The International Osteoporosis Foundation has estimated that worldwide, approximately 30%-50% people aged over 50 years are at risk for the development of fragility fractures secondary to osteoporosis [1]. Vertebral compression fractures occur in 20% of people over the age of seventy years and in 16% of postmenopausal women. Osteoporotic vertebral compression fractures are commonest in the dorso-lumbar region [2]. Prevention of progressive kyphotic deformity or correction of existing deformity is important both to reduce the risk of fracture at adjacent levels and to prevent the consequences of spinal kyphosis [3-5].
Osteoporotic vertebral compression fractures have been shown to adversely affect quality of life, physical function, mental health, and survival. These effects are related to the severity of the spinal deformity and pain associated with the fracture. In recent years, researchers have highlighted the impaired pulmonary function that is associated with osteoporotic vertebral compression fractures and spinal deformity [6]. It has been reported that, there is 9% decrease in pulmonary vital capacity for each thoracic vertebral fracture [7]. Kyphosis can lead to reduced abdominal space with poor appetite and resultant nutritional problems [8]. By shifting the patient’s centre of gravity forward, kyphotic deformity not only increases the risk of additional fractures, but also may lead to poor balance, which increases the risk of accidental falls [5]. In addition to the morbidity associated with vertebral compression fractures, there is an increased mortality rate for older women with vertebral compression fractures compared with that for age matched controls, as found in a prospective study. The mortality rate was related to pulmonary problems, and it increased with the number of vertebrae fractured [9].
Traditionally, acute vertebral compression fractures have been treated non-operatively except in rare cases in which the fracture is associated with neurologic compromise or advanced spinal instability. Non-operative measures for some symptomatic vertebral compression fractures fail as a result of intolerable pain, deformity, loss of function, or a combination thereof [10]. Open spinal surgery in patients with osteoporosis is fraught with complications because these patients are often of advanced age and frequently have co morbidities and because of the difficulty of securing fixation in osteoporotic bone [11]. So, vertebral compression fractures should be aggressively treated with minimally invasive techniques such as PVP or PKP, other than traditional methods such as conservative treatment or open surgery. The present study was undertaken to evaluate the PVP in terms of pain reduction and restoration of functional abilities among the patients suffering from symptomatic osteoporotic vertebral compression fracture.
Materials and Methods
An observational descriptive study, to evaluate the clinical outcome of PVP with follow up for one-year period, was conducted among the patients admitted and operated (PVP) between 2011 to 2013 for symptomatic osteoporotic vertebral compression fracture in the Department of Orthopaedics, IPGMER and SSKM Hospital, Kolkata, West Bengal, India. Patients with symptomatic osteoporotic vertebral compression fractures attended at Outpatient Department (OPD) and Emergency, were included as a study participants depending on the inclusion and exclusion criteria. Inclusion criteria were compression fractures of vertebral body, single or double confirmed by X-ray/CT scan/MRI, intractable pain related to the compression fracture, no other suspicious sources of pain as determined by imaging and clinical history, patient medically stable for the procedure and no other sources of neurological compromise and had given consent for the study. Exclusion criteria were laboratory findings suggesting other than osteoporosis responsible for compression fracture, vertebral compression fracture of more than one-year duration, spine pain that did not clinically correlate with the vertebral fracture, more than three fractured vertebras, neurological compromise, unstable fracture and refuse to give consent for the study. Patient determined to be medically unstable by primary care physician. Ethical clearance was obtained from the Institutional Ethics Committee of IPGMER and SSKM Hospital, Kolkata, West Bengal, India and informed consent was also taken from each study participants.
Considering inclusion and exclusion criteria, all the 25 patients consecutively underwent PVP under local anaesthesia for symptomatic osteoporotic vertebral compressive fracture within the study period were considered as study participants. Radiopaque vertebroplasty bone cement (Polymethyl methacrylate with 5% Hydroxyappetite) was used in all cases. Operative procedure is described below.
