The clinical success of resin composite restoration depends on various parameters like depth of cure, degree of polymerization, polymerization shrinkage, linear coefficient of thermal expansion, modulus of elasticity, wear resistance, C-factor etc. Depth of cure is defined as the thickness of a light cured resin that can be converted from a monomer to a polymer when exposed to a light source under a specific set of conditions [1]. Degree of conversion is defined as the percentage of carbon-carbon double bonds (- C = C -) converted to single bonds (- C - C -) to form a polymeric resin [1].
When light is transmitted through the composite resin, there is a gradual decrease in degree of conversion as the distance increases from the irradiated surface which leads to elution of monomer causing failure of the restoration [2-5]. Increment thickness of 2 mm is the gold standard for composite placement and curing [6,7]. It is highly technique sensitive and time consuming in cases of larger posterior restorations or during core build up procedures, where composite restorations are indicated. To address these problems, various manufactures have recently introduced new type of resins, so called “bulk fill” materials which claim to cure a maximum increment thickness of 4 mm [8-11].
There are some relevant methods to determine the degree of monomer to polymer conversion of composite resin specimens like FTIR spectroscopy, Laser Raman spectroscopy, Electron Spin Resonance (ESR), Infrared Spectroscopy (IR), Dynamic Mechanical Thermal Analysis (DMTA), Attenuated Total Reflection (ATR) etc., [12]. Of these, the most reliable method to determine the extent of monomer conversion is FTIR, which can detect the stretching vibrations of carbon-carbon double bonds involved in polymerization directly before and after curing of the composite resins [13-15]. The method typically utilizes the height ratio of the peaks corresponding to aliphatic and aromatic double bonds to determine the degree of conversion. A method for finding the curing of the maximal increment thickness of resin composites has been introduced by the International Organization for Standardization (ISO) in the second edition of ISO 4049. In 1988, it was officially denominated as “ISO 4049, Depth of Cure” [16]. According to this method, a teflon mold was used to create the composite specimen. The specimens were removed from the mold after light curing and uncured resin was scraped off with a plastic instrument. The length was measured and divided by 2 as per ISO 4049 method [17].
Hence, the aim of this study was to comparatively evaluate the depth of cure of two different bulk fill composite resins (Surefil SDR bulk fill flowable and Filtek bulk fill flowable composite) by ISO 4049 method and to evaluate the degree of conversion of the same composite resins with FTIR spectroscopy method. The tested null hypothesis was that there is no difference in depth of cure and degree of conversion between the two bulk fill flowable composite materials.
Materials and Methods
This in vitro study was conducted in Department of Conservative Dentistry and Endodontics at Best Dental Science College and Dental Hospital, Madurai, Tamil Nadu, India, after getting approval of the Ethical committee. Based on the figures of bottom hardness reported in previous study [18], the sample size for this study was calculated as 10 samples per group for a confidence level of 95% and a power of 95%.
Hence, composite resin specimens (n=10) per group were prepared with both bulk fill flowable composites, Surefil SDR bulk fill flowable composite (Dentsply Caulk, Milford, DE, USA) designated as Group A and Filtek bulk fill flowable composite (3M ESPE, St.Paul, MN, USA) designated as Group B [Table/Fig-1,2].
Group A and Group B Surefil SDR bulk fill flowable composite and Filtek Bulk fill flowable fill flowable composite.

Composition of Surefil SDR and Filtek bulk fill flowable composites.
| Group | Composite resin | Resin | Filler | Photoinitiator | Lot number | Manufacturer |
|---|
| Group A | 1. Surefil SDR bulk fill flowable composite | Urethane di- methacrylate resin (UDMA) | Barium and strontium alumino fluoro silicate glasses | Camphoroquinone | 1406000399 | Dentsply |
| Group B | 2. Filtek bulk fill flowable composite | BisGMA, BisEMA, Procry-lat, UDMA | Zirconia or silica, ytterbium trifluoride | Camphoroquinone | N 575416 | 3M ESPE |
Estimation of Depth of Cure
Depth of cure was determined according to “ISO 4049; Depth of Cure” method, using re-usable teflon mold of 8 mm length and 4 mm diameter. The mold was placed on a glass slide covered by a mylar strip and then the teflon mold was filled in bulk with one of the bulk fill flowable composites. The top side of the mold was covered with a mylar strip and light cured for 20 seconds, keeping the light tip centered and in contact with the material (LEDition, Ivoclar Vivadent AG, Schaan, Liechtenstein, operating at 7.5 VDC, 3W LED, with a wavelength range of 430-490 nm and typical light output of 600 mW/cm2).
After light curing, the cylindrical specimens were pushed out of the teflon mold and the uncured resin composite material was removed or scrapped off with a plastic spatula. This technique gave specimens of different sizes. The absolute length of the cylindrical specimen of the cured resin composite was then measured with a digital caliper of ±0.01 mm accuracy [Table/Fig-3]. The absolute length was divided by two and the value was recorded as ‘Depth of Cure’.
