A Rare Case of Osteopetrosis with Unusual Feature as Microcephaly
Parul Bhati1, P C Goyal2
1 Assistant Professor, Department of Paediatrics, North DMC Medical College and Hindu Rao Hospital, Delhi, India.
2 Professor, Department of Paediatrics, North DMC Medical College and Hindu Rao Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Parul Bhati, 8/6, East Patel Nagar, 3rd Floor, New Delhi-110008, India.
E-mail: parulbhati13@gmail.com
Erlenmeyer flask deformity, Optic atrophy, Sandwich appearance of vertebra
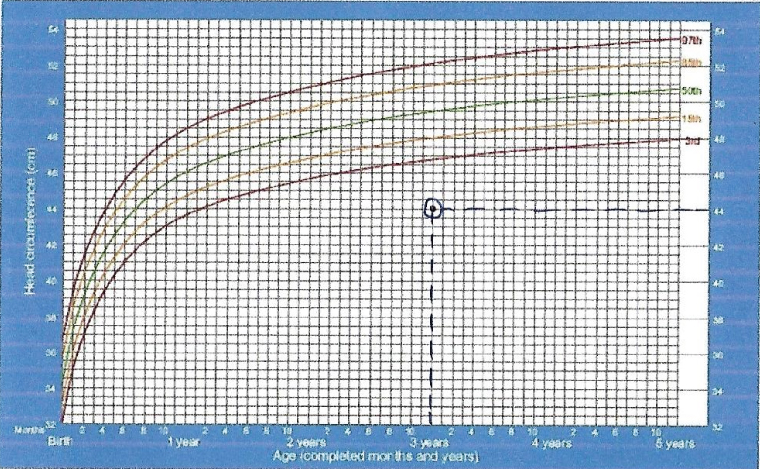
A three-years-old child was admitted in paediatric ward in Hindu Rao Hospital with complaints of fever on and off for 14 days with yellowish discoloration of eyes. Child had inability to walk with progressive swelling of abdomen with protrusion of eyes for last two years. Child had developmental delay. At three years of age he could walk with support, had immature pincer grasp, could recognize family members and could speak 2-3 word sentences. There was history of elder sibling`s death at age of 18 months due to similar illness. On examination, child was alert but irritable with pallor, icterus and proptosis. Child had microcephaly with head circumference 44 cm (<-3 SD, 88% of median) [Table/Fig-1]. Abdomen was distended with dilated veins, umbilicus was everted with massive hepatosplenomegaly and ophthalmological examination, revealed bilateral optic atrophy [Table/Fig-2]. Child had anaemia (Hb- 4.4 mg/dl, MCV- 127.4 fL, RDW- 86.4) with thrombocytopenia (Platelet count- 70,000). Peripheral smear was suggestive of megaloblastic anaemia. Skeletal survey showed, generalised increased bone density and Erlenmeyer flask deformity of long bones [Table/Fig-3]. Moreover, skull radiograph showed wide diploe space and increased density of base, also, radiograph of spine showed alternate dense and lucent bands suggestive of Rugger Jersey spine (sandwich appearance of vertebrae) [Table/Fig-4] and ‘bone in bone’ appearance of phalanges [Table/Fig-5].
Chart depicting head circumference of infants from birth to five years with the head circumference of present case represented by the dot.
Protruded eyes with abdominal distension due to hepatosplenomegaly.

Erlenmeyer flask deformity of femur.

Skull radiograph showing wide diploe space (right) and radiograph of spine showing ‘sandwich’ appearance of vertebrae.

Increased bone density and ‘bone in bone’ appearance of phalanges.