Operative procedure (PVP): The patient was positioned prone, with bolsters located under the sternum and pelvis in an attempt to reduce the kyphosis from the fracture. Under fluoroscopic guidance, an 11-gauge trocar with a cannula was inserted through or adjacent to the pedicle into the posterior aspect of the vertebral body. After proper mixing the cement, we filled the syringes with liquid cement and waited until the cement forms loops or threads [Table/Fig-1]; that means it had become sticky which would decrease the chances of cement leakage. Then, the cement was injected into the vertebral body under fluoroscopic control, ensuring that the cement remains within the confines of the vertebral body and, particularly, does not flow in a retrograde fashion into the spinal canal. Single dose of Injection Cefuroxime (1.5 g) was added for prophylaxis against infection [Table/Fig-2]. To minimize the incidence of cement leakage, few techniques were adopted, like not doing the procedure before three weeks, injecting the right amount of cement adequate for pain relief, injecting the cement with 2cc syringes, thus minimum chance of accidental over-injection, continuous fluoroscopic monitoring during injection, injecting the cement when it can form loops, means in semisolid stage as liquid cement can easily flow through small cracks and last but not the least, keeping the needle with stilet for some time (five minutes) after injection to prevent backflow.
Polymethayl Methacrylate (PMMA) bone cement formed a loop.

Multiple 2 c.c. syringes for injecting the cement.

The patients were evaluated by the Oswestry Disability Questionnaire (ODQ) [12], Visual Analogue Scale (VAS) [13] which was recorded at presentation, immediate postoperative, one week after the operation, one month after the operation, three months after the operation, then six monthly intervals postoperatively. Each and every patient was followed up for one year.
Statistical Analysis
The collected data were analyzed by IBM SPSS statistics version 20 software. Chi square test was applied for significance testing in case of categorical variables. Other parametric or non-parametric statistical tests were applied for continuous variables whenever applicable. A p-value <0.05 was considered as statistically significant.
Results
Among 25 study participants, there were 17 (68%) females and 8 (32%) males. The mean age of affected males was 66.3 (± 2.36) years and females was 61.5 (± 2.27) years. As the age of the study participants were not normally distributed, so non-parametric Mann-Whitney U test was applied and it was found that there was statistically significant age difference (p<0.001 at α 5%) among the male and female patients with respect to symptomatic osteoporotic vertebral compressive fracture. Females were presented at a younger age compared to male patients.