Measurement of cured resin samples with digital caliper.

The same procedure was repeated for estimating the depth of cure for all the specimens. Hence, the procedure was done ten times for each group to obtain ten specimens per group.
Estimation of Degree of Conversion
The degree of conversion of both bulk fill flowable composites (Surefil SDR and Filtek flowable bulk fill composites) was estimated using FTIR method.
After determining the depth of cure of resin composite specimens, each specimen in Group A and Group B, which were of different sizes were divided into two equal halves. They were referred as coronal half and pulpal half, designated as Group A1, A2 and Group B1, B2 respectively. Hence, 20 specimens per each group and total of 40 resin composite specimens were made to estimate the degree of monomer to polymer conversion individually in coronal half (Group A1 and B1) and pulpal half (Group A2 and Group B2).
All specimens were pulverized and mixed with potassium bromide (KBr) in 1:10 ratio as it is 100% transparent with wide spectral range. The specimens were then pressed in hydraulic pellet maker (Pixie hydraulic pellet press, Pike technologies, Madison, USA) which is thin, transparent and 13 mm in diameter. The prepared pellets were placed into a cell holder in spectrophotometer and the readings were made [Table/Fig-4].
Prepared pellets of resin samples to be examined under spectrometer.
Degree of Conversion is calculated by the formula [19],

H2 → peak height absorbance intensity of carbon double bond peak aliphatic
H1 → peak height absorbance intensity of carbon double bond peak aromatic.
Statistical Analysis
Statistical analysis was performed by Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 19.0 for Windows). Using this software mean and standard deviation were calculated for quantitative variables. Student’s unpaired t-test was used to test the significance of difference between the two groups. A p-value of less than 0.05 is taken to denote the significant relationship.
Results
Depth of Cure
The mean depth of cure of Group A (Surefil SDR bulk fill flowable composites) was 3.89 mm (±0.103) and for Group B (Filtek bulk fill flowable composites) was 3.54 mm (±0.129) [Table/Fig-5].
Comparison of mean depth of cure values of both bulk fill flowable composites (Student’s unpaired t-test).
| Group | Depth of cure (mm) | p-value |
|---|
| Mean | ± S.D. |
|---|
| Group A | 3.89 | 0.103 | <0.001* |
| Group B | 3.54 | 0.129 |
*Significant (p<0.05)
Statistical analysis revealed significant difference (p<0.05) in the depth of cure between the two bulk fill flowable composites with Group A higher than Group B.
Degree of Conversion
The degree of conversion percentage for four groups were, Group A1=78.51 (±47.8), Group A2=31.9 (±22.4), Group B1=39.8 (±5.2), Group B2=37.4 (±6.4) [Table/Fig-6]; and it was higher for Group A1.
Comparison of degree of conversion percentage of coronal and pulpal half of both bulk fill flowable composites (Student’s unpaired t-test).
| Group | Mean | ± S.D. | p-value |
|---|
| Group A1 | 78.51 | 47.8 | 0.0203* |
| Group B1 | 39.8 | 5.2 |
| Group A2 | 31.9 | 22.4 | 0.4614** |
| Group B2 | 37.4 | 6.4 |
*Significant (p<0.05)
** Non Significant (p>0.05)
Statistical analysis revealed significant difference (p<0.05) in degree of conversion between the two bulk fill flowable composites with Group A1 (coronal half of Surefil SDR flow) higher than Group B1 (coronal half of Filtek bulk fill flowable composite). [Table/Fig-7,8]. On the other hand, there was no statistically significant difference (p>0.05) between Group A2 (pulpal half of Surefil SDR flow) and Group B2 (pulpal half of Filtek bulk fill flowable composite). Hence, null hypothesis was rejected in case of depth of cure and coronal half of degree of conversion of both the bulk fill flowable composites.
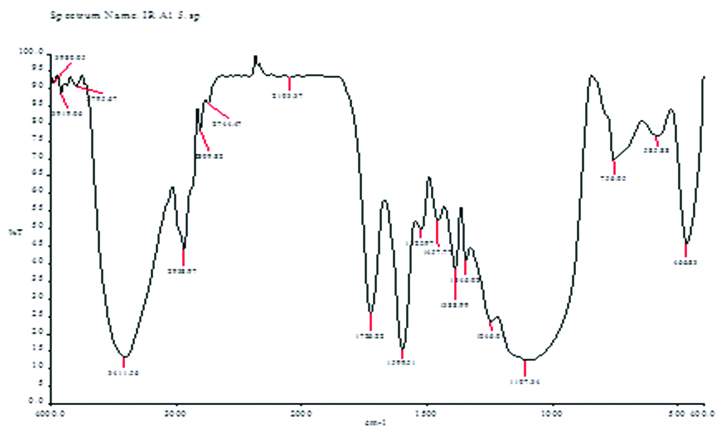
Graphical representation of FTIR for Surefil SDR flow.
