Composite restoration has now become an essential part of everyday dental practice and with the improvement in dental adhesive systems; there has been an increase in patient’s demand for esthetics and preservation of tooth structure [1]. However, the major shortcoming of the dental composite materials is the polymerization shrinkage and the stress associated with it [2].
Polymerization shrinkage produces contraction stresses in the resin composite restoration. As the elastic modulus of the composite increases during curing, an internal stress and deformation is induced in the surrounding tooth structure [3]. This stress is exhibited as bond failure, cuspal deflection, enamel microcracking, pulpal irritation, secondary caries and postoperative sensitivity, which in turn can lead to restoration failure requiring rerestoration [4].
Cuspal deflection is defined as a biomechanical phenomenon which leads to linear movement of the cusp tips of the tooth as a result of interactions between the polymerization shrinkage stress of the composite and the compliance of the cavity wall of the tooth [5]. About 10 μm–45 μm of cusp deflection has been reported during composite restoration, varying according to the measurement method, tooth type, and cavity size [6].
The extent of polymerization shrinkage stress can be influenced by the cavity configuration (C-factor, bonded surface/unbonded free surface) [7]. As the C-factor increases, the compensation for polymerization shrinkage by the flow of composite decreases, and thus, the polymerization stress at the bonded surface increases [8,9].
New material developments such as hybrid resin composites, fine hybrid resin composites, nanohybrid resin composites, purely nano-filled resin composites, and silorane-based composites have been introduced during the last decade, but the clinical problems still persist [10]. The most recent attempt to reduce polymerization shrinkage is the development of SonicFillTM system that enables sonic activation of the composite, significantly reducing its viscosity to rapidly fill the cavity [11]. Upon deactivation of the sonic energy, the viscosity of the composite increases and allows easy and accurate sculpting morphology of the composite. Thus, combines the advantages of a flowable composite with universal composites [12].
Hence, this study was done to evaluate the cuspal deflection of premolars restored with different composite materials using different insertion techniques.
Materials and Methods
The present in vitro study was conducted in the Department of Conservative Dentistry and Endodontics, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India.
Forty human maxillary first premolar teeth having approximately similar crown size and regular occlusal anatomy, extracted for orthodontic purposes and free from caries, cracks or defects were selected for this study.
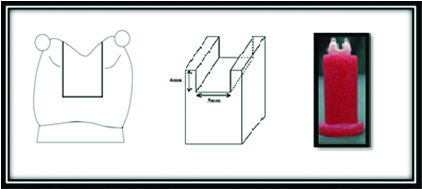
An approximately 1 mm diameter glass bead was fixed to each cusp as reference point for intercuspal distance measurements. Each tooth was mounted vertically using molten modelling wax in preformed moulds with dimensions simulating the base of the micrometer gauge [Table/Fig-1].
Glass beads placed as reference point;

Cavity Preparation
Each tooth was subjected to preparation of a large MOD cavity, with the parallel walls using a diamond flat-ended fissure bur (SSWhite-SSW SF 51C) in a high speed handpiece with water coolant. A uniform cavity design with standardized dimensions was selected for the tooth preparation having width of two third the intercuspal distance (3 mm) and a depth of 4 mm gauged from the tip of the buccal cusp to the pulpal floor and prepared. The stylized, slot MOD preparation, prepared without proximal boxes, was utilized in order to minimize preparation variation. The cavity width and depth were same at occlusal isthmus and proximal part. All gingival walls were located above the cementoenamel junction at the cervical aspect of the proximal part [Table/Fig-2].
Showing stylized cavity design and measurements.
The samples were divided into four groups (n=10):
Group I (n=10) – prepared teeth were restored using Tetric N-Ceram by bulk fill technique of restoration.
Group II (n=10) – prepared teeth were restored using Tetric N-Ceram by horizontal incremental technique of restoration.
Group III (n=10)– prepared teeth were restored using Tetric N-Ceram by modified tangential technique of restoration.
