A Rare Surprising Cause of Acute Severe Pancreatitis
Cyriac Abby Philips1, Philip Augustine2, George Joseph3, Lijesh Kumar4, Pushpa Mahadevan5
1 Associate Director, Department of Hepatology and Liver Transplant Medicine, PVS Institute of Digestive Diseases, Kochi, Kerala, India.
2 Chairman, Department of Gastroenterology, PVS Institute of Digestive Diseases, Kochi, Kerala, India.
3 Senior Consultant, Department of Radiology, PVS Institute of Digestive Diseases, Kochi, Kerala, India.
4 Consultant, Department of Radiology, PVS Institute of Digestive Diseases, Kochi, Kerala, India.
5 Head, Department of Pathology, Lakeshore Hospital, Kochi, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Philip Augustine, Associates, PVS Memorial Hospital Campus, Kaloor, Kochi-682017, Kerala, India
E-mail: abbyphilips@gmail.com
A 39-year-old woman is admitted with clinical, biochemical and imaging features suggestive of acute pancreatitis. Conservative and guideline based management failed to improve her condition. Repeate the imaging utilizing contrast revealed the progression of extra-pancreatic signs in the absence of pancreatic necrosis, the absence of intra-abdominal fluid collections, but enhancing omental and peritoneal deposits and obstructive pancreatitis. A biopsy and histopathological evaluation of the omentum revealed rare anaplastic large cell lymphoma causing obstructive pancreatitis. In patients who present with pancreatitis not responding to conventional treatment and with an atypical disease course, the diagnostic possibility of rare causes of pancreatitis such as obstructive/infiltrative pathology must be thought of.
Anaplastic lymphoma, B-cell lymphoma, Critical care, Multiple organ failures, Pancreatitis
Case Report
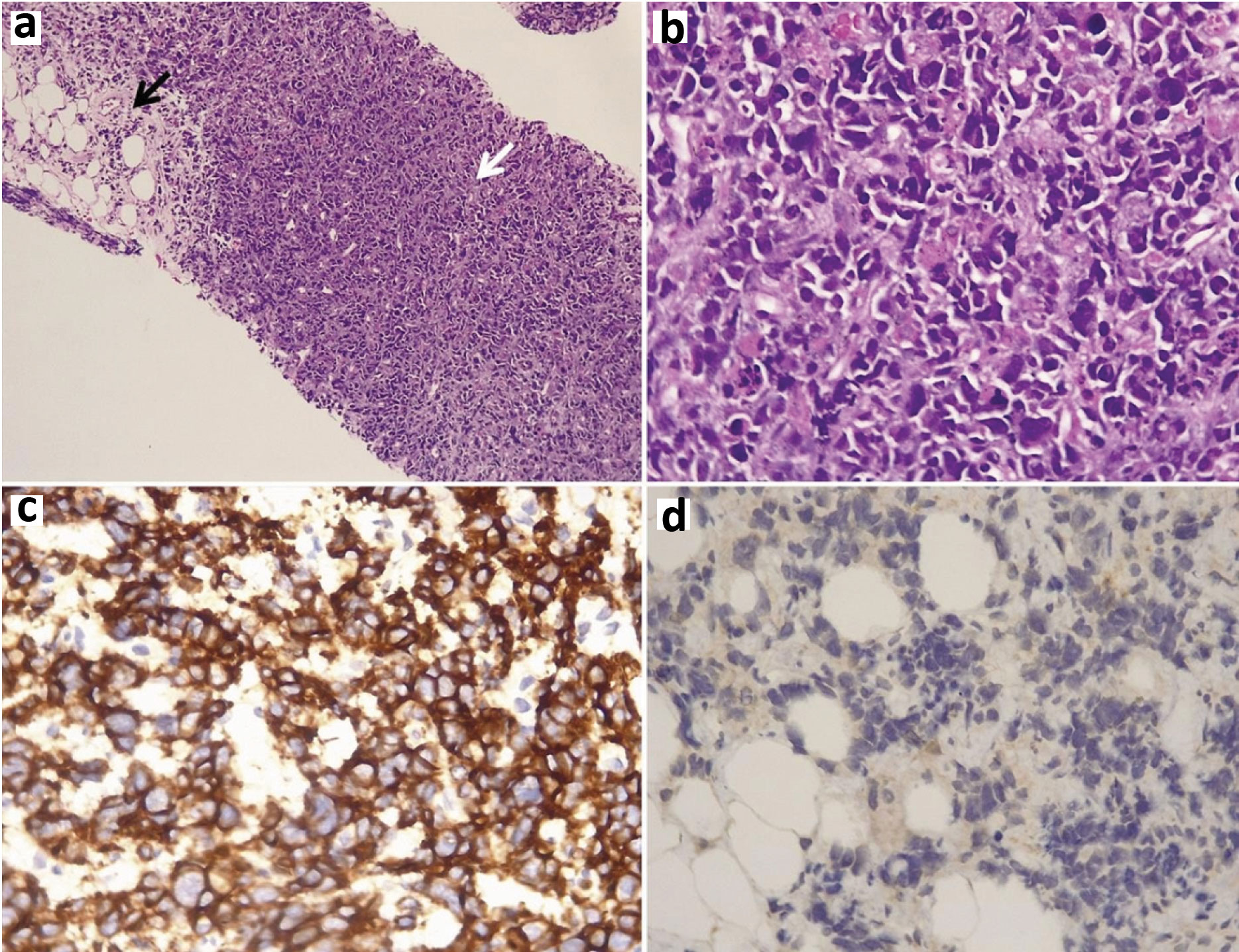
A 39-year-old female reported complaining of severe epigastric pain which was radiating to the back since four days and was associated with obstipation and progressive abdominal distension. She consumed two to three tablets of 50 mg diclofenac per day for two days with mild improvement in pain. In the event of new onset lower limb swelling and facial puffiness, the patient was taken to a nearby primary care center where she was diagnosed to have acute severe pancreatitis based on leukocytosis, raised serum amylase and lipase {642 U/L; reference range: (60-108 U/L) and 988 U/L; reference range: (7-58 U/L) respectively}, with bulky pancreas on ultrsonography and possible drug induced acute kidney injury. She was kept nil per oral and judicious intravenous fluid management was given. Twenty four hours later, anuria ensued with advanced azotemia, requiring multiple haemodialysis sessions. When the abdominal symptoms and signs worsened two days later, she was referred to our center for further management. Clinical evaluation revealed a conscious but drowsy patient with tachycardia and tachypnea and tender doughy abdomen with guarding and sluggish bowel sounds. In the presence of renal failure, a plain Computed Tomography (CT) of the abdomen was done that showed bulky pancreas with extensive mesenteric inflammation, with mild peri-hepatic and peri-pancreatic fluid. The patient was managed conservatively with naso-jejunal (fluoroscopy guided, difficult