BIRADS assessment categories.
| ACR-BIRADS* final assessment categories | Number of ladies |
|---|
| BIRADS 1 | 36 |
| BIRADS 2 | 46 |
| BIRADS 3 | 28 |
| BIRADS 4 | 7 |
| BIRADS 5 | 1 |
ACR-BIRADS - American College of Radiology - Breast Imaging Reporting and Data Systems
In all, 118 females were evaluated with bilateral mammography of which 6 (5.1%) new cases of breast carcinoma were detected during this study and another 28 (23.7%) cases with probably benign findings were advised short interval follow up.
Discussion
The lurking danger in India, in terms of cancer related mortality among women, is the enormity of the magnitude of the undiagnosed/hidden cases [6]. This can be attributed to the conservative nature of the society, hesitancy among women to seek medical help, customs, illiteracy, ignorance and non availability of nationwide screening program [3,4,6,11]. There has been a sharp increase in the incidence rates of breast cancer in India with every passing year [2].
The week long screening camp conducted as part of this study was able to attract significantly more females (118) than the number of cases of mammography in our institute in previous six months (98). This signifies the effective role of reaching out to public by means of word of mouth, health care workers, handouts etc., in an effort to dispense the ignorance, hesitancy and taboo associated with such medical conditions. Most of the females were unlikely to undergo mammography and clinical breast examination, if not for the awareness created by the camp.
Cancer screening camps have been earlier used as part of studies in India to assess the utility of screening mammography and its effectiveness. Reddy N et al., organized a screening camp comprising of clinical breast examination, mammography, ultrasonography and fine needle aspiration biopsies of suspicious lesions in a rural area and found that mammography was not feasible in Indian set up due to financial considerations and suggested that the procedure may be limited to high risk ladies only [10]. The study recommended that regular self breast examination, clinical breast examination, education and awareness are more viable alternatives to mammography for screening purposes in India. This is in contradiction to some studies, which suggested that mammography is the only screening modality proven to effectively reduce mortality [7,8,13]. In the present study, six new cases of breast cancer were detected and confirmed on histopathology as against no positive cases diagnosed in the study by Reddy N et al., [10]. The data on mammography in our institute suggests most of the cases were referred from different specialities rather than voluntary and seven new cases of breast cancer were detected among them. However, such referred patients do not represent the general population in contrast to the present study.
There is no conclusive evidence to show that by only increasing awareness and self breast examination, mortality rates can be effectively reduced [7,9]. Barton MB et al., found that clinical breast examination along with mammography, as screening tools, have a role in reducing mortality. However, there is no evidence of clinical breast examination as an independent screening tool contributing to reducing mortality. Moreover, the clinical examination methods have not been standardized [14].
Mammography is most sensitive in detecting lesions in breasts composed of scattered fibroglandular densities or entirely fatty breasts. When the breast parenchymal composition is dense, the sensitivity of film screen mammography decreases [15]. Such dense breasts are also associated with increased risk of developing breast cancer [16]. With digital mammography, the sensitivity of detecting lesions even in dense breasts has improved [17]. MRI and ultrasonography have a supplemental role in the screening protocol and cannot replace mammography as a primary screening modality [18].
Bleyer A and Welch HG, concluded that though the overall reduction in mortality by the use of mammography as screening tool is marginal, there was a significant risk of overdiagnosing and over treating owing to the early detection of lesions, the treatment of which may not yield any benefits in terms of mortality reduction [19]. However, in a country like India, where many cases are detected in late stages leading to increased mortality rates [5], such a tool can only improve survival.
Many states of USA have legislations regarding implementation of mammography as screening tool with suitable modifications from time to time [20]. In the Indian scenario, there is an argument that effective breast cancer screening program involving mammography will not be feasible due to financial implications [5,10,21]. However, in the present context, when India is the fastest growing economy and when the gender sensitivity and equality is being highlighted like never before by the administration, time cannot be more appropriate to come up with a suitable breast cancer screening program incorporating mammography camps, clinical breast examination and awareness campaigns and pay a tribute to the women of this nation. It is not fair on our part to conclude that our economy will not be able to handle the financial burden. Its an administrative call. A sensitive government will find it important enough to channelize finances and expand the mammography services and integrate clinical breast examination and community driven mass awareness campaigns, so that the taboo, stigma, hesitancy on part of our society can be overcome and maximum females can reap the benefits of early detection of breast cancer.
Limitation
The participants in the camp were from a specified geographical area (district). Multiple such studies in different parts of the country can further strengthen the findings. The change in the participant’s knowledge and behaviour as a result of the camp was not assessed. The camp was conducted for free and hence the likely financial burden due to implementation of the mammography camp was not calculated.
Conclusion
There is a need for breast cancer screening program, due to a sharp increase in incidence and associated mortality among Indian females. Mammography, being the only proven modality to effectively reduce mortality due to breast cancer, is the need of the hour in India, despite its financial implications. Screening mammography camps help reach out to public, increase awareness, help mobilize women to seek medical care and also identify malignancy at an earlier stage. It is the right time, when India is amongst fastest growing economies and when gender sensitivity is a major administrative priority, to formulate a suitable breast cancer screening program incorporating mammography camps, clinical breast examination and awareness campaigns and pay a tribute to the women of this nation.
*ACR-BIRADS - American College of Radiology - Breast Imaging Reporting and Data Systems