Hypertension is considered as one of the major risk factor for the development of cardiac and cerebrovascular diseases, playing an important role in the development of atherosclerosis, as well as modifying the geometry of the left ventricle resulting in an increase in the wall thickness and cardiac mass. Authors estimate that from 1975 to 2015, the number of adults with this problem have increased from 594 million to more than 1.1 billion. Furthermore, many hypertensive patients remain undiagnosed for years and several are not diagnosed correctly and are inappropriately treated for decades [4].
The high sensitivity C-Reactive Protein (hs-CRP) is an inflammatory marker that has been commonly associated with CVD. It may be related to chronic inflammatory conditions, such as atherosclerosis and after adjusting for risk factors for CVD, patients with high CRP levels, are at a higher risk of suffering from acute myocardial infarction [5]. Besides the increase, this biomarker has also been related to the increase of cardiovascular risk in patients with established disease and the occurrence of the first vascular event. These facts show that hs-CRP is valuable in primary and secondary prevention and prophylaxis. For the CVD patients the evaluation of this marker may help in the evaluation of the severity of the disease, efficacy of the treatment and prognosis [6].
Hypertension is associated with atherosclerosis that may interfere in the oxide LDL-c uptake by macrophages resulting in vascular vulnerability. Reduction of blood pressure in the elderly hypertensive patients decreases morbidity and mortality. Basic researches may be helpful in avoiding incorrect diagnosis and may improve the medical approach once it predicts short and long terms outcomes. It is an independent marker in asymptomatic multiple ethnic groups [7]. It is well established that there is a relationship between the presence and severity of arterial lesions and hs-CRP, and it is known that nearly half of infarctions may happen in patients who do not present with dyslipidemia [6]. For these reasons, the aim of this study was to verify the association among hs-CRP levels, metabolic profile and severity of the disease in hypertensive and non-hypertensive patients who underwent arteriography.
This study is part of a larger project involving patients who attended the Haemodynamics Unit of the University Hospital.
Materials and Methods
This study was transversal and analytical, it was performed at the Haemodynamic Laboratory of the University Hospital in the city of Marilia - state of São Paulo, Brazil. The subjects were recruited by the convenience sampling technique and comprised of patients attending the hospital from February 2012 to July 2012, who satisfied the inclusion criteria of the study (adult and elderly patients who underwent arteriography and accepted to undergo all necessary biochemical and anthropometric evaluations required for the study). Ninety-five subjects were included in this study (male: 52; female: 43 aging 36 to 88 years). The procedures were approved by the Ethical Committee of the University of Marilia (Protocol 449 / Record 25000.113733/2010-14) and only started after the subjects signed a Free and Informed Consent Form (Resolution 196/10 of October 1996 – National Health Council – CNS). The experimental protocol was in accordance with the Ethical Standards of the Institutional Ethical Committee and the Helsinki Declaration of 1975 (revised in 2008).
In a preliminary statistical analysis, we observed that the gender was not a determining factor in the studied parameters, for this reason we performed the study with male and female in the same sample.
Anthropometric and biochemical parameters: The Body Mass Index (BMI) was calculated using the formula weight/(height)2 (Kg/m2). Waist circumference was measured midway between the bottom edge of the last rib and the iliac crest in the mid-axillary plane. Blood pressure (BP) was evaluated according to the diagnostic criteria of the “2014 evidence-based guideline for the management of high blood pressure in adults” [8].
Blood sample was collected in order to measure glycaemia, Total Cholesterol (TC), Low-Density Lipoprotein Cholesterol (LDL-c), High-Density Lipoprotein Cholesterol (HDL-c), Triglycerides (TG) and level of high sensitivity-CRP (hs-CRP) {levels of hs-CRP were classified as high (>0.3 mg/dL), moderate (0.1 – 0.3 mg/dL) and low (<0.1 mg/dL)} [9].
Castelli Index I (CI-I) was calculated using TC/HDL-c and for Castelli Index II (CI-II) we used LDL-c/HDL-c ratios (normal values are respectively ≤ 4.4 and 2.9). The estimate of low density lipoprotein particle size was performed by the ratio TG/HDL-c (≤ 2.0 mg/dL is relative to small and dense particles (sdLDL-c) [10].
Metabolic syndrome diagnosis: The occurrence of at least three alterations in the following parameters was used to classify the presence of Metabolic Syndrome (MS): blood pressure, BMI, glycaemia, TG, and HDL-c [11].