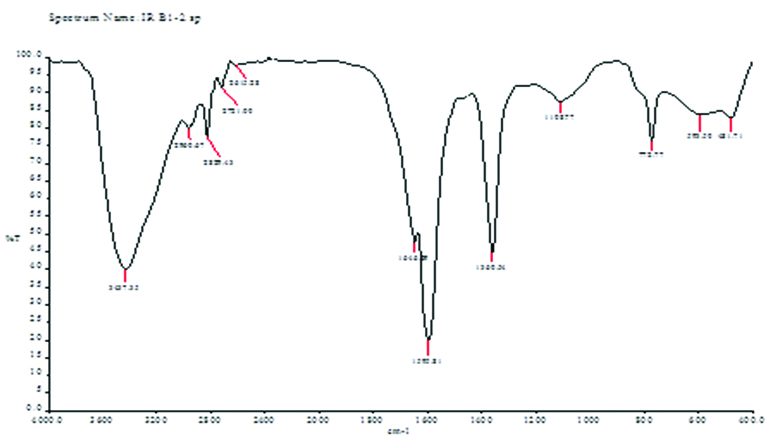
Graphical representation of FTIR for Filtek bulk fill flow.
Discussion
Traditional composite resin restorative materials may result in reduced polymerization in the more apical aspects of a restoration during bulk placement. According to the literature, this may be due to the inability of the light from the light-curing unit to penetrate these regions [20,21].
Recent developments in restorative and flowable composite resins have resulted in a greater total depth of cure up to 4 mm [22,23]. Greater translucency, increased photoinitiator content, or an additional photoinitiator type may be the factors responsible for improved depth of cure of these resin composite materials [24]. Due to low-viscosity and easy handling properties of these flowable composites, they are particularly beneficial in restoring cavities which are difficult to access, forming layered structures reducing air entrapment and finally used as liners due to their higher flexibility [25].
The depth of polymerization is considered vital to make sure that, the clinical problems do not arise due to partially polymerized material in the base of the cavity [26]. Unlike other indirect techniques, which was based on measuring changes in the mechanical performance of the material to estimate relative degree of conversion, FTIR spectroscopy allows the direct detection of the amount of unreacted C = C in the resin matrix [27,28].
FTIR spectroscopy is a powerful analytical technique which has been utilized as a quantitative measure for the identification and monitoring setting reactions and polymerization of a broad range of dental materials [29]. Because the polymerized specimens need to pulverized, [17,30], the depth of cure was estimated first by a method called ISO 4049 method.
In the present study, the depth of cure values using the scraping method [18] were greater for both the tested bulk fill flowable composite materials, at the same time, the mean depth of cure of Surefil SDR flow was statistically higher than Filtek bulk fill flowable composites. These results were in accordance to study done by Flury S et al., who found that ISO 4049 method showed highest depth of cure values for bulk fill composites [16].
It has been demonstrated that filler size and content in dental composites may reduce light penetration and is directly related to depth of cure [31,32]. The presence of pigments in shaded composite materials should also have an effect on depth of cure because pigments are opaque particles that will limit light penetration and reduce the degree of polymerization at greater depths within a cavity preparation [18].
The highest degree of conversion was observed to be higher on coronal half of Surefil SDR bulk fill flowable composite than in coronal half of Filtek bulk fill flowable composite. This might be due to the fact that SDR contains a patented modified UDMA, which is claimed to reduce polymerization shrinkage, shrinkage stress and improve degree of conversion [33]. Moreover, the manufactures claims that low polymerization shrinkage for Surefil SDR flow shall result from addition of the “polymerization modulator” a chemical moiety in the resin back bone, increasing flexibility and hence, relaxing the polymerized network without affecting degree of conversion. The unique combination of high glass filler loading with SDR resin provides high depth of cure and proper rheology for self leveling characteristic for optimum adaptation and marginal integrity. This was confirmed by other studies showing significant lower polymerization stress values for Surefil SDR flow [34].
Similarly, Filtek bulk fill flow composites contain a proprietary monomer analogous to Bis-GMA and patented as Procrylat resin. It was also found that these modified monomers have altered polymerization kinetics and delayed the monomer conversion [35] which could explain better degree of conversion for this material.
Limitation
Limitations of this study were non-inclusion of conventional composites for better comparison and the number of samples should have been increased.
In future, a better designed study closer to clinical scenario, evaluation of depth of cure and degree of conversion with other methods, usage of higher intensity and other light sources and in cavity designs with various configuration factor (C-factor) is required.
Conclusion
Within the limitations of the study, Surefil SDR bulk fill resin has better depth of cure and degree of conversion in the coronal half when compared to Filtek bulk fill composite. Further studies are required to evaluate the other physical and mechanical properties of both the bulk fill flowable composite resins.