Group IV (n=10) – prepared teeth were restored using SonicFillTM as a bulk fill restorative material.
Tooth Restoration
All the samples were subjected to uniform etching and bonding procedure.
Each tooth was thoroughly dried before the restorative procedure. The etching gel (N- Etch Ivoclar, Vivadent marketing, India) was applied on the prepared tooth for 15 seconds. Each tooth was then rinsed for 10 seconds and blot dried. Immediately after blotting, bonding agent (Tetric N- Bond IvoclarVivadent marketing, India) was applied to the etched surface for 15 seconds with a slow agitation of the applicator. Gentle air pressure was applied for 5 seconds to evaporate the solvents and was then light cured for 20 seconds. In all cases, the matrix band was placed without using a retainer in order to avoid any tension on the cusps.
Restorative procedure and the photopolymerization scheme followed for different groups are as mentioned in [Table/Fig-3].
Restorative procedure and the photopolymerization scheme followed for different groups.
| Group | Restorative technique | Photopolymerization scheme |
|---|
| Group I | Bulk fill using Tetric N Ceram | 60 seconds |
| Group II | Horizontal incremental pattern : each increment measuring 1 mm+1.5 mm+1.5 mm | 20 seconds + 20 seconds +20 seconds |
| Group III | Modified tangential increments : 1 mm horizontal increment + 2 tangential increments | 20 seconds + 20 seconds + 20 seconds |
| Group IV | Bulk fill using SonicFillTM as a restorative material | 60 seconds |
Sample Measurement
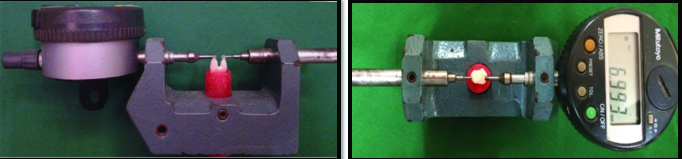
The models were placed into the customized assembly such that the two prongs touched the buccal and lingual reference points of the mounted tooth throughout the test readily detecting any linear change in the measurement onto the attached digital micrometer (Mitutoyo, Kawasaki, Japan). The intercuspal distance of unaltered tooth i.e., ‘the initial intercuspal distance’ between the reference points was first measured. Consecutive measurement of intercuspal distance after cavity preparation for each tooth was recorded as ‘intermediate distance’. The distance between the glass beads was measured continuously throughout the restorative placement procedure at room temperature for 15 minutes after tooth restoration until the deflection became a continuous plateau and was recorded as the ‘final distance’ [Table/Fig-4]. The difference between the final and the initial measurements gave us the measurement of the cuspal deflection. The stability of the setting was essential since any slight motion was easily detected by the digital micrometer [Table/Fig-5].
Showing restoration of the prepared tooth using SonicFill as a restorative material.

Showing adjustment and measurement of the tooth sample in the customized digital micrometer assembly.
Statistical Analysis
Mean cuspal deflection for each group was calculated and One-Way ANOVA test was applied for the analysis of significant difference between the groups followed by Unpaired t-test analysis.
A p-value less than 0.05 were considered statistically significant.
Results
[Table/Fig-6] represents the initial and the final mean intercuspal distance of the four groups and the mean cuspal deflection that occurred in each group.
Descriptive table showing initial readings, final readings and cuspal deflection (initial readings – final readings) in different groups.
| Groups | Initial readingsMean ± S.D | Final readingsMean ± S.D | Difference(Initial readings - final readings)Mean ± S.D | F value (ratio of mean squares) | p-value |
|---|
| Group I | 7.784 ± 0.466 | 7.739 ± 0.459 | 0.045 ± 0.018 | 15.209 | <0.001 [highly significant]. |
| Group II | 7.874 ± 0.537 | 7.845 ± 0.540 | 0.029 ± 0.009 |
| Group III | 7.639 ± 0.357 | 7.620 ± 0.356 | 0.018 ± 0.005 |
| Group IV | 7.857 ± 0.558 | 7.840 ± 0.558 | 0.017 ± 0.004 |
*p<0.05 consider statistically significant.
