The prevalence of cardiovascular diseases has been increasing over the past two centuries. According to a World Health Organization (WHO) report, cardiovascular diseases are the main leading causes of death worldwide [1-3]. Coronary artery disease is the leading cause of death, disability, and financial burden compared to other diseases [4].
Coronary artery disease can be found in various locations such as the proximal, mid, and distal parts of the arteries or even simultaneous disease of several arteries [5].
Right and left coronary arteries supply blood to the heart muscle. Coronary arteries are the first branches that separate from the aorta and are separated from the right and left Valsalva sinus. The Left Main (LM) coronary artery which is separated from the left Valsalva sinus is divided into two branches - the Left Anterior Descending artery (LAD) and Left Circumflex artery (LCX).
The LAD runs through the anterior interventricular groove toward the apex. This artery consists of three parts: proximal, mid, and distal. The LCX which has two parts, proximal and distal, runs backward through the left inter atrioventricular groove. The Right Coronary Artery (RCA) is separated from the right Valsalva sinus and runs through the right inter atrioventricular groove to the crux. RCA consists of three parts: proximal, mid, and distal [6]. Various risk factors exist for coronary artery disease. Adjustable risk factors for this disease include hyperlipidemia, hypertension, diabetes mellitus, smoking, obesity, lack of exercise, and excessive alcohol ingestion. Either avoiding or treating these risk factors can dramatically decrease the risk of coronary artery disease [1,2,7]. Although there are known risk factors for coronary artery diseases, a number of these risk factors have greater significance [8,9].
Our hypothesis is, the number of involved coronary arteries and existence of major risk factors have a positive relationship. Also, possibly some of these risk factors may involve proximal part of the coronary arteries and they are different between Iranian patients in compare to other ethnics.
This study aimed to recognize the pattern of coronary artery disease and its relationship with a number of well-known, preventable risk factors in patients with coronary artery disease who presented to Farshchian Heart University Hospital, Hamadan, Iran. These findings should enable health care providers to reduce or treat coronary artery disease risk factors by planning.
Materials and Methods
In this descriptive cross-sectional study, trained staff at Farshchian Heart University Hospital reviewed the files of patients diagnosed with coronary artery disease by coronary angiography from January 2010 to December 2014. The required data were registered in a manual checklist. Staff extracted the following data from patients’ files: file number, gender, age (years), and risk factors that included hyperlipidemia, diabetes mellitus, hypertension, and existence of a history of coronary artery disease in first degree relatives. The risk factors were collected as “yes” or “no” answers on the checklist. We collected the following coronary angiography result – presence of Single Vessel Disease (SVD), 2-Vessel Disease (2VD), or 3-Vesssel Disease (3VD), in addition to the location of their coronary disease (proximal, mid, or distal). A cardiologist performed the coronary angiographies with a Siemens Axiom Artis. We excluded all patients with the following three criteria: i) presence of valvular disorders; ii) presence of congenital heart diseases; or iii) lack of data in patients’ files.
We defined significant stenosis as the presence of >50% stenosis in the main left coronary artery and when significant stenosis in the LAD, LCX, and RCA arteries was ≥70% [6].
Statistical Analysis
The checklist data was analysed by SPSS software version 16.0 (Chicago, IL, USA). Variables were reported as mean and standard deviation and percentage. For comparing the history of risk factors in terms of coronary artery disease Chi-Square test was used. The p-value <0.05 was considered to be statistically significant. Ethical committee waived ethical considerations.
Results
Among 1154 of patients presented with coronary artery disease, 54 cases were excluded due to lack of data. There were 743/1100 (67.5%) males and 357/1100 (32.5%) females. We observed SVD in 558 (50.7%) of patients, 257 (23.4%) had 2VD, and 285 (25.9%) had evidence of 3VD.
Patients with SVD had a mean age of 52.2 (SD: 10.4) years, whereas those with 2VD were 61.5 (SD: 10.8) years old and patients with 3VD had a mean age of 65.4 (SD: 10.9) years (p<0.001).
Among 558 cases with SVD there were 384 (68.9%) males and 174 (31.1%) females. The 257 cases with 2VD consisted of 175 (68%) males and 82 (32%) females. This rate was 184 (64.5%) males and 101 (35.5%) females in the 285 cases with 3VD.
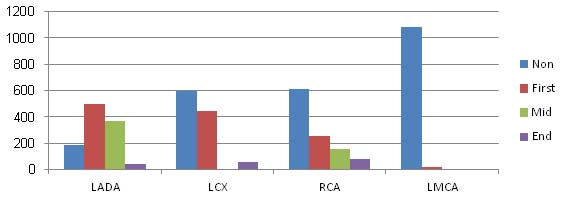
In terms of LAD disease, 322 (64.9%) of males and174 (35.1%) of the females had disease in the proximal area. LAD disease in the mid area was observed in 240 (65%) of males and 129 (35%) of females, whereas 36 (78.2%) of males and 10 (21.8%) of females had disease in the distal area.
