Sacrococcygeal Teratoma in a Seven-Day-Old Child with Pulmonary Differentiation
Barkha Gupta1, Surekha Yadav2, Nita Khurana3, Prince Raj4
1 Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
2 Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
3 Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
4 Assistant Professor, Department of Paediatric Surgery, Lok Nayak Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Barkha Gupta, Room No.62, Pathology Block, Maulana Azad Medical College, New Delhi-110002, India.
E-mail: barkhaguptadr@gmail.com
Sacrococcygeal Teratoma (SCT) showing pulmonary differentiation has been rarely reported in the literature. Till date, only eight cases have been reported, out of which six belong to teratomas arising from female genital tract. Spinal teratomas showing pulmonary differentiation are rarer and only two cases have been reported so far in the literature both of which had associated congenital spinal anomaly.
We present a rare case of seven day old infant with sacrococcygeal teratoma showing mature lung differentiation as one of its components. The infant was otherwise asymptomatic and had no associated spinal anomaly. This case has been presented for its rarity. Extensive review of the literature along with the possible pathogenesis is also included for better understanding.
Infant, Mature lung, Organoid differentiation
Case Report
A seven-day-old, full term infant was presented at the Paediatric Surgery outpatient department with a swelling on back since birth. No history of fever, vomiting or bladder and bowel dysfunction was present. The swelling did not vary in size on coughing/crying. No similar family history was present. On examination, child was 2.2 kg in weight, head and chest circumference were within normal limits. A single, lobulated swelling measuring 8×4 cm, was seen in the pre-sacral region. Overlying skin was shiny and showed prominent veins. Swelling had variable consistency with well-defined margins. It was non-fluctuant and non-compressible. Impulse on coughing was absent. Physical examination revealed no gross congenital anomaly or spinal abnormality and both lower limbs were equal in length. Anal opening was seen at its normal position. Central nervous system examination was within normal limits. Plain radiography of pelvis revealed a solid cystic mass in the sacrococcygeal region compatible with teratoma [Table/Fig-1a].
a) Plain Radiograph of pelvis revealing a solid cystic mass in the sacrococcygeal region marked by arrow; b) Gross specimen of 8×4 cm size, revealing variegated, solid-cystic appearance.
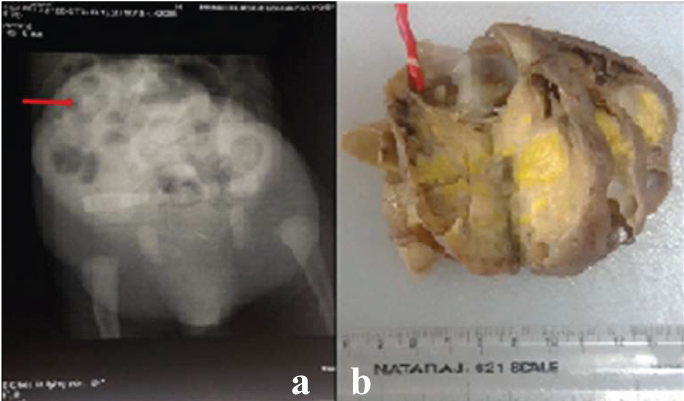
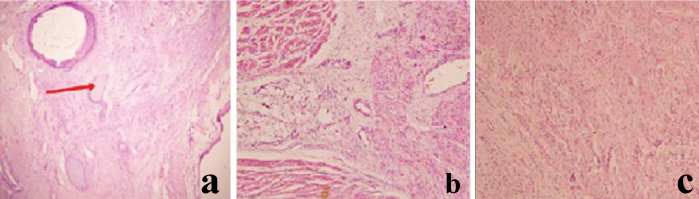
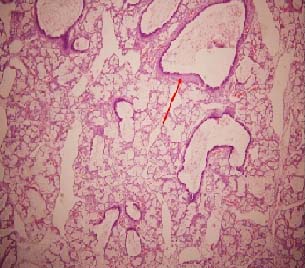
Excision of sacrococcygeal mass along with part of coccyx was performed using Mercedes-Benz incision and sent for histopathological examination. The excised specimen comprised of globular soft tissue bits measuring 8×4 cm. Cut section was solid cystic, variegated with presence of mature fat and grey white fibrous areas [Table/Fig-1b]. Grossly, teeth were not seen. Mature lung tissue was not seen. Microscopy revealed areas showing teratomatous component from all three germ layers. Skin and subcutaneous tissue, keratin flakes, cartilage [Table/Fig-2a], adnexal structures, mature fat, muscle [Table/Fig-2b], mature neural tissue [Table/Fig-2c], mucous glands, cartilage and bone were conspicuous. The pulmonary differentiation was prominent and comprised of bronchial tissue lined by pseudostratified ciliated columnar lined glands with scattered goblet cells. Dilated and oedematous normal alveoli were prominently seen [Table/Fig-3]. No immature element was noted.