Osteopetrosis is a Greek word meaning stony bone. It is also known as ‘Marble bone disease’ and ‘Albers-Schönberg disease’, after German radiologist who described this condition in 1904. The incidence of autosomal recessive osteopetrosis is one in 250,000 births [1] and that of autosomal dominant osteopetrosis is five in 100,000 births [2]. Its severity ranges from asymptomatic to fatal consequence.
Discussion
Osteopetrosis patients have increased bone density due to defective bone resorption [3]. In osteopetrosis, there are molecular defects in osteoclasts resulting in imbalance between bone formation by osteoblasts and bone resorption by osteoclasts. It has three clinical types: (1) Autosomal recessive malignant form; (2) Autosomal recessive intermediate form; and (3) Autosomal dominant benign form [4]. In present case, according to age and severity of presentation, autosomal recessive malignant form is likely to be observed. This is further supported by the fact that one elder sibling died at an early age of 18 months with similar illness in family. Autosomal recessive malignant osteopetrosis manifests in infants and is of fatal variety. In osteopetrosis, bones are weak and prone to fractures whereas, in osteomyelitis, there is impairement of bone growth resulting in short stature. Patients usually present with typical facial appearance with macrocephaly and frontal bossing but in present case, microcephaly was observed. Microcephaly is an atypical finding in osteopetrosis and it has been reported in very few cases [5,6]. Choanal stenosis and hydrocephalus occurs because of skull changes [7]. Blindness, deafness and facial palsy occur due to narrowing of nerve foramina. Similarly, in present case bilateral optic atrophy was present probably due to optic nerve formina compression. Patients of osteopetrosis can also present with hearing loss, tooth eruption defects, severe dental caries, hypocalcaemia, tetanic seizures and secondary hyperparathyroidism. Abnormal expansion of bone causes bone marrow suppression resulting in pancytopenia and anaemia. This causes secondary expansion of extramedullary haematopoietic sites like liver and spleen. In above mentioned case, anaemia, pancytopenia and extramedullary haematopoiesis was present as evident by massive hepatosplenomegaly.
The diagnosis is usually based on clinical and radiological findings. The typical radiological feature included diffuse sclerosis of all bones. Metaphysis of long bones have characteristic funnel like appearance causing Erlenmeyer flask deformity. In present case, typical Erlenmeyer flask deformity was noted in femoral bone due to alternating bands of sclerosis. Vertebrae and phalanges have “Bone-in-bone” appearance. Focal sclerosis of vertebrae gives rise to “sandwich” vertebrae and “rugger-jersey” spine [3]. Present case also, showed the ‘sandwich’ appearance in vertebrae.
Treatment is based on correcting symptoms and managing complications. The definitive cure of osteopetrosis is human stem cell transplantation. It is usually done in severe forms of osteopetrosis due to high associated morbidity and mortality. Vitamin D supplementation to stimulate osteoclast, corticosteroid and erythropoietin to treat anaemia and gamma interferon to improve immunity are used. Infantile malignant osteopetrosis is associated with diminished life expectancy while it is normal for adult forms.
Conclusion
Osteopetrosis has varied presentation and can present from mild autosomal dominant form to severe autosomal recessive forms. Affected patients can have severe anaemia, thrombocytopenia with extramedullary haematopoiesis evidenced by hepatosplenopomegaly. These patients usually have macrocephaly but might present with atypical manifestation of microcephaly. There is no effective medical treatment for osteopetrosis and it is largely symptomatic.
[1]. Loria-Cortes R, Quesada-Calvo E, Cordero-Chaverri C, Osteopetrosis in children: A report of 26 casesJ Pediatr 1977 91(1):43-47. [Google Scholar]
[2]. Bollerslev J, Andersen PE, Radiological, biochemical and hereditary evidence of two types of autosomal dominant osteopetrosisBone 1988 9(1):7-13. [Google Scholar]
[3]. Stark Z, Savarirayan R, OsteopetrosisOrphanet Journal of Rare diseases 2009 4(1):5 [Google Scholar]
[4]. Kocher MS, Kasser JR, OsteopetrosisAm J Orthop (Belle Mead NJ) 2003 32(5):222-28. [Google Scholar]
[5]. Ocal G, Berberoglu M, Adiyaman P, Cetinkaya E, Ekim M, Aycan Z, Osteopetrosis, renal tubular acidosis without urinary concentration abnormality, cerebral calcification and severe mental retardation in three Turkish brothersJ Pediatr Endocrinol Metab 2001 14(9):1671-77. [Google Scholar]
[6]. Shah AM, Boby KF, Karande SC, Lahiri KR, Jain MK, Three sibs with mild variety of osteopetrosisJournal of postgraduate medicine 1996 42(4):123-25. [Google Scholar]
[7]. Al-Tamimi YZ, Tyagi AK, Chumas PD, Crimmins DW, Patients with autosomal-recessive osteopetrosis presenting with hydrocephalus and hind brain posterior fossa crowdingJ Neurosurg Pediatrics 2008 1:103-06. [Google Scholar]