Frequency of patients with LCX was 290 (64.8%) (males) and 158 (35.2%) (females) at the proximal area. Distal disease of LCX was seen in 51 (88%) of males and 7 (12%) of females.
RCA disease in the proximal area was 172 (67.7%) (males) and 82 (32.3%) (females), whereas there were 96 (61.5%) (males) and 60 (38.5%) (females) with RCA disease in the mid area. Distal disease of the RCA was seen in 60 (78%) of males and 17 (22%) of females. Disease at the proximal section in LMCA was observed in 11 (64.7%) of males and 6 (35.3%) of females.
Another result about the relationship between some major risk factors and diseased coronary arteries were showed in [Table/Fig-1,2,3,4 and 5].
Relationship between risk factors and the number of involved coronary arteries.
| Variables | Yes/No | SVD*N (%)***** | 2VD**N (%) | 3VD***N (%) | p-value**** |
|---|
| Diabetes Melitus | Yes | 73 (13%) | 60 (23%) | 188 (66%) | <0.001 |
| No | 485 (87%) | 197 (77%) | 97 (34%) |
| Hypertension | Yes | 175 (31%) | 131 (51)% | 195 (68.5%) | <0.001 |
| No | 383 (69%) | 126 (49%) | 90 (31.5%) |
| Family History | Yes | 70 (13%) | 61 (26%) | 46 (16.6%) | 0.007 |
| No | 457 (87%) | 174 (74%) | 231 (83.4%) |
| Hyperlipidemia | Yes | 117 (21%) | 85 (33%) | 99 (35%) | <0.001 |
| No | 436 (79%) | 172 (67%) | 182 (65%) |
* single vessel disease ** 2-vessle disease *** 3-vessel disease
****by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
***** Number (Percent)
Coronary artery involved part distribution based on age
| Involved Artery | Involved Part | Mean Age** | SD* |
|---|
| LAD | Proximal | 61.6 | 11.5 |
| Mid | 60.9 | 10.30 |
| Distal | 58.2 | 9.3 |
| LCX | Proximal | 63.9 | 11 |
| Distal | 62.4 | 11.2 |
| RCA | Proximal | 63 | 11.5 |
| Mid | 64 | 11.4 |
| Distal | 59.8 | 10.1 |
| LMCA | Proximal | 68.4 | 11.1 |
*by Descriptive Statistics(Explorel).
The relationship between hypertension, hyperlipidemia with coronary arteries involved part.
| Coronary Artery | Involved Part | Hypertension | p-value* |
|---|
| | Positive historyN (%) | Negative historyN (%)** | |
|---|
| LAD | Proximal | 279 (56.2%) | 217 (43.8%) | <0.001 |
| Mid | 162 (44%) | 207 (56%) |
| Distal | 9 (20%) | 37 (80%) |
| LCX | Proximal | 270 (60.2%) | 178 (39.8%) | <0.001 |
| Distal | 21 (36%) | 37 (64%) |
| RCA | Proximal | 155 (61%) | 99 (39%) | 0.048 |
| Mid | 82 (52.5%) | 74 (47.5%) |
| Distal | 25 (32.5%) | 52 (67.5%) |
| LMCA | Proximal | 13 (76.5%) | 4 (23.5%) | 0.009 |
| | Hyperlipidemia | |
| PositivehistoryN (%) | NegativehistoryN (%) |
| LAD | Proximal | 161 (33%) | 331 (67%) | 0.001 |
| Mid | 99 (27%) | 270 (73%) |
| Distal | 9 (19.6%) | 37 (80.4%) |
| LCX | Proximal | 140 (30.9%) | 308 (69.1%) | 0.025 |
| Distal | 18 (31%) | 40 (69%) |
| RCA | Proximal | 81 (33%) | 167 (67%) | 0.052 |
| Mid | 52 (33.5%) | 103 (66.5%) |
| Distal | 20 (26%) | 57 (74%) |
| LMCA | Proximal | 6 (35%) | 11 (65%) | 0.3 |
*by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
**Number (Percent)
The relationship between diabetes mellitus, family history and coronary artery disease part.
| Coronary Artery | Involved Place | Diabetes Melitus | p-value* |
|---|
| | Positive historyN(%) | Negative historyN (%)** | |
|---|
| LAD | Proximal | 208 (42%) | 288 (58%) | 0.01 |
| Mid | 84 (30%) | 285 (70%) |
| Distal | 7 (15%) | 39 (85%) |
| LCX | Proximal | 217 (48.5%) | 231 (51.5%) | 0.066 |
| Distal | 9 (15%) | 49 (85%) |
| RCA | Proximal | 142 (56%) | 112 (44%) | 0.026 |
| Mid | 51 (33%) | 105 (67%) |
| Distal | 22 (38.5%) | 55 (71.5%) |
| LMCA | Proximal | 15 (88%) | 2 (22%) | 0.026 |
| | Family History | |
| Positive historyN(%) | Negative historyN (%) |
| LAD | Proximal | 81 (17%) | 388 (83%) | 0,69 |
| Mid | 58 (17%) | 285 (83%) |
| Distal | 9 (19.5%) | 37 (80.5%) |
| LCX | Proximal | 87 (20.6%) | 337 (79.4%) | 0.06 |
| Distal | 8 (13.8%) | 50 (86.2%) |
| RCA | Proximal | 37 (15%) | 212 (85%) | 0.66 |
| Mid | 27 (19%) | 115 (81%) |
| Distal | 23 (31%) | 51 (69%) |
| LMCA | Proximal | 2 (12%) | 15 (88%) | 0.42 |
*by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
**Number (Percent)
Frequency distribution of coronary arteries disease place.