The most commonly affected segment was D12 (46.66%) followed by D11 (20%) and L1 (20%) and others (13.34%). Among the male patients L1 and D12 was equally affected and among females, D12 was mostly affected. Most of the cases (84%) were operated within three to four weeks after diagnosis; only four cases (16%) were operated after six weeks of diagnosis. The average cement used per segment was 2.9 (±0.13) cc.
Time taken to report significant pain relief after injection of the cement was tabulated bellow [Table/Fig-3]. The table shows that most of the patients (56%) reported pain relief postoperatively within 10 minutes, followed by 4 (16%) patients got pain relief within 10-20 minutes, 3 (12%) patients within 20-30 minutes and 4 (16%) patients took more than 30 minutes.
Time taken to report significant pain relief after injection.
| Gender | Time elapsed since operation |
|---|
| <10 minutes | 10-20 minutes | 20-30 minutes | >30 minutes |
|---|
| Male | 4 | 2 | 1 | 1 |
| Female | 10 | 2 | 2 | 3 |
| Total | 14 | 4 | 3 | 4 |
| Percentage | 56 | 16 | 12 | 16 |
Chisquare test for this 2X5 table shows that there is no statistically significant difference (p=0.86) among male and female patients with respect to duration to report pain relief after injection.
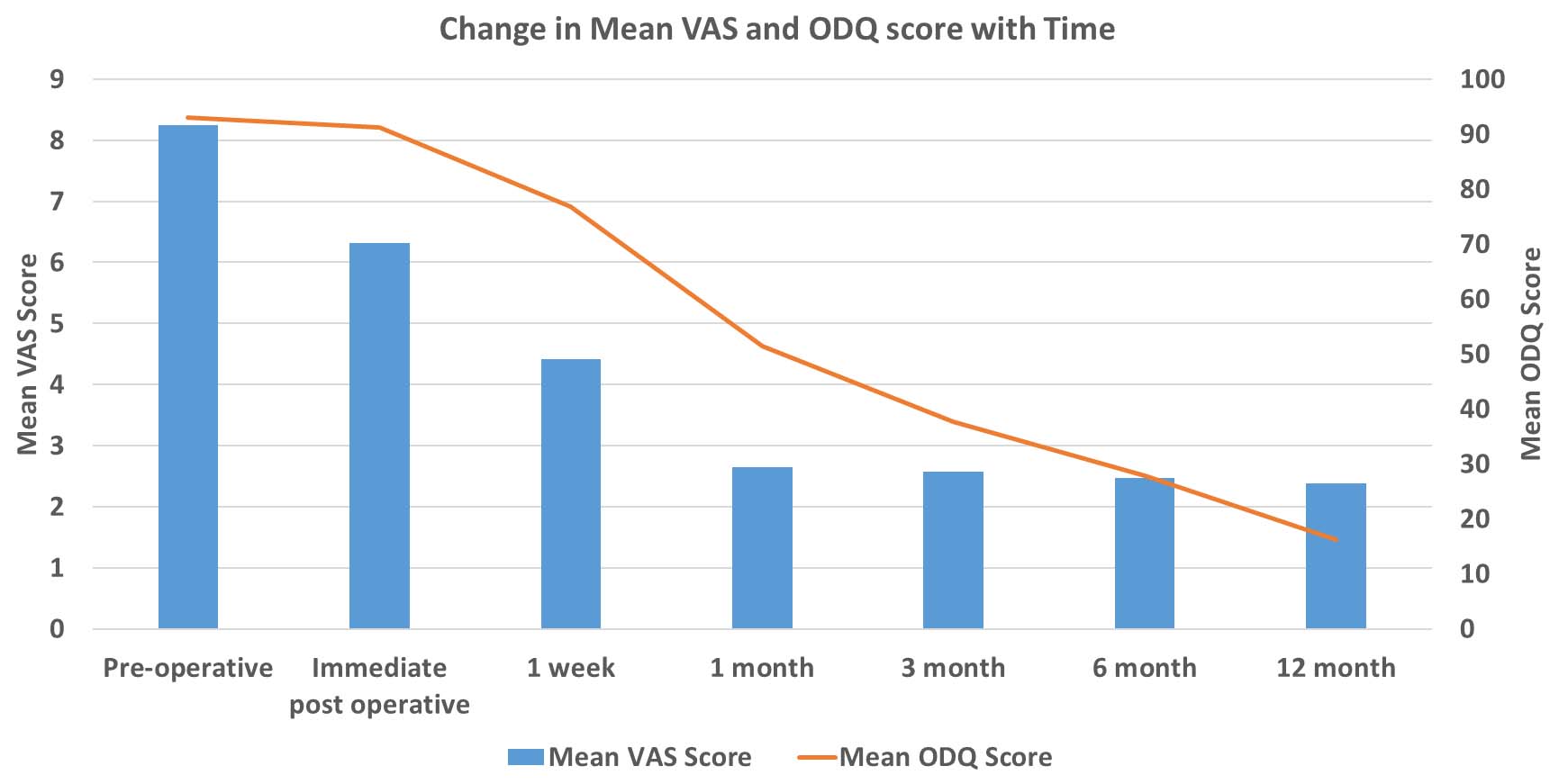
Mean VAS score and ODQ score and their interpretation at presentation and during follow up was tabulated below [Table/Fig-4]. There was a gradual decrease in both VAS and ODQ scores from preoperative period to end of follow up [Table/Fig-5]. VAS and ODQ scores were normally distributed among the study participants, so repeated measures ANOVA with Bonferroni post-hoc test was applied for significance testing.
VAS and ODQ score at different time point.
| Time point | VAS | ODQ |
|---|
| Mean (±SD) | Interpretation | Mean (±SD) | Interpretation |
|---|
| Preoperative at presentation | 8.24 (±1.16) | Severe pain | 93.01 (±4.54) | Bed-bound |
| Immediate postoperative | 6.31 (±1.21) | Moderate pain | 91.25 (±4.68) | Bed-bound |
| one week postoperative | 4.41 (±0.86) | Mild pain | 76.84 (±3.76) | Crippled |
| one month postoperative | 2.64 (±0.16) | No pain | 51.41 (±3.24) | Severe disability |
| three month postoperative | 2.58 (±0.09) | No pain | 37.6 (±3.14) | Moderate disability |
| six month postoperative | 2.47 (±0.06) | No pain | 27.8 (±2.89) | Moderate disability |
| 12 month postoperative | 2.38 (±0.08) | No pain | 16.23 (±1.17) | Minimal disability |
Change in mean VAS and ODQ score with time.
Mean VAS score and ODQ score and their interpretation at presentation and during follow up was tabulated below [Table/Fig-4]. There was a gradual decrease in both VAS and ODQ scores from preoperative period to end of follow up [Table/Fig-5]. VAS and ODQ scores were normally distributed among the study participants, so repeated measures ANOVA with Bonferroni post-hoc test was applied for significance testing.
