Chondroid Lipoma in Left Thigh –A Rare Case Report
Sachin Shivaji Kapse1, Surekha U.2, Anita P. Javalgi3
1 Postgraduate, Department of Pathology, BLDEU’s, Shri. B.M. Patil Medical College, Vijayapura, Karnataka, India.
2 Professor, Department of Pathology, BLDEU’s, Shri. B.M. Patil Medical College, Vijayapura, Karnatak, India.
3 Assistant Professor, Department of Pathology, BLDEU’s, Shri. B.M. Patil Medical College, Vijayapura, Karnatak, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sachin Shivaji Kapse, Postgraduate, Department of Pathology, BLDEU’s, Shri. B.M. Patil Medical College, Vijayapura-586103, Karnataka, India.
E-mail: sachinkapse004@gmail.com
Chondroid lipoma is a rare variant of lipoma and often confused with chondroid tumours such as soft tissue chondroma, extraskeletal chondrosarcoma and myxoid chondrosarcoma. It consists of two components – adipose tissue and cartilaginous tissue. Differentiating chondroid lipoma from its malignant variant such as extraskeletal chondrosarcoma and myxoid chondrosarcoma is necessary as the treatment modality is more intense and aggressive for latter. Here we are presenting histopathological features and differential diagnosis in an unusual case of chondroid lipoma in a 40-year-old female.
Extraskeletal chondrosarcoma, Myxoid chondrosarcoma, Soft tissue chondroma
Case Report
A 40-years-old female patient presented in Surgery OPD with complaints of slow growing, painless mass in the left thigh since one year. There was no history of trauma. On clinical examination, vague, non-tender and mobile mass was noted in left thigh. Based on the history of slow growing mass which was mobile, clinical diagnosis of benign soft tissue tumour was made. The mass was completely excised and sent for histopathological study.
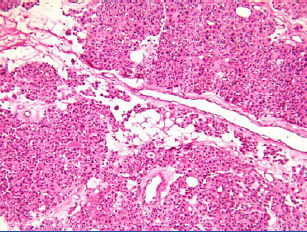
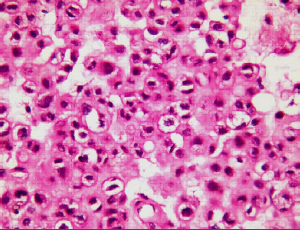
Grossly, it was an encapsulated, irregular mass measuring 4 x 3 x 2 cm with adherent fibromuscular tissue at places [Table/Fig-1]. Cut surface of the mass was solid, lobulated, yellowish white with chondroid tissue focally. Microscopic examination of multiple sections revealed well circumscribed, encapsulated tumour tissue comprised of lobules of mature adipose tissue admixed with cartilage nodules in a fibromyxoid stroma [Table/Fig-2]. Also, noted were many round to oval cells with round to oval nucleus having vacuolated and eosinophilic cytoplasm suggestive of lipoblast-like cells [Table/Fig-3]. There was no evidence of nuclear pleomorphism, mitotic activity, plexiform capillaries and necrosis. Periphery of the tumour tissue showed, skeletal muscle bundles free of tumour tissue. PAS stain of section showed positivity for intracytoplasmic glycogen and neural fat [Table/Fig-4]. S100 showed faint positivity for small vacuolated cells i.e., lipoblast-like cells.
Gross morphology of chondroid lipoma showing yellowish fibrofatty mass.

Photomicrograph showing admixture of mature adipose tissue with cartilaginous tissue. (H and E, 10X).
Photomicrograph showing chondroid tissue along with few lipoblast –like cells (H and E, 40X).
Photomicrograph showing intracytoplasmic positivity for PAS. (PAS, 40X).
Based on above histomorphological features diagnosis of chondroid lipoma was made. Follow up after four months showed no signs of local recurrence or metastasis.
Discussion
Chondroid lipoma is an unusual benign mesenchymal tumour arising from adipose tissue. It was first described by Meis JM and Enzinger FM in 1993. It consists of two components – adipose tissue and cartilaginous tissue [1]. It can occur in any age group but most of them present at the age group of 30 to 40 years. Females are more commonly affected as compared to males. Most common sites for chondroid lipoma are proximal extremities, limb girdle, leg, trunk, head and neck region. Rarely, it can also occur in feet and hands. It can arise from superficial muscular fascia, skeletal muscle or subcutis [2]. In the present case location of tumour was in the skeletal muscle. Due to presence to fibromyxoid matrix and lipoblast-like cells and close resemblance to the histomorphological features of chondrosarcomas there are high chance to be misdiagnosed as extraskeletal chondrosarcoma or myxoid chondrosarcoma [1-5].
