Pure Villous Adenoma of the Vesicoureteric Junction Presenting as Pyonephrosis
Gwendolyn Fernandes1, Shital Munde2, Amey Rojekar3
1 Associate Professor, Department of Pathology, Seth G.S. Medical College and K.E.M. Hospital, Mumbai, Maharashtra, India
2 Uropathology Fellow, Department of Pathology, Seth G.S. Medical College and K.E.M. Hospital, Mumbai, Maharashtra, India
3 Assistant Professor, Department of Pathology, Seth G.S. Medical College and K.E.M. Hospital, Mumbai, Maharashtra, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gwendolyn Fernandes, C-802, Swayam, Poonam Garden, Mira Road, Mumbai-401107, Maharashtra, India.
E-mail: drgwenfern@yahoo.co.in
Villous adenomas of the urinary tract are uncommon neoplasms which share similar morphological features with gastrointestinal villous adenomas. Only two case series and around 20 scattered case reports of villous adenoma in the urinary tract have been published in English literature till date. They have been identified mainly in the urinary bladder, urethra, prostate and urachus, but the occurrence of villous adenomas at the vesicoureteric junction has not been described. We present a case of villous adenoma of the vesicoureteric junction which completely occluded the lumen and led to gross pyonephrosis.
Benign neoplasm, Uncommon neoplasm, Urinary tract
Case Report
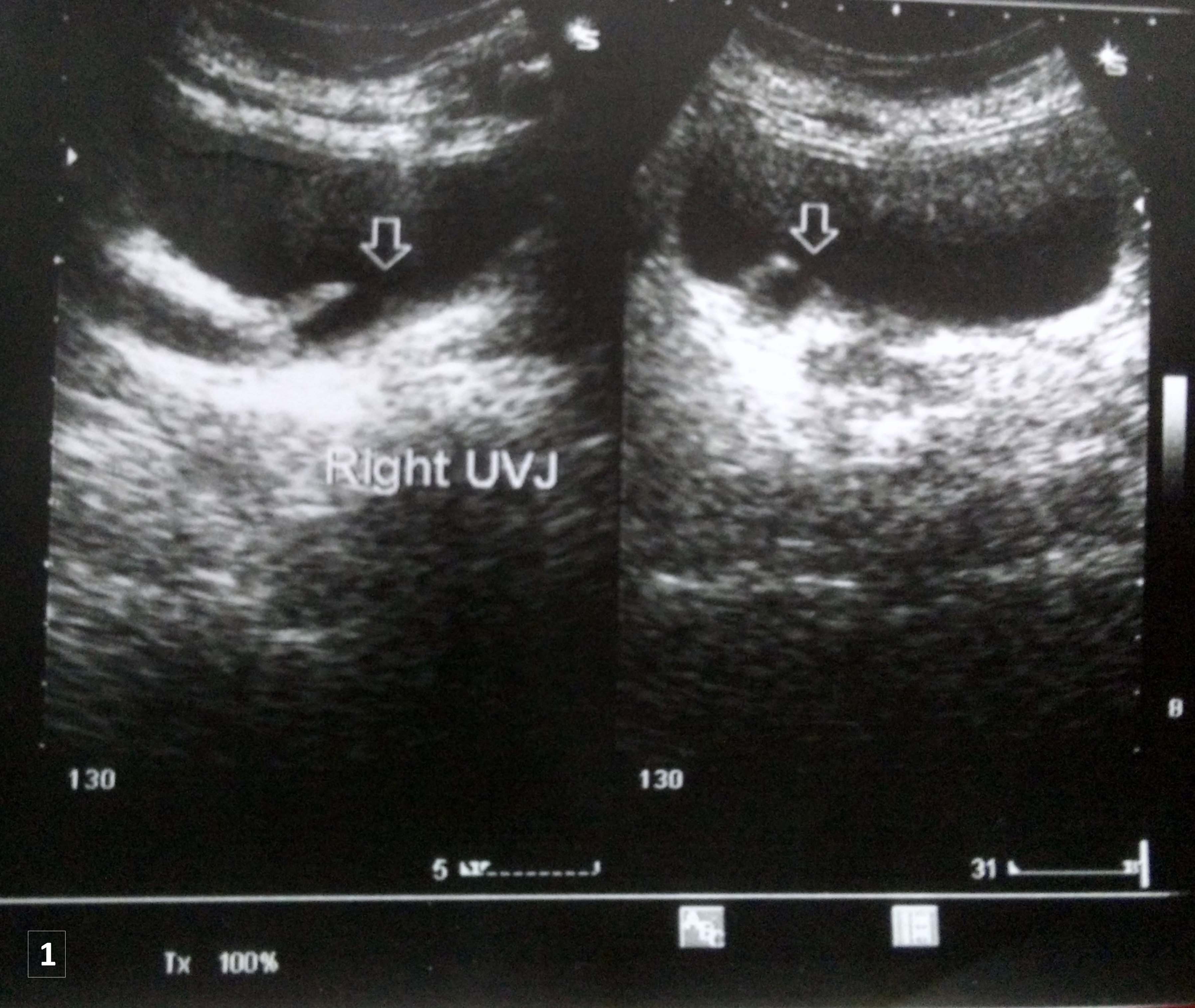
A 50-year-old female presented with right sided flank pain and intermittent fever with chills since four years. She also had anorexia and generalised weakness. There were episodes of pyuria since six months. Haematological investigations showed anaemia and moderate leucocytosis. Her serum creatinine was 1.7 mg/dl and Blood Urea Nitrogen (BUN) was 45 mg/dl. Microscopic urine examination showed 8-10 red blood cells per high power and 60-70 pus cells per high power. Ultrasound examination of abdomen and pelvis showed gross hydronephrosis of right kidney with multiple calculi varying from 6 mm to 35 mm in the lower portion of pelvicalyceal system. The contralateral kidney was normal. A