One-way ANOVA test was applied for the analysis of significant difference between the groups.
ANOVA test reveals that the variance of difference (initial readings – final readings) in different groups was statistically highly significant (p<0.001).
All four groups were associated with a significant cuspal deflection. The comparison between the different groups [Table/Fig-6,7], revealed that the mean cuspal deflection was highest in group I (bulk filling using Tetric N ceram) and was lowest in Group IV (bulk filling using SonicFillTM). Group II and Group III were having an intermediate mean cuspal deflection with Group III (modified tangential incremental filling using Tetric N ceram) showing lesser mean cuspal deflection when compared to Group II (horizontal incremental filling using Tetric N ceram).
Unpaired t-test applied for the comparison of cuspal deflection in between Group I, Group II, Group III and Group IV.
| Groups | Difference(Initial readings – final readings)Mean±S.D | Difference(Initial readings – final readings)Mean±S.D | t-value | p-value |
|---|
| I and II | 0.045±0.018 | 0.029±0.009 | 2.4786 | 0.0233 (significant) |
| I and III | 0.045±0.018 | 0.018±0.005 | 4.3966 | 0.0003 (significant) |
| I and IV | 0.045±0.018 | 0.017±0.004 | 4.6805 | 0.0002 (significant) |
| II and III | 0.029±0.009 | 0.018±0.005 | 3.1366 | 0.0057 (significant) |
| II and IV | 0.029±0.009 | 0.017±0.004 | 3.6807 | 0.0017 (significant) |
| III and IV | 0.018±0.005 | 0.017±0.004 | 0.7157 | 0.4833 |
*p<0.05 consider statistically significant
There was a highly significant difference of mean cuspal deflection among all the groups except for Group III and Group IV where p-value >0.05.
Discussion
Cusp deflection is a common biomechanical occurrence observed in teeth restored with composites and is the result of interactions between the polymerization shrinkage stress of the composite and the elastic deformation of the cavity wall. The two factors that could be involved in cusp deflection are the bonding system and the composite itself [13,14].
Hood JA reported that the remaining cusp after cavity preparation acts as cantilever beams under occlusal load. According to mechanical principles, the cusp deflection is proportional to the cantilever length cubed, and to the inverse of the thickness of the cantilever cusp cubed [15]:

The polymerization shrinkage during composite curing is the main force inducing cusp deflection. The cuspal deformation depends on the amount of polymerization shrinkage, the total amount of composite in a cavity, and the elastic modulus of the cured composite [15,16]. The polymerization shrinkage force is also affected by the flow of composite and the C-factor [17]. It is very difficult to establish a formula estimating the cusp deflection from so many variables; therefore, it is practical to measure deflection experimentally.
The results of this study have shown that there is an inward deflection of the cusps for all the experimental groups evaluated. The proprietary low-shrinkage SonicFillTM material used in this study showed significantly lower cuspal flexure, in accordance with the manufacturer’s claim [18-20].
The incremental insertion technique has been documented to decrease the polymerization shrinkage by reducing the bulk of composite cured with each layer [21,22]. Decreasing the C-factor has also been suggested to reduce the curing shrinkage by permitting unobstructed “flow” of the material in the unbonded surface layer [3].

As the C-factor increases, the compensation for polymerization shrinkage by the flow of composite decreases, and thus, the polymerization stress at the bonded surface increases [17]. In a study conducted by Kim ME and Park SH, it was concluded that the incremental filling techniques reduced the amount of cuspal deflection when compared to bulkfill technique [21]. In the current study, the overall amount of cusp deflection of the incrementally filled groups (Group II and Group III) was significantly lesser than that of bulk filled group (Group I) (p<0.05) hence, supporting the previous studies [3,6].
