Crossed Fused Ectopic Kidney: A Case Report
Rohit Bhattar1, Anuradha Maheshwari2, Vinay Tomar3, Sher Singh Yadav4
1 Mch Urology Resident, Department of Urology and Renal Transplantation, Sawai Man Singh Medical College, Jaipur, Rajasthan, India.
2 Clinical Associate, Department of Anaesthesia, Eternal Hospital, Jaipur, Rajasthan, India.
3 Professor and Head, Department of Urology and Renal Transplantation, Sawai Man Singh Medical College, Jaipur, Rajasthan, India.
4 Professor and Head, Department of Urology and Renal Transplantation, Sawai Man Singh Medical College, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rohit Bhattar, Mch Urology Resident, Department of Urology, Sawai Man Singh Medical College, Jaipur-302004, Rajasthan, India.
E-mail: bhattarrohit@gmail.com
Crossed fused ectopic kidney is an unusual congenital malformation of the urinary tract. This condition is usually identified in the autopsy specimen rather than in general clinical scenario. In this condition, both kidneys are located on one side of the midline and are fused with each other. This condition is generally asymptomatic and usually diagnosed as incidental finding. We came across a case of crossed fused left to right ectopia with inferior infusion with nephroptosis. Generally, in cases of crossed fused renal ectopia, one kidney is lower than the other one but in our report, both kidneys were present at the same level. Initially it was thought as cake kidney, but on careful inspection diagnosis of crossed fused left to right ectopia with inferior infusion was made. During workup of abdominal pain, this finding was detected with no gross abnormality except for a tiny calculus. After detailed discussion with the patient, regular follow up was done without any active intervention and during that period he remained clinically and radiologically stable. So in these conditions active intervention is not always mandatory and patient may remain asymptomatic without any intervention.
Cake kidney, Inferior fusion, Left to right ectopia
Case Report
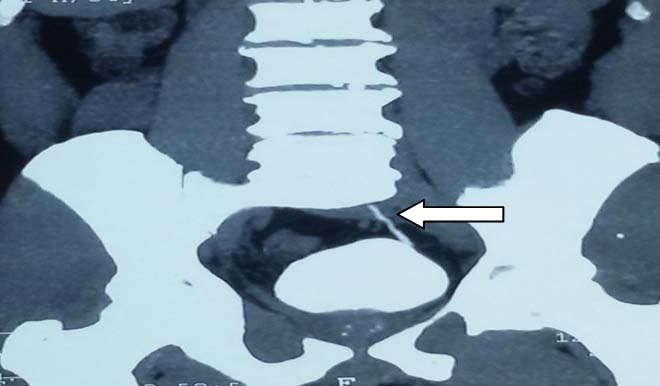
A 47-year-old male patient presented with history of intermittent pain in right lumbar region for 12 months. History, general physical examination and routine laboratory investigations were in the normal range. His blood pressure was within normal range and cardiovascular, chest, skeletal system and genital examination did not reveal any anomaly. Abdominal ultrasonography showed ‘empty’ renal fossae bilaterally and a large fused kidney in the right iliac fossa. After that Contrast Enhanced Computed Tomography (CECT) abdomen and subsequently computed tomography renal angiography was done which showed that both kidneys were lying at the right paravertebral region at L4-L5 level i.e., at the same level. Inferior pole and mid region of both kidneys were fused and upper pole was free with anteriorly directed bilateral renal pelvices [Table/Fig-1].
CECT abdomen showing fused kidney with bilateral renal fossa empty (coronal images), (straight arrow showing right kidney and curved arrow showing embryologically left kidney).

Ureter from right moiety draining into right side and ureter from left moiety crosses the midline and drain into the left side of urinary bladder [Table/Fig-2]. There was an accessory right renal artery arising from right common iliac artery and a 3 mm non obstructive calculus at upper calyx of right kidney with normal vascular supply to left moiety [Table/Fig-3].
CECT abdomen showing the left ureter entering the bladder orthotopically (coronal images).
CECT renal angiography showing renal vessels (coronal images).

Initially, this was thought as a cake kidney, as both kidneys were present at the same level and major portion of both kidneys were fused but on vigilant inspection final diagnosis was made of left to right ectopia with inferior fusion and nephroptosis. Patient was counselled and managed conservatively (analgesics as and when needed only). After three years, CECT abdomen was repeated and similar findings were noted. Patient did well without any active complaints during this period.
