Group B Streptococcus: An Unusual Cause for Urinary Tract Infection
Bichitrananda Swain1, Anindita Rakshit2, Kundan Kumar Sahu3, Nalinee Sahoo4, Sarita Otta5
1 Professor, Department of Microbiology, IMS and SUM Hospital, Bhubaneswar, Odisha, India.
2 Demonstrator, Department of Microbiology, Calcutta School of Tropical Medicine, Kolkota, West Bengal, India.
3 Associate Professor, Department of Microbiology, IMS and SUM Hospital, Bhubaneswar, Odisha, India.
4 Postgraduate Student, Department of Microbiology, IMS and SUM Hospital, Bhubaneswar, Odisha, India.
5 Assistant Professor, Department of Microbiology, IMS and SUM Hospital, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sarita Otta, 1/5, Kanchanjunga Enclaves, Chandrasekharpur, Bhubaneswar-751016, Odisha, India.
E-mail: saritaotta@gmail.com
Diabetes mellitus, Group B Streptococci, VITEK-2
Dear Editor,
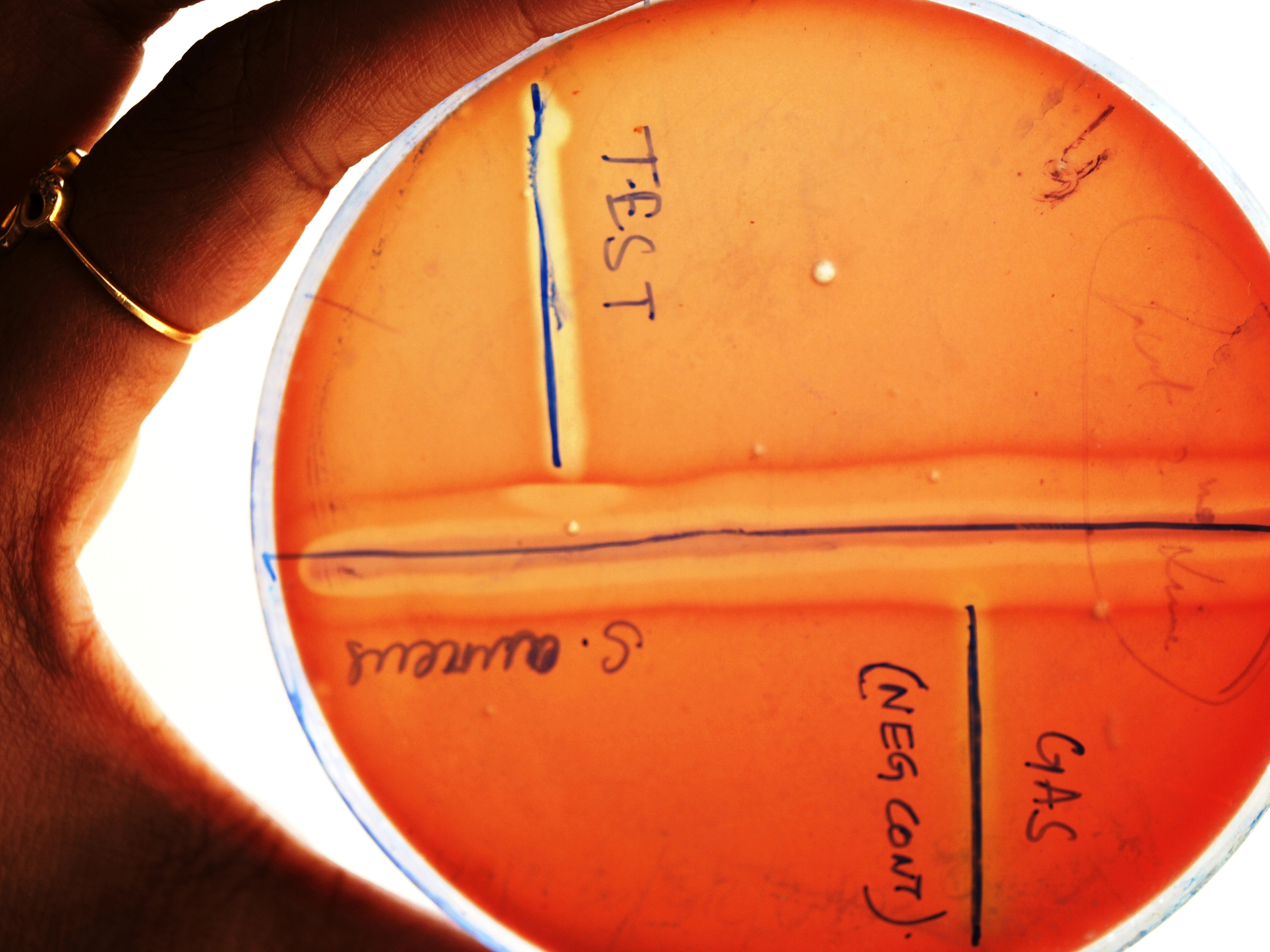
Group B Streptococcus (GBS), the cervicovaginal colonizer, is a common cause of neonatal sepsis, pneumonia, meningitis, bacteraemia, skin and soft tissue infections, chorioamnionitis, endometritis, osteomyelitis etc., but its association with Urinary Tract Infections (UTIs) is rare [1]. A 58-year-old diabetic male presented to the outpatient department in our hospital with mild fever and frequent micturition. After a thorough clinical examination, laboratory tests were advised which denoted a higher leucocyte count with neutrophilia (TLC-15000/mm3, N-82%) and higher blood sugar levels (FBS-170 mg/dL and PPBS-236 mg/dL). Other tests including those for malaria and enteric fever were negative and renal function tests and liver function tests were within normal limits. He was seronegative for HIV and non reactive for Venereal Disease Research Laboratory (VDRL) test. With a mid stream urine sample, wet mount preparation showed plenty of pus cells with numerous cocci, mostly arranged in chains. On culture after overnight aerobic incubation at 37°C, significant number of fine, opaque colonies was grown on Cystine Lactose Electrolyte Deficient (CLED) agar plate. These were Gram-positive cocci in chains and showed negative reactions for catalase and bile esculin. The organism was beta haemolytic, bacitracin resistant [Table/Fig-1] and Christie-Atkins-Munch-Petersen (CAMP) positive [Table/Fig-2] on sheep blood agar. Thus, the isolate provisionally identified as Streptococcus agalactiae was further substantiated by VITEK-2 system (bioMérieux) using Gram-Positive (GP) identification card with 98% probability. Antimicrobial susceptibility test was performed by modified Kirby-Bauer disk diffusion method as per CLSI guidelines [2] and the patient became asymptomatic with proper antibiotic treatment. Repeat urine culture after seven days did not show any growth of this organism.