to place) feeds, intravenous antibiotics and renal replacement therapy. Three days later, in the absence of clinical improvement, ultrasound abdomen revealed the persistence of mesenteric and omental thickening with the similar appearing pancreas, without overt fluid collections. The initial diagnosis was challenged and a contrast CT of abdomen was performed after obtaining high risk consent from next of kin, which revealed extensive enhancement, thickening and matting of stomach and proximal small intestine with enhancing peritoneal nodules, necrotic sub-diaphragmatic lymph nodes and bulky heterogeneously enhancing pancreas [Table/Fig-1a-c]. Image guided core biopsy of the omentum was done. Histopathology revealed healthy omental fibro-fatty tissue (black arrow, [Table/Fig-2a]) with neoplasm arranged in sheets (white arrow, [Table/Fig-2a]) with cells showing a moderate amount of eosinophilic cytoplasm and pleomorphic hyperchromatic nucleus [Table/Fig-2b]. The tumour cells were leucocyte common antigen, cMyc, CD 30 [Table/Fig-2c] and CD 43 positive with cytokeratin 7 and 20 [Table/Fig-2d], Anaplastic Lymphoma Kinase (ALK), CD25, CD20, CD3, Bcl 2, Tdt and MUM-1 negative, consistent with ALK negative anaplastic large B-cell lymphoma with high proliferation index (Ki67 >80%) which led to secondary tumour infiltration related obstructive pancreatitis. Rapid progression of disease with multi organ failure followed within the next 36 hours rendering the patient ineligible for chemotherapy regimen. The patient succumbed to her illness 12 days after admission to the hospital.
a) Plain Computed Tomography (CT) of abdomen showing bulky pancreas with extensive mesenteric inflammation, with mild peri-hepatic and peri-pancreatic fluid; b) Contrast enhanced CT of abdomen revealing enhancing peritoneal nodules and necrotic sub diaphragmatic lymph nodes with; c) Extensive enhancement, thickening and matting of stomach and proximal small intestine and bulky heterogeneously enhancing pancreas.

a) Histopathology of omental biopsy showing normal omental fibro-fatty tissue (black arrow; haematoxylin and eosin stain, 10x) with neoplasm arranged in sheets (white arrow, haematoxylin and eosin stain, 10x) with; b) Tumour cells showing moderate amount of eosinophilic cytoplasm and pleomorphic hyperchromatic nucleus (haematoxylin and eosin stain, 40x); c) The tumour cells showed CD 30 positivity Immunohistochemistry (IHC) stain, 40x) and d) Negative for cytokeratin 7 and 20 immunohistochemical stains (IHC stain, 40x)
Discussion
Primary pancreatic lymphomas are very rare pancreatic malignancies and constitute less than 2% of extra-nodal lymphomas. Primary pancreatic anaplastic large cell lymphomas are extremely rare. Still rarer is anaplastic large cell lymphomas involving the pancreas secondarily, leading to acute pancreatitis as the index presentation [1]. Here, we present the case of a young woman who presented with acute severe pancreatitis and in whom initial imaging was highly suggestive of pancreatitis. In the presence of inadequate response to treatment, re assessment led to the diagnosis of anaplastic large B cell lymphoma, secondarily involving the pancreas leading to obstructive pancreatitis, a rare causation.