Arterial lesions: The catheterization report was classified for this work as: severe coronary lesion (over 70%), moderate coronary lesion (50-70%), mild coronary lesion (less than 50%) and no lesion [12].
Statistical Analysis
BioEstat program was used in order to analyse the data and the following tests were used: Chi-square test, Fisher, Student t-test and ANOVA complemented by Tukey test. A level of significance of 5% was applied to all the conclusions obtained from the inferential analysis.
Results
In [Table/Fig-1] it can be observed that most individuals of this study presented with HBP, MS, and DM. The comparison between hypertensive and non-hypertensive patients shows that there are significant differences related to the presence of MS and DM.
Subjects of the study according to the presence or absence of hypertension, metabolic syndrome, and type 2 Diabetes mellitus.
| Parameter | Hypertensive n = 75 (78.95 %) | Non-hypertensive n= 20 (21.05 %) | Total |
|---|
| MS | 70 (93.33%) | 6 (30.00%) | 76 (80.00%) |
| p-value | 0.0123* | |
| DM2 | 39 (52.00%) | 4 (20.00%) | 43 (45.26%) |
| p-value | 0.0213* | |
MS: Metabolic syndrome; DM2: Type 2 Diabetes mellitus.
Chi-square test.
[Table/Fig-2] shows significant differences among hypertensive and non-hypertensive patients in glycaemia, triglycerides, waist circumference, body mass index and hs-CRP.
Biochemical parameters of the subjects according to the presence of hypertension.
| Parameter | Hypertensive n = 75 (78.95 %) | Non-hypertensive n= 20 (21.05 %) | p-value |
|---|
| Glycaemia (mg/dL) | 124.14 ± 45.33* | 101.90 ± 20.09 | 0.0388 |
| CT (mg/dL) | 180.75 ± 41.38 | 169.75 ± 44.14 | 0.0621 |
| HDL-c (mg/dL) | 44.45 ± 11.85 | 47.05 ± 11.02 | 0.0700 |
| LDL-c (mg/dL) | 108.85 ± 37.51 | 107.56 ± 39.83 | 0.0662 |
| TG (mg/dL) | 195.27 ± 74.52* | 124.25 ± 57.94 | 0.0421 |
| Castelli Index I | 4.25 ± 1.52 | 4.06 ± 1.43 | 0.0993 |
| Castelli Index II | 2.57 ± 1.33 | 2.45 ± 1.11 | 0.0832 |
| Size of LDL-c particle | 3.65 ± 3.93 | 3.04 ± 2.55 | 0.0706 |
| hs-CRP (mg/dL) | 0.53 ± 0.44* | 0.38 ± 0.21 | 0.0118 |
| WC (cm) | 98.52 ± 12.52* | 92.15 ± 13.02 | 0.0301 |
| BMI (kg/m2) | 29.99 ± 1.41* | 25.75 ± 3.87 | 0.0435 |
significant difference at a level of 5%.
TC: total cholesterol; TG: triglycerides; HDL-c: high density lipoprotein; LDL-c: low density lipoprotein; TG: triglycerides; Castelli Index I: TC/HDL-c; Castelli Index II: LDL-c/HDL-c; Estimative of the size of LDL-c particle: TG/HDL-c; hs-CRP: high sensitivity C reactive protein; BMI: body mass index; WC: waist circumference.
Our results show that most subjects undergoing arteriography are classified as having hypertension, and most of these hypertensive patients have glucose intolerance or DM, and significantly higher values of WC, BMI, and hs-CRP [Table/Fig-1,2].
We may observe in [Table/Fig-3] that there are significant differences among high, moderate and low levels of hs-CRP in hypertensive patients.
Values of hs-CRP in patients according to the presence of hypertension.
| hs-CRP (mg/dL) | Hypertensive n = 75 (78.95 %) | Non-hypertensive n= 20 (21.05 %) | Total |
|---|
| High | 38 (50.67%) | 6 (30.00%) | 44 (46.32%) |
| Moderate | 10 (13.33%) | 9 (45.00%) | 19 (20.00%) |
| Low | 27 (36.00%) | 5 (25.00%) | 32 (33.68%) |
Chi-square test, p-value=0.0069, hs-CRP: high sensitivity C reactive protein.
In [Table/Fig-4] we observe significant differences between classification of hs-CRP in hypertensive patients and non-hypertensive patients only for Castelli Index I and WC.