Bacitracin resistant beta haemolytic colonies on sheep blood agar.

Isolate showing positive CAMP test.
UTI is the second most common infectious disease in human, common in females and is mostly caused by Gram-negative bacilli [3]. In males, it is rarely attributed to Streptococcus agalactiae. Despite the high prevalence of GBS in the urethra, especially in individuals presenting with Sexually Transmitted Disease (STD), it is a rare cause of UTI [4,5]. GBS is mostly associated with postpartum infection that results from the vertical transmission of bacteria due to maternal cervicovaginal colonization. Group B Streptococcal infection in healthy adults is extremely uncommon, except in young and middle aged women, and is mostly associated with diabetes mellitus and chronic renal failure [6]. Diabetes, in our case, may be the predisposing factor. The increased frequency of UTIs in these patients may be due to the presence of glycosuria, neutrophil dysfunction or increased adherence of the bacteria to uroepithelial cell [7]. As GBS colonizes the vagina and is highly prevalent in urethra of STD patients, so one must keep it in mind as it may be a source of infection for the urinary tract, especially in sexually active diabetic individuals. A prompt diagnosis will alleviate the development of further complications.
[1]. Chaiwarith R, Jullaket W, Bunchoo M, Nuntachit N, Sirisanthana T, Supparatpinyo K, Streptococcus agalactiae in adults at Chiang Mai University Hospital: a retrospective studyBMC Inf Dis 2011 11:149 [Google Scholar]
[2]. CLSI. Performance Standards for Antimicrobial Susceptibility Testing: Twenty Sixth Informational Supplement. CLSI document M100-S26. Wayne, PA: Clinical and Laboratory Standards Institute; 2016 [Google Scholar]
[3]. Ronald A, The etiology of urinary tract infection: traditional and emerging pathogensAm J Med 2002 113(1A):14S-19S. [Google Scholar]
[4]. Christensen KK, Christensen P, Flamholc I, Ripa T, Frequencies of streptococci of groups A, B, C, D and G in urethra and cervix swab specimens from patients with suspected gonococcal infectionActa Pathologica Et Microbiologica Scandinavica 1974 Section B:82-470. [Google Scholar]
[5]. Walling J, Forsgren A, Group B streptococci in venereal disease clinic patientsBr J Venereal Dis 1975 51:401 [Google Scholar]
[6]. Munoz P, Coque T, Creixems MR, Bernaldo de Quiros JC, Moreno S, Bouza E, Group B Streptococcus: a cause of urinary tract infection in non pregnant adultsClin Infect Dis 1992 14:492-96. [Google Scholar]
[7]. Hakeem L, Bhattacharyya D, Lafong C, Janjua K, Serhan J, Campbell I, Diversity and complexity of urinary tract infection in diabetes mellitusBr J Diabetes Vasc Dis 2009 9:119-25. [Google Scholar]