Lymphoma involving the pancreas is rare (1-2%) in comparison to pancreatic adenocarcinoma and is mostly of non-Hodgkin’s type. Diffuse Large B-Cell Lymphoma (DLBCL) of the pancreas is a rarity, and index presentation as acute pancreatitis is uncommon and seldom reported in the literature [2]. Anaplastic Large Cell Lymphoma (ALCL) is an aggressive CD30 positive non-Hodgkin lymphoma that can either be ALK positive or negative with the former typically occurring in younger patients with a favourable prognosis and survival rates of 70% in comparison to the latter (survival rate of 40%) at five years. Primary pancreatic ALCL are exceedingly rare with lesser than 10 cases reported in the current literature and most of them presenting as pancreatic masses [3]. Primary pancreatic lymphoma is diagnosed based on Dawson’s criteria which include neither superficial lymphadenopathy nor enlargement of mediastinal lymph nodes on chest radiography; a normal leukocyte count in peripheral blood and main mass in the pancreas with lymph node involvement confined to the peripancreatic region; without hepatic or splenic involvement [4]. In our patient extensive involvement of sub-diaphragmatic and abdominal lymph nodes, omentum and peritoneum and enhancement and matting of stomach and bowel favoured a secondary involvement of the pancreas. We could not perform a bone marrow biopsy to understand the extent of the disease in view of rapid progression and early mortality. Also, the complete blood counts at admission were not suggestive of marrow infiltration. We did not find reports on systemic ALK negative ALCL diffusely involving the upper gastrointestinal tract and pancreas and presenting with acute severe pancreatitis [5]. Ishida M et al., described the first documented case of ALCL following IgG4-related autoimmune pancreatitis and cholecystitis and DLBCL and suggested that malignant lymphoma may be high in patients with IgG4-related sclerosing disease and that intense medical follow-up was necessary [6]. Luther J et al., described the case of a previously healthy young woman who developed acute sclerosing mesenteritis secondary to anaplastic lymphoma, diagnosed post mortem [7], highlighting the plethora of presentations with rare lymphomas, aswas seen in our patient. Treatments for ALCL include anthracycline-based regimens such as cyclophosphamide, doxorubicin, vincristine, prednisone which is usually ineffective in ALK negative patients and needs to be coupled with antibody drug conjugate brentuximab vedotin or autologous stem cell transplantation [3], all of which were inappropriate options in our patient with multiple organ failures. Contrast studies and where required, histopathology is of utmost importance in diagnosing different causes/mimickers of pancreatitis in patients presenting with an atypical disease course and not responding to traditional treatments.
Conclusion
Acute pancreatitis is clearly diagnosed in the presence of classical clinical, biochemical and imaging features. Unusual causes of pancreatitis include groove pancreatitis, autoimmune or IgG4 related pancreatitis, pancreatitis associated with atypical infections such as dengue or leptospirosis and pancreatitis in the presence of pancreatic adenocarcinoma. However, in patients who present with clinical features of pancreatitis with an atypical disease course, such as those with rapidly progressing symptoms, those not responding to conventional treatment and with atypical imaging features such as predominant extra-pancreatic features, obstructive causes of pancreatitis due to pancreatic infiltration by malignancy such as lymphoma must be considered. In such a situation, biopsy and histopathology examination must be undertaken to confirm the diagnosis. Additionally, this decision can only be drawn, based on contrast imaging of the abdomen early in the course of the disease evaluation. Anaplastic large cell lymphomas involving the pancreas secondarily, leading to acute pancreatitis as the index presentation is rarely described in the literature.
[1]. Savopoulos CG, Tsesmeli NE, Kaiafa GD, Zantidis AT, Bobos MT, Hatzitolios AI, Primary pancreatic anaplastic large cell lymphoma, ALK negative: a case reportWorld J Gastroenterol 2005 11:6221-24. [Google Scholar]
[2]. To CA, Quigley MM, Saven A, Nicholson L, Masquerade without a mass: an unusual cause of severe acute pancreatitisJ Gastrointest Oncol 2013 4:114-17. [Google Scholar]
[3]. Ahmed B, Estey E, Manning J, David C, Keating MJ, Kantarjian H, Anaplastic large cell lymphoma with involvement of the pancreas presenting as panniculitisin a patient with a history of acute myeloid leukemia-case report and review of the literatureHaematologica 2006 91:e150-e152. [Google Scholar]
[4]. Saif MW, Primary pancreatic lymphomasJOP 2006 7:262-73. [Google Scholar]
[5]. Xing X, Feldman AL, Anaplastic large cell lymphomas: ALK positive, ALK negative, and primary cutaneousAdv Anat Pathol 2015 22:29-49. [Google Scholar]
[6]. Ishida M, Hodohara K, Yoshida K, Kagotani A, Iwai M, Yoshii M, Occurrence of anaplastic large cell lymphoma following IgG4-related autoimmune pancreatitis and cholecystitis and diffuse large B-cell lymphomaInt J Clin Exp Pathol 2013 6:2560-68. [Google Scholar]
[7]. Luther J, Faje AJ, Al-Hawary M, Kao JY, Anaplastic lymphoma masquerading as sclerosing mesenteritis: a case reportJ Gastrointest Cancer 2012 43:364-66. [Google Scholar]