The differences between horizontal and tangential incremental techniques (Group II and Group III) were apparent, proving the increased efficacy of tangential increments. This could be explained by an increased C-factor, resulting in greater cusp deflection in Group II.
According to the most of the studies done till now, an incremental layering technique has been the standard procedure in direct posterior composite restorations to reduce polymerization shrinkage stress and achieve adequate curing [9,23], yet, recent advances in composite technology for posterior restoration have been targeted as alternatives to the incremental layering technique [24].
SonicFillTM is a composite restoration where the viscosity of the composite is dramatically reduced, up to 87%, due to the special rheological modifiers that react to sonic activation of the material delivered through the SonicFill™ hand piece during its placement. Thus, increasing its flow and enabling rapid filling of the cavity. Precise adaptation to the cavity walls make the frequency and size of critical voids located at the margin and along line angles of the cavity less pronounced compared to the conventional putty-like composites [12]. When the sonic energy is stopped, the composite returns to a more viscous, non-slumping state that is perfect for carving and contouring [25].
Generally, increasing the filler load in the resin matrix results in reduction of overall shrinkage of the composite due to the reduced availability of the monomer for the curing reaction. But it may also result in increase in the viscosity of a material, thus posing difficulty in placement and more chances of gap formation [24]. SonicFillTM consist of a special composite formulation, which contains about 83.5% of fillers by weight, which is significantly higher when compared to the filler content of Tetric N Ceram (78%wt) [19,26]. Difference in the cuspal deflection among the two different bulk fill materials used in this study could be attributed to the difference in the filler loading.
It has also been documented that an increase in filler volume content results in an increase in the stiffness of the material with high modulus of elasticity thereby increasing the cuspal deflection, which contradicts with the results of the current study [27,28]. This can be due to the bulk filling of the SonicFillTM. There is relaxation of polymer chains with the decrease in polymerizing light intensity which decreases with the decrease in the distance of the light curing tip to the restoration material. Hence, less contraction stress is produced in the deepest portions of the cavity when bulk filled with SonicFillTM permitting a delay in attainment of the gel point, thus, reducing polymerization stresses [29]. Secondly, proper adaptation of the material to cavity walls without void formation reduces the contraction, thus, reducing the possibility of the composite pulling away from the tooth surface during polymerization subsequently lowering the cuspal deflection [12,30].
In the current study, SonicFillTM (Group IV) showed the least cuspal deflection among the four groups but the difference between the cuspal deflection among Group III and Group IV was not statistically significant. Thus, it can be concluded that SonicFillTM has a comparable cuspal deflection to the modified tangential technique of incremental filling. Even though, incremental technique has been recommended for sufficient light penetration, its drawbacks include the likelihood of trapping voids or contamination between the layers and the increased time required to place the restoration [31,32].
Cuspal flexure during curing of resin composite restorative materials can cause significant problems in adhesive dentistry, such as debonding of the restoration- tooth interface, microleakage, marginal staining, postoperative sensitivity and microcracks within the tooth structure.
Limitation
Although, the research has reached its aim, there were some unavoidable limitations due to less ideal conditions such as tooth hydration condition; unrestrained test condition-absence of occlusal load, which may not necessarily be expected in the actual practice. It is obvious that dentists have always been looking for a fast and reliable filling technique allowing the reduction of layers, effort and time; therefore, the time-consuming incremental layering technique can be substituted with the bulk fill technique using SonicFillTM as a bulk fill material. However, further researches evaluating the properties of the material and its clinical implications are recommended.
Conclusion
All the groups studied caused measurable cuspal deflection. In general, bulkfill restoration with conventional composite showed significantly highest cusp deflection. There were no significant differences in cuspal deflection among SonicFillTM and modified tangential incremental insertion techniques.
*p<0.05 consider statistically significant.
One-way ANOVA test was applied for the analysis of significant difference between the groups.
ANOVA test reveals that the variance of difference (initial readings – final readings) in different groups was statistically highly significant (p<0.001).
*p<0.05 consider statistically significant