Biochemical parameters of the subjects according to the presence of hypertension and classification of hs-CRP.
| Parameter | hs-CRP (mg/dL) |
|---|
| High | Moderate | Low |
|---|
| Hypertensive | Non-Hypertensive | Hypertensive | Non-Hypertensive | Hypertensive | Non-Hypertensive |
|---|
| n | 38 (40.00%) | 6(6.32%) | 10 (10.53%) | 9(9.47%) | 27(28.42%) | 5(5.26%) |
| Glucose (mg/ L) | 119.58±48.07 | 92.83±18.65 | 133.58±47.41 | 108.44±21.99 | 116.90±22.74 | 101.00±17.13 |
| TC (mg/L) | 185.21±45.70 | 163.17±29.16 | 177.78±42.79 | 183.78±48.58 | 192.90±44.86 | 180.80±40.59 |
| LDL-c (mg/L) | 111.00±44.22 | 92.63±26.06 | 106.83±36.35 | 101.76±39.20 | 96.48±31.55 | 103.08±45.78 |
| HDL-c (mg/L) | 41.58±10.77 | 47.83±11.58 | 46.11±11.13 | 48.67±11.39 | 50.90±15.17 | 43.20±11.14 |
| TG (mg/L) | 166.21±147.89 | 113.50±40.17 | 124.19±56.60 | 126.78±98.72 | 122.60±70.14 | 132.60±84.09 |
| Castelli Index I | 4.65±1.77* | 3.17±1.05 | 3.98±1.12 | 4.03±1.58 | 3.50±1.00 | 4.69±1.19 |
| Castelli Index II | 2.84±1.61 | 2.04±0.81 | 2.40±0.93 | 2.42±1.08 | 2.12±0.75 | 1.98±1.45 |
| Size of LDL-c | 4.47±5.16 | 2.62±1.41 | 2.90±1.74 | 3.02±3.05 | 3.58±1.68 | 2.59±3.02 |
| WC (cm) | 99.86±13.54* | 90.17±7.61 | 97.89±12.53 | 92.22±11.84 | 95.40±8.28 | 94.40±11.15 |
| BMI (kg/m2) | 29.61±4.59 | 27.04±4.85 | 26.95±4.27 | 27.23±4.02 | 26.87±2.45 | 25.53±2.64 |
HPB: high blood pressure; hs-CRP: high sensitivity C reactive protein; TC: total cholesterol; TG: triglycerides; HDL-c: high density lipoprotein; LDL-c: low density lipoprotein; Castelli Index I: TC/HDL-c; Castelli Index II: LDL-c/HDL-c; Estimative of the size of LDL-c particle: TG/HDL-c; BMI: body mass index; WC: waist circumference.
Significant; p<0.05
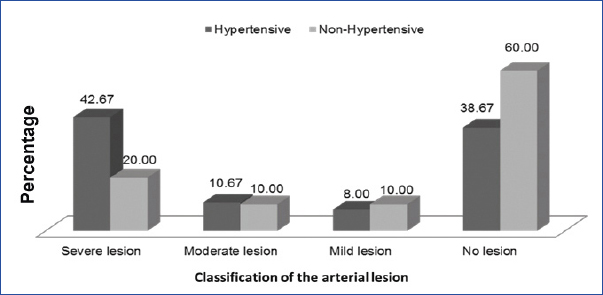
In [Table/Fig-5] it is possible to observe that in the group of severe and moderate lesion, patients with hypertension are in greater number when compared to non-hypertensive and in those without lesions or with mild lesion, the opposite is observed.
Patients according to the presence of hypertension and catheterization report for: severe coronary lesion, moderate coronary lesion, mild coronary lesion and no lesion.
*Chi-square test; p-value = 0.2739
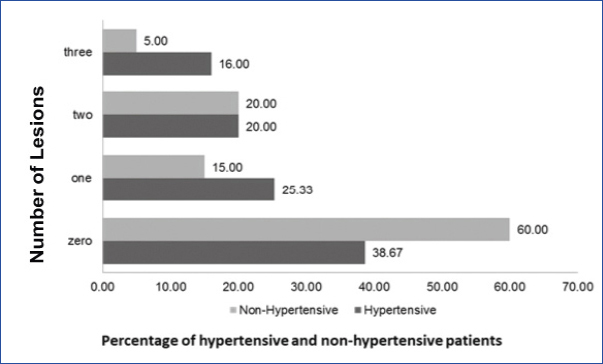
[Table/Fig-6] shows the comparison in patients with or without hypertension. The presence of one or three arteries with obstruction tend to be higher in hypertensive patients. In the group of patients without lesions, it is possible to see that most of them are not hypertensive.