mass lesion, completely occluding the right vesicoureteric junction and projecting into bladder was seen and showed features similar to that of ureterocele [Table/Fig-1]. Cystoscopy was done which showed an exophytic growth in the right vesicoureteric orifice. The ureteroscope was passed into the right ureter up to the mid-pole of the kidney. Pyonephrosis of right kidney was seen. Complete excision of the mass was done and the mass was sent for histopathological examination.
Ultrasonography of the urinary bladder showing a cystic lesion with an isoechoic wall occluding the right vesicoureteric junction.
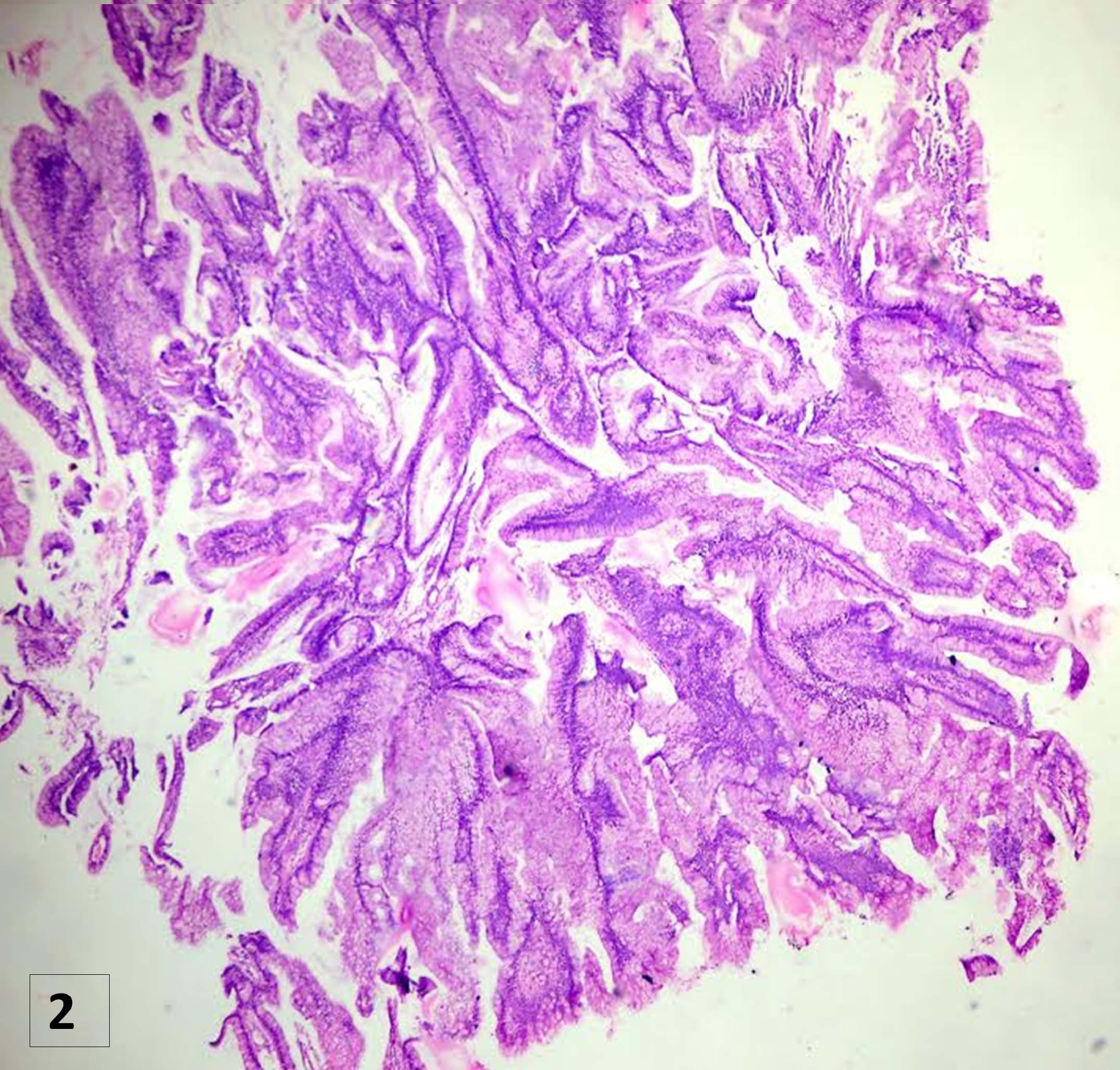
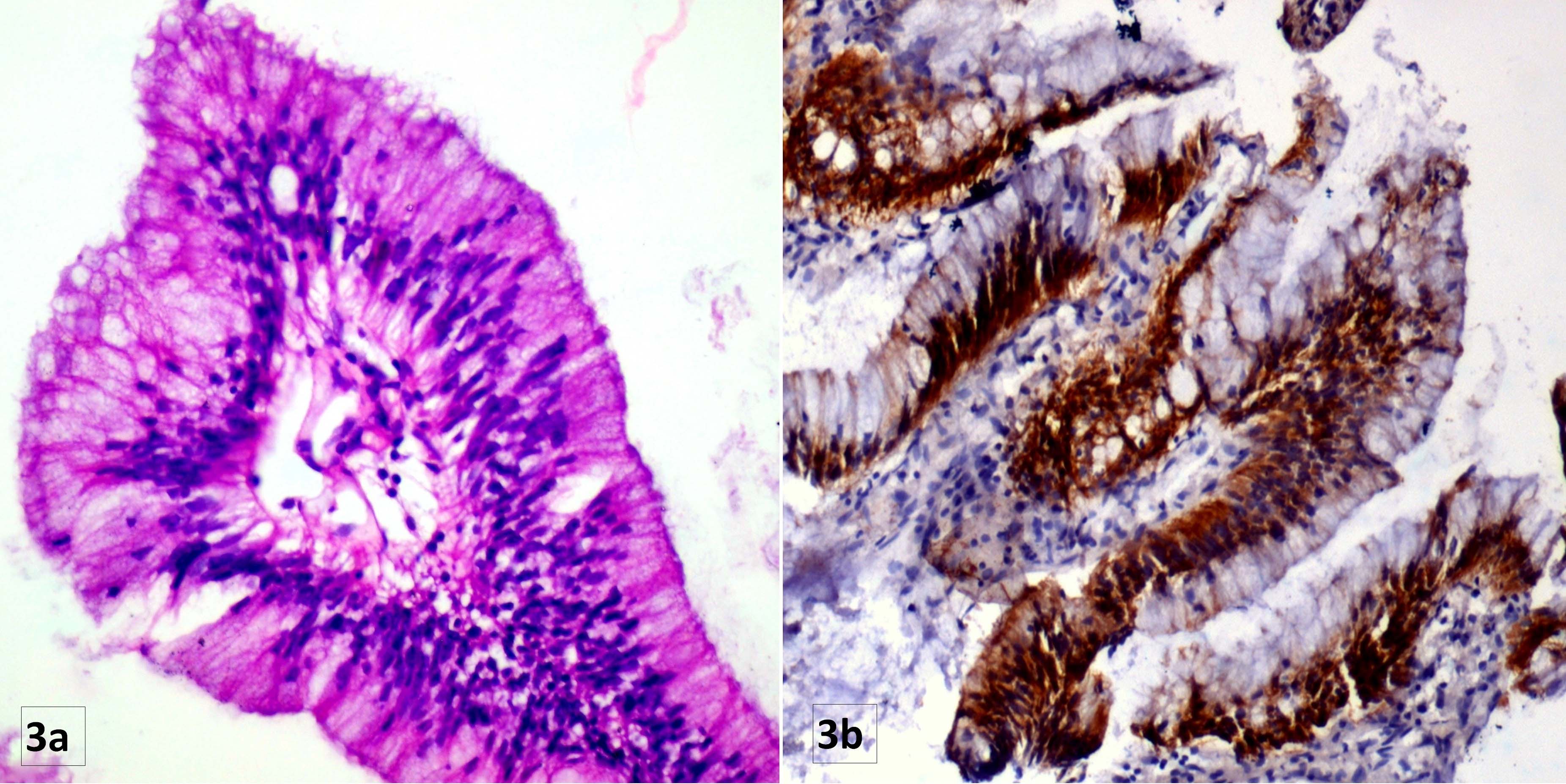
On gross examination, a single polypoidal structure measuring 6 mm x 5 mm was seen. Microscopy revealed a mass with fronds or papillary architecture and fibrovascular cores to the papillae [Table/Fig-2]. The papillae were lined by pseudostratified tall columnar, mucus secreting epithelium with bland nuclear features [Table/Fig-3a]. Stratification of the nuclei and nuclear crowding were seen, but no nuclear atypia or nuclear features of malignancy were present. Immunohistochemistry showed strong positivity for CK20 [Table/Fig-3b]. A diagnosis of pure villous adenoma of the right vesicoureteric junction leading to pyonephrosis of the right kidney was made. A nephrectomy was done a month after the excision of villous adenoma. Our latest follow-up was seven months after the diagnosis of adenoma, where the patient was disease free.
Scanner view showing fronds or papillary architecture with fibrovascular cores to the papillae (H&E 4X).
a) High power magnification showing a papilla with pseudostratified tall columnar, mucus secreting epithelium with bland nuclear features (H&E 40X); b) Immunohistochemistry with Cytokeratin 20 shows strong positivity in the epithelium (IHC 40X).
Discussion
Villous adenomas are benign glandular neoplasms that can occur anywhere in the urinary tract but they have been identified mainly in the urinary bladder, urethra, prostate and urachus [1]