Tissue derived from various germ cell layers; a) Stratified squamous epithelium along with cartilage (marked with arrow); b) Muscle and fat; c) Neural tissue (a-c: H&E, 200X).
Pulmonary differentiation with presence of alveoli formation and bronchial cartilage (marked with arrow) (H&E, 200X).
The postoperative period was uneventful and the patient was discharged after one week. The patient was asymptomatic on after one month follow up.
Discussion
SCT appears on the caudal portion of the newborn and accounts for 40% of all teratomas in the first two decades of life [1]. The incidence of the disease is between 1/35,000 and 1/40,000 live births and has a female:male ratio of 4:1 [2]. The tumour arises from embryologically multipotent cells of Hensen’s node located within the coccyx [3] and are now-a-days, increasingly diagnosed by prenatal obstetric ultrasound [4].
Teratomas per se are very commonly encountered lesions and are composed of wide variety of tissues, foreign to the organ/site involved often representing tissues from all the three germ cells. The histologic spectrum of teratomas has been described mainly in the female genital tract [5-7].
Blackwell WJ et al., extensively studied ovarian teratomas and categorized various components seen on the basis of the frequency of their occurrence. Their study concluded that retina, pancreas, thymus, adrenal gland, pituitary gland, kidney, lung and breast were rare findings being documented in less than 5% cases [5]. Pulmonary differentiation in particular, for unknown reasons, is a rare phenomenon in teratomas and has been reported in five ovarian, one uterine [5-7] and two spinal teratomas till now in the literature [8,9] [Table/Fig-4]. Also, a recent study from Takanashi Y et al., described the presence of bronchial cysts in a mediastinal teratoma [10].
Summary of cases of teratomas with pulmonary differentiation reported till date.
| Case No. | Author | Year | Age | Sex | Site |
|---|
| 1 | Wilms et al., [5] | Not available | Not available | Female | Ovary |
| 2 | Blackwell WJ et al., [5] | 1946 | Not available | Female | Ovary |
| 3 | Blackwell WJ et al., [5] | 1946 | Not available | Female | Ovary |
| 4 | Blackwell WJ et al., [5] | 1946 | Not available | Female | Ovary |
| 5 | Pruszczynski M et al., [6] | 1988 | 48 years | Female | Ovary |
| 6 | Khoor A et al., [7] | 1995 | 33 years | Female | Uterine Cervix |
| 7 | Ramdial PK et al., [8] | 1998 | 2 months | Female | Cervical spine |
| 8 | Jain D et al., [9] | 2007 | 8 months | Male | Lumbar spine |
| 9 | Current case | 2016 | 7 days | Male | Sacrococcygeal region |
Wilms is considered to be the first author, by most articles, who has described pulmonary differentiation in teratoma and has been credited for this by Blackwell et al., [5]
Amongst the various studies reported till date, Wilms is considered to be the first to describe pulmonary differentiation in teratomas, although, no details regarding clinico-pathologic profile of the case is available [5].