Repeated measures ANOVA with Bonferroni post-hoc test shows that VAS score decreased significantly at immediate postoperative (p<0.001), at one week after operation (p<0.001) and at one-month postoperatively (p<0.001). Then there was no statistically significant (p>0.05) change in VAS score till 12 months, On the other hand, there was no significant change in ODQ score immediately after operation (p=0.18). Then disability, measured by ODQ score, significantly decrease (p<0.05) over time from one week to 12-month postoperatively. So, according to VAS score, preoperative severe pain subsided to no pain status at one month of operation and disability status improved from bed bound to minimal disability at one year of operation.
There was no postoperative complication among the operated patients during total one year follow up period, except two incidences of cement leakage, though there was no symptom for that.
Discussion
Among 25 patients, reduction in pain was reported by 56% of them within 10 minutes of operation. Mean VAS score at presentation was 8.24 (±1.16). It reduced to 6.31 (±1.21) and 2.38 (±0.08) at the immediate postoperative period and after 12 months respectively. This reduction in pain was statistically significant (p < 0.05). Disability, measured by ODQ score, significantly decrease (p<0.05) over time from one week to 12-month postoperatively. At presentation, ODQ score was 93.01 (±4.54). It reduced to 76.84 (±3.76) one wk after operation and 16.23 (±1.17) one year after operation.
Osteoporotic vertebral compression fractures are very commonly encountered in older age group [1]. Previously they were treated mainly by conservative methods with bed rest, bracing and anti-osteoporotic therapy which is often not very successful in relieving pain and preventing further deformity [2]. It was almost impossible to achieve painless full functional life for all those patients by newer treatment modalities [2]. Therefore, these patients are treated with a minimal invasive procedure like PVP [2]. In recent times, this procedure has become a very common practice and popular worldwide [14]. In our study, we are trying to evaluate the role of PVP in treating osteoporotic vertebral compression fractures in terms of symptomatic relief and any possible complication of the procedure.
Most of the studies like study conducted by Diel P et al., Prather H et al., and Mpotsaris A et al., commented on the short term benefit of the procedure after follow up period of at least 12 months, we have also followed up every patient up to 12 months, which is sufficient enough to comment on the short-term benefits and complications [3,9,15].
The fracture-procedure interval was different in different studies. Muijs SP et al., had done the PVP six weeks after fracture [16], Mpotsaris A et al., did the operation within 6-12 weeks [15], whereas Klazen CA et al., had done it within three to six weeks [17]. In our study, the average interval was 3.72 weeks.
The mean amount of injected cement varies in different studies mostly from 1.5-5.3 ml [15-17]. In our series, the mean value is 2.9 ml, which is within the range stated by others. In our series patients noticed a significant reduction in pain starting as early as from 10 minutes after the procedure. Though the exact time is not mentioned by other observers while they have pointed out that pain relief is immediate and completes within one week [17]. Improvement in pain scores, measured by VAS, and functional capabilities, measured by ODQ, were observed at one week after operation and that improvement were maintained up to 12 month postoperative follow up, This result is also comparable to other researchers’ experience like Prather H et al., Mpotsaris A et al., and Muijs SP et al., [9,15,16].
Cement leakage was observed in two cases at two weeks after injection. Asymptomatic radiological cement leakage was cited as a most common complication by all the studies, whereas pulmonary cement embolus, spinal cord injury was also reported rarely [15-17]. Incidence of cement leakage varies from 6% to 15% usually, whereas very high incidence (82%) was reported by Martin DJ et al., [18]. In our study, it was observed 6.3% leakage among the segments and 8% leakage among the patients.
Lavelle W et al., stated that kyphoplasty was a better procedure for osteoporotic vertebral compression fracture as the height of the vertebra can be restored, while in terms of pain relief and restoration of functional ability both are same [19] while cement leakage is stated as a common problem in vertebroplasty by Muijs SP et al., [16].
Limitation
The limitation of our study is that we don’t have a large patient number. The study would have been more analytical if we could have compared it with other modes of management. We did not find any recurrence of pain or adjacent level fracture in our study, may be long follow up is needed to comment on that.
Conclusion
PVP has become a common practice worldwide for its benefits with fewer side effects for symptomatic osteoporotic vertebral fractures. In this study, satisfactory results were observed with this procedure in terms of excellent pain relief and internal stability to the fractured vertebra thus preventing further collapse and progression of kyphosis, allowing the patients to regain normal activity at the earliest, at a very reasonable cost with minimal complication.
Chisquare test for this 2X5 table shows that there is no statistically significant difference (p=0.86) among male and female patients with respect to duration to report pain relief after injection.