Discussion
Crossed fused renal ectopia is one of the rare congenital abnormalities. It is mostly seen in autopsy but can also be present in clinical practice in various forms. The prevalence of the crossed renal ectopia with fusion was estimated to be 1 in 1000 live births [1] and simple ectopic kidneys can be located from the pelvis to the thoracic cavity, but not the crossed fused ectopic kidneys which are generally located in abdomen at a lower level or in pelvic cavity. The incidence at autopsy can vary from 1 in 2000 to 1 in 7500 [2, 3]. This is more common in males and left to right ectopia with inferior fusion is referred as the most common variety. In our case, it was presented like a cake kidney but with precise evaluation, final diagnosis of crossed fused left to right inferior ectopia was made because in cake kidney upper pole of both kidneys are also commonly used which were not seen in this case [3]. Understandings of these kinds of anomalies are important especially if surgery has to be planned. Aim of our report is to share our experience and focus on unusual presentation of crossed fused inferior left to right ectopic kidney with nephroptosis. In cases of crossed renal ectopia, fusion variety is most common and present in 90% of cases. It can be present in the form of unilateral fused kidney with either Inferior Category (A) or Superior ectopia (B), S shaped or sigmoid kidney (C), Cake or lump (D), Disc or doughnut (E) and L shaped or tandem kidney (F) [3]. Our case felt under Category (A). Many theories have been postulated like influence of genetic factor, teratogenic factor or malalignment and abnormal rotation of caudal end of embryo that will lead to aberrant development of metanephric blastema and ureteric bud during the 4th to 8th week of gestation. So, both kidneys could not achieve normal position but the exact cause of crossed ectopia is still not known and eventual shape and site of the kidneys depend upon the time and amount of fusion and extent of rotation [3,4]. Most cases of crossed renal ectopia were diagnosed incidentally as these are generally asymptomatic. However, if symptomatic then the most common presenting symptoms are abdominal or flank pain, a palpable mass, dysuria or haematuria. Ureteral orifices are usually orthotopic in these kinds of anomalies with only 3% that have ectopic ureteric orifices. Anomalies like Vesicoureteric Reflux (VUR), ureterocoele, nephrolithiasis, Ureteropelvic Junction (UPJ) obstruction and very rarely carcinoma can be associated with these anomalies [3-5]. VUR is the most common associated anomaly that can lead to pyelonephritis [5]. Our patient was also a male and both kidneys of our patient were ectopic but he did not have any other associated anomaly except having a small nonobstructed renal calculus. There are no specific primary approaches for the management of these anomalies and treatment should be tailored according to associated anomalies [6,7]. There are various investigations like CECT, Magnetic Resonance Imaging (MRI) or Intravenous Pyelography (IVP) and renal scintigraphy for diagnosis of these anomalies but Multi Detector Computed Tomography (MDCT), urography is the investigation of choice for these anomalies [8,9]. Temporary episodes of urinary pathway obstruction can lead to acute abdominal pain. However, in our cases patient had history of only occasional dull aching pain (with no episodes of colic), which could be due to a small calculus or more commonly non specific [10]. Our patient did well without any intervention and managed only with analgesics. Regular follow up was done for three years which suggested that in the absence of any other associated anomaly these patients can be easily managed only by conservative measures.
Conclusion
Although silent, and mostly detected in autopsy specimen. In clinical practice, these conditions are mostly detected incidentally during evaluation of other condition unless it is associated with other anomalies or complicated by obstruction or infection. This can be observed in various clinical forms and management should be planned according to the clinical presentation and anatomical abnormality.
[1]. Shapiro E, Telegrafi S, Anomalies of form and fusion, crossed renal ectopia with and without fusionIn Campbell-Walsh Urology Book, Wein A. J. et al, editors 2016 11th edPhiladelphiaWB Saunders:2988-93. [Google Scholar]
[2]. Boyan N, Kubat H, Uzum A, Crossed renal ectopia with fusion: report of two patientsClinical Anatomy 2007 20(6):699-702. [Google Scholar]
[3]. Abeshouse B S, Bhisitkul I, Crossed renal ectopia with and without fusionUrol. Int 1959 9:63 [Google Scholar]
[4]. Patel T V, Singh A K, Crossed fused ectopia of the kidneysKidney International 2008 73(5):662 [Google Scholar]
[5]. Shaikh T P, Ansari S, Thahir V U, Mandhane N, Karandikar S, Cross fused ectopic kidney: A rare congenital malformation with review of literatureInt J Sci Rep 2015 1(3):166-68. [Google Scholar]
[6]. Akdogan L, Oguz A K, Ergun T, Ergun I, The rarest of the rare: crossed fused renal ectopia of the superior ectopia typeCase Reports in Nephrology 2015 Article ID 742419, 4 pages, 2015 [Google Scholar]
[7]. Solanki S, Bhatnagar V, Gupta A K, Kumar R, Crossed fused renal ectopia: Challenges in diagnosis and managementJournal of Indian Association of Pediatric Surgeons 2013 18(1):07-10. [Google Scholar]
[8]. Turkvatan A, Olçer T, Cumhur T, Multidetector CT Urography of renal fusion anomaliesDiagn Interv Radiol 2009 15:127-34. [Google Scholar]
[9]. Sharma V, Ramesh Babu CS, Gupta OP, Crossed fused renal ectopia: Multidetector computed tomography studyInt J Anat Res 2014 2(2):305-09. [Google Scholar]
[10]. Ramaema D P, Moloantoa W, Parag Y, Crossed renal ectopia without fusion—An unusual cause of acute abdominal pain: A Case ReportCase Reports in Urologyvol. 2012, Article ID 728531, 4 pages, 2012 [Google Scholar]