Discussion
In this study, we observed a meaningful relationship between age and LCX, LMCA, and RCA disease at the proximal section and the number of diseased coronary arteries. Among patients with diabetes mellitus and hypertension, we observed significantly more patients with 3VD, whereas those with hyperlipidemia and positive family histories had significantly more SVD. A relationship existed between diabetes mellitus and proximal RCA and LMCA disease. We also observed this relationship between hypertension and hyperlipidemia with proximal left circumflex and RCA disease.
In a case-control study in Tehran, Iran that included 125 patients in both groups, the relationship between diabetes mellitus with proximal coronary arteries disease was observed, however, they did not observe any relationship between hypertension, hyperlipidemia, and coronary artery disease. No relationship existed between hypertension and the number of diseased coronary arteries. However, 22% of patients had diabetes. The prevalence of SVD in diabetic patients was 10.9%, whereas the prevalence of multivessel disease was 89.1% in this group of patients. Non-diabetic patients had a prevalence of 39% for SVD and 61% for multivessel disease. The authors observed a meaningful relationship between diabetes mellitus and multivessel disease, which was similar to the current study [10].
A cross-sectional study in Kerman, Iran enrolled 196 patients who suffered from coronary artery disease. They reported that patients with 3VD had more diabetes mellitus and hypertension [5]. Their results were the same as of the present study.
A cross-sectional study in Mazandaran, Iran on 201 patients showed a meaningful relationship between intensity of coronary artery disease (number and extent) with the following risk factors: diabetes mellitus, hyperlipidemia, and hypertension which supported the findings of the current study. There was no relationship with family history and other risk factors [11].
In three studies performed on various races in New York, researchers investigated the relationship between risk factors and pattern of coronary artery disease. The first study included 75 patients from Bangladesh and 57 patients from other nationalities. The researchers observed that only race affected the pattern of coronary artery disease [12].
The second study compared 198 Indian patients with 191 Caucasian patients. This study revealed that, among major risk factors, old age and male sex were associated with high prevalence of 3VD [13].
The third study compared 520 South Asian patients with 219 Caucasians. Similar to the current study, increased age, diabetes mellitus, hyperlipidemia and hypertension were the effective risk factors for coronary artery disease. There were no meaningful relationships observed between other risk factors in both groups [14].
Researchers in two case-control studies from Japan reported that hypertension, diabetes mellitus, and hyperlipidemia were common effective risk factors in coronary artery disease in patients who suffered from acute myocardial infarction. However, they did not observe any relationship between other investigated risk factors [15,16]. In the current study, a positive family history had no relationship with patterns of coronary artery disease.
Another study in India reported a probability of increased coronary artery disease in patients with diabetes mellitus and hypertension. In this study, only increased age showed a relationship with LMCA disease and increased numbers of diseased arteries. There was a greater probability of LMCA disease in diabetic patients [17].
A milder disease on angiography and a lower incidence of multiple vessel disease is a common finding in a study in North Indian women comparing to men [18].
Another study which was conducted on the patient younger than 45 years old with acute myocardial infarction as their first presentation of coronary artery disease; hypertension, hyperlipidemia, diabetes mellitus and smoking had positive relationship with this manifestation. Despite of unknown number of diseased coronary arteries in this study, but at overall, congruity between the result of this study and ours was consistent [19].
The different findings reported by these studies might be attributed to the differences in study designs, variables in demographics, geographical differences and genetics.
Limitation
Unknown precise duration of hypertension, hyperlipidemia and diabetes mellitus is a major limitation for results interpretation.
Conclusion
Risk factors such as diabetes mellitus and hypertension have a stronger relationship with 3-vessel coronary artery disease. Diabetes mellitus, hypertension and hyperlipidemia show a considerable relationship with coronary artery disease at the proximal part of the arteries. According to this study, we advise that health care providers take into consideration a basic plan in order to decrease the impact of these risk factors on coronary artery disease.
* single vessel disease ** 2-vessle disease *** 3-vessel disease
****by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
***** Number (Percent)
*by Descriptive Statistics(Explorel).
*by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
**Number (Percent)
*by Chi-Square Test, A p-value <0.05 was considered to be statistically significant
**Number (Percent)