Patients according to the presence of hypertension and number of affected arteries.
*Chi-square test; p-value = 0.2851
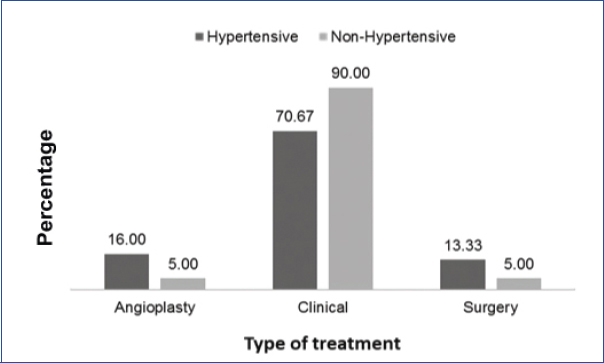
In [Table/Fig-7], we observe that most individuals included in this study underwent clinical management, angioplasty or surgery, those ones classified as having HBP are greater in number.
Patients according to the presence of hypertension and the treatment.
*Chi-square test; p-value = 0.2088
Discussion
In agreement with our results, some authors as Feng YH and Fu P and Camara A et al., also found association between hypertension and DM [13,14]. The glucose intolerance or DM are normally related to the increase of the BMI that is also related to the synthesis of inflammatory markers [15]. The visceral obesity is also known to play a role in the development of obesity-related comorbidities. Authors have shown that glucose intolerance and obesity, apart from its relationship with inflammation processes, are also involved in the oxidative stress and is important in the development of inflammatory and thrombotic processes. Hyperglycaemia increases the morbidity and mortality possibly resulting from complications associated with the resistance to insulin [16].
Our results also showed the prevalence of MS in the hypertensive patients. The MS has a polygenic and multifactorial origin and is associated to a cluster of risk factors represented by HBP, obesity, visceral fat, glucose intolerance, high levels of triglycerides and LDL-c, and low levels of HDL-c, which increase the chances of developing type II DM and CVD. These factors are also associated with the morbidity and mortality of the patients [17].
We may consider other possibilities in the clinical stratification of CVD as alterations in the Castelli Index I and II as well as the estimate of the LDL-c particle. These ratios may work as an additional tool to study the cardiovascular risk. Castelli Index I and II indicate that the patient is at higher CVD risk [9]. The sdLDL-c particles indicate increased risk for developing CVD once these particles cannot be recognized by LDL-c receptors and are highly susceptible to peroxidation. Low levels for HDL-c, high levels of TG and sdLDL-c are independent risk factors for cardiac injuries [18]. The overproduction of sdLDL-c and its oxidation makes it capable to easily permeate the arterial wall cells contributing to atheromatous plaque formation. Several authors have pointed the relationship between sdLDL-c and hypertension [10,18,19].
Level of hs-CRP was also higher in patients with HBP, in our study. This protein is produced by adipocytes and liver and is regulated by Interleukin-1 (IL-1), IL -6 and Tumour Necrosis Factor-α (TNF-α) and may be routinely measured. High values for BMI and WC are associated with CVD due to the release of these inflammatory biomarkers, that is associated with sedentary lifestyle may promote the installation of a low intensity inflammatory process. This condition intensifies the production of inflammatory markers such as hs-CRP and other reactive species that damage the vascular endothelium and augment the risk of acute myocardial infarction [20].
High hs-CRP values are frequently found in hypertensive patients and it is currently considered as an independent risk factor for hypertension [21]. Authors have postulated that this biomarker can aggravate hypertension via several mechanisms once it participates in systemic and local inflammatory responses and may damage vascular endothelial cells, resulting in the decrease of nitric oxide and prostaglandins. Furthermore, it can lead to the thickening of vascular intima inducing the installation and progression of atheroma, resulting in the peripheral resistance; and decreasing the vascular reactivity to vasodilators, and blood flow speed aggravating vascular sclerosis and increase of the blood pressure [22].
Hypertensive patients in our study presented BMI and WC above normal values. Authors have shown the relationship among these parameters and HBP. Camara A et al., investigated the prevalence of hypertension in African patients and found association with obesity [14]. Obese individuals normally present with hypertension and related cardiovascular diseases, which, nowadays is a serious worldwide health problem reaching epidemic proportions and affecting both paediatric and adult populations [23]. Obesity is associated with hypertension, increase in the release of hs-CRP, dyslipidemia, diabetes, CVD, reduction in the life expectancy and increase in the morbidity [13,24].