Chondroid lipoma is composed of cartilaginous tissue and mature adipose tissue with features of both embryonal fat and embryonal cartilage [6]. Histopathologically it has close resemblance to myxoid chondrosarcoma, extraskeletal chondrosarcoma, soft tissue chondroma and myoepithelial tumours. Differentiating it from myxoid liposarcoma is difficult as both of them share similar features clinically and radiologically. Hence, microscopic examination is necessary to differentiate chondroid lipoma from myxoid liposarcoma. Myxoid liposarcoma shows atypical spindle cells, plexiform vascular pattern and show S100, vimentine and CD36 positivity. Extraskeletal myxoid chondrosarcoma show hypercellularity and pleomorphism of chondroid tissue with few cells containing intracytoplasmic vacuoles. Soft tissue chondroma is seen in young adults and is usually located in hand and feet and can locally recur. Microscopically, it contains multinucleated giant cells. Myoepithelial tumours are located superficially and show absence of multivacuolated cells and shows keratin, EMA and smooth muscle actin positivity on Immunohistochemistry (IHC) [1-5]. In present case, atypical spindle cells, plexiform vascular pattern, pleomorphism, intracytoplasmic vacuoles and multinucleate giant cells were absent, hence this case was concluded as chondroid lipoma.
As it is easily misdiagnosed and can lead to unnecessary overt surgical treatment. Hence awareness of this entity is must as chondroid lipoma has better prognosis compared to myxoid liposarcoma and extraskeletal chondrosarcoma [4].
When diagnostic difficulty between chondrolipoma and myxoid liposarcoma is their IHC will help to differentiate. Tumour cells in chondroid lipoma are positive for S100 and vimentine while there will be no reactivity for keratin, smooth muscle actin, muscle specific actin and CD36 [1,2].
Radiological imaging data is sparse due to rarity of lesion. On MRI, T1W shows low intensity and high intensity on T2W, chondroid tissue shows well demarcated and lobulated shape. Marked diffuse peripheral enhancement, with arcs and rings enhancement patterns in the central part will be seen on gadolinium aspiration. Similar findings can be seen in liposarcoma, extraskeletal chondroma, chondrosarcoma [7]. In present case, as clinical diagnosis of lipoma was made, radiological evaluation was not done.
The chondroid lipoma is cured by simple surgical excision while myxoid chondrosarcoma and extraskeletal chondrosarcoma requires wide surgical excision as well as radiotherapy. If chondroid lipoma is misdiagnosed as myxoid chondrosarcoma or extraskeletal chondrosarcoma it may cause undue psychological trauma to the patient in addition unnecessary expenses [1-5]. Therefore, motive of this case report is to create awareness as well as to put light on this variant of lipoma where lack of experience/exposure may lead to misdiagnosis.
Conclusion
Chondroid lipoma is a recently described rare variant of benign lipomatous tumour. Due to high cellularity and morphology of the cells, it can be misdiagnosed as myxoid chondrosarcoma and extraskeletal chondrosarcoma. Awareness of this entity is important in order to avoid over diagnosis of soft tissue sarcoma and subsequent overtreatment.
[1]. Meis JM, Enzinger FM, Chondroid lipoma. A unique tumour simulating liposarcoma and myxoid chondrosarcomaAm J Surg Pathol 1993 17:1103-12. [Google Scholar]
[2]. Yaranal PJ, Hegde V, Chondroid lipoma of the thigh: A case reportIndian J Pathol Microbiol 2013 56:464-65. [Google Scholar]
[3]. Setiawati R, Dimpudus FJ, Sun Z, Chondroid lipoma of the right thigh: Correlation of imaging findings & histopathology of an unusual benign lesionAMJ 2012 5:355-58. [Google Scholar]
[4]. Gokhale U, Pillai RG, Varghese PV, Samarsinghe D, Chondroid Lipoma: A case reportOman Med J 2008 23:116-17. [Google Scholar]
[5]. Manna AK, Chattopadhyay A, Chowdhury K, Chowdhury MK, Dutta SK, Chondroid lipoma —a case reportIndian J Pathol Microbiol 2006 49:422-24. [Google Scholar]
[6]. Kindblom LG, Lipomatous tumours-how we have reached our present views, what controversies remain and why we still face diagnostic problems: A tribute to Dr Franz EnzingerAdv Anat Pathol 2006 13:279-85. [Google Scholar]
[7]. Yildiz AE, Aydingoz U, Sokmensuer C, Karcaaltincaba M, Intramuscular Chondroid Lipoma: Magnetic Resonance Imaging Diagnosis by “Fat Ring Sign.”Balkan Med J 2015 32(1):107-10. [Google Scholar]