Blackwell WJ et al., in their study of 225 ovarian teratomas, described two cases with mature lung formation and one with foetal lung formation. Although, clinicopathologic aspects of the cases have been described in the study, specific data regarding the age of these cases are not known [5].
Pruszczynski M et al., described formation of adult lung in ovarian teratoma in a 48-year-old female. They postulated that the induction of development of mature tissues required longer cyclic functioning of the ovarian follicles therefore; degree of differentiation was dependent on the age of the patient [6]. However, this notion does not fit in with our present case where the lesion was present since birth.
Ramdial PK et al., were the first ones to report pulmonary differentiation in spinal teratoma in a two-month-old child with associated cervical spine dysraphism [8].
Jain D et al., reported second case of mature pulmonary differentiation in dorsal lumbar teratomas in eight-month-old infant. Their case also had associated spinal dysraphism [9].
Rare occurrence of pulmonary differentiation in teratomas of any site largely remains unexplained. Ramdial PK et al., proposed that cell matrix and cell-to-cell signaling, mediated by peptide growth factors and extracellular matrix components can play a pivotal role in determining cellular proliferation, differentiation and migration [8]. Though, authors of this study support their opinion, a precise and careful search of more cases is needed to clarify the hypothesis of pulmonary differentiation within the teratoma.
Conclusion
The present case adds to the literature a rare presentation of SCT exhibiting pulmonary differentiation. More number of cases of organoid differentiation needs to be reported in order to establish definite pathogenesis behind such differentiation.
Wilms is considered to be the first author, by most articles, who has described pulmonary differentiation in teratoma and has been credited for this by Blackwell et al., [
5]
[1]. Tapper D, Lack EE, Teratomas in infancy and childhood. A 54-year experience at the Children’s Hospital Medical CenterAnn Surg 1983 198(3):398-410. [Google Scholar]
[2]. Tuladhar R, Patole SK, Whitehall JS, Sacrococcygeal teratoma in the perinatal periodPostgrad Med J 2000 76(902):754-59. [Google Scholar]
[3]. Herman TE, Siegel MJ, Cystic type IV sacrococcygeal teratomaJournal of Perinatology 2002 22(4):331-32. [Google Scholar]
[4]. Harrison MR, Adzick NS, Holzgreve W, The Unborn Patient: The Art and Science of Fetal Therapy 2001 3rd edPhiladelphiaWB Saunders:709 [Google Scholar]
[5]. Blackwell WJ, Dockerty MB, Masson JC, Mussey RD, Dermoid cysts of the ovary: their clinical and pathological significanceAm J Obstet Gynecol 1946 51:151-72. [Google Scholar]
[6]. Pruszczynski M, Sporny S, Cate LN, Smedts F, Benign cystic ovarian teratoma with lung differentiationZentralbl Allg Pathol 1988 134(7):687-89. [Google Scholar]
[7]. Khoor A, Fleming MV, Purcell CA, Seidman JD, Ashton AH, Weaver DL, Mature teratoma of the uterine cervix with pulmonary differentiationArch Pathol Lab Med 1995 119(9):848-50. [Google Scholar]
[8]. Ramdial PK, Nadvi SS, Mallett R, Cervical spine dysraphism with teratoma exhibiting pulmonary differentiation: case report and review of the literaturePediatr Dev Pathol 1998 1(6):528-33. [Google Scholar]
[9]. Jain D, Sharma MC, Sarkar C, Rishi A, Suri V, Garg A, Spinal teratoma with pulmonary differentiation: a report of rare case and review of literatureFetal Paediatr Pathol 2007 26(4):185-91. [Google Scholar]
[10]. Takanashi Y, Tajima S, Takahashi T, Shinmura K, Koyama S, Neyatani H, Mediastinal mature teratoma with complete gastrointestinal and bronchial wallsRespirology Case Reports 2015 3(3):89-91. [Google Scholar]