Our data suggests that hypertensive patients when compared to non-hypertensives are more prone to the presence of one or three affected arteries, to the presence of more severe lesions and more invasive procedure [Table/Fig-5,7]. Carpenter M et al., also found association between hypertension and the presence of plaques and surgical therapeutics [25]. These authors performed a review related to the carotid intima media thickness and its link to the increased risk of CVD and subsequent events in the general population and in the high-risk groups, such as those with hypertension. Other studies also found similar associations [26,27].
Authors have suggested that cardiovascular outcomes are lowest in patients who have achieved blood pressure of less than 130/80 mmHg [1]. Rapsomaniki E et al., found that people with hypertension (blood pressure =140/90 mm Hg or those receiving blood pressure-lowering drugs) had a lifetime risk of overall cardiovascular disease at 30 years of age of 63.3% (95% CI 62.9–63.8) compared with 46.1% (45.5–46.8) for those with normal blood pressure, and developed cardiovascular disease 5·0 years earlier (95% CI 4.8–5.2) [28]. Our findings show that HBP may be associated with different cardiovascular outcomes and is an important component to be considered in patients who underwent arteriography in order to reduce further cardiovascular complications.
Several evidences have indicated that HBP is related with the modification of the arterial walls, through the vasoactive peptides angiotensin and endothelin-1 that induces and accelerates the atherosclerotic process due to inflammatory mechanisms [29]. The Angiotensin II stimulates Nicotinamide Adenine Dinucleotide Phosphate (NADPH)/Nicotinamide Adenine Dinucleotide (NADH) oxidase in the endothelium, as well as in the smooth muscle cells, and the adventitia, producing reactive oxygen species. This process results in endothelial dysfunction, inflammation and increased breakdown of Nitric Oxide (NO), contributing to the progression of vascular disease and atherogenesis. Furthermore, hypertension, inflammation and atherosclerosis together, potentiate endothelial dysfunction, which in turn perpetuates the harmful action of this dysfunction, aggravating the dysfunction of the endothelium (vicious circle) [30].
It is noteworthy to remember that the high hsCRP may also be associated with atheromatous plaques in the vascular wall and with the release of IL-1β, IL-6 and TNF-α by activated monocytes, as well as the expression of Intracellular Adhesion Molecule-1 (ICAM-1) and Vascular Adhesion Molecule-1 (VCAM-1) by endothelial cells. hsCRP also causes potent down-regulation of transcription eNOS (synthase of nitric oxide) on the endothelial cells and destabilizes the function of the mRNA of eNOS, resulting in a reduction in the production of NO [31,32]. This decrease appears to be the critical step in the development of atherosclerosis, hypertension, and other vascular events [33,34].
Limitation
One limitation of our study is the size of the sample. If it were larger, we would have had the data that could be extrapolated to populations beyond those found in this research.
Conclusion
Our data shows that most of the patients who underwent arteriography suffer from hypertension, MS and are related to the presence of more severe lesions in the arteries, and had undergone more invasive procedures like angioplasty and surgery. Our findings indicate that the blood pressure control is of paramount importance to ensure better quality of life and life expectancy once it is associated to several risk factors that increase the morbidity and mortality of CVD.
MS: Metabolic syndrome; DM2: Type 2 Diabetes mellitus.
*Chi-square test.
*significant difference at a level of 5%.
TC: total cholesterol; TG: triglycerides; HDL-c: high density lipoprotein; LDL-c: low density lipoprotein; TG: triglycerides; Castelli Index I: TC/HDL-c; Castelli Index II: LDL-c/HDL-c; Estimative of the size of LDL-c particle: TG/HDL-c; hs-CRP: high sensitivity C reactive protein; BMI: body mass index; WC: waist circumference.
Chi-square test, p-value=0.0069, hs-CRP: high sensitivity C reactive protein.
HPB: high blood pressure; hs-CRP: high sensitivity C reactive protein; TC: total cholesterol; TG: triglycerides; HDL-c: high density lipoprotein; LDL-c: low density lipoprotein; Castelli Index I: TC/HDL-c; Castelli Index II: LDL-c/HDL-c; Estimative of the size of LDL-c particle: TG/HDL-c; BMI: body mass index; WC: waist circumference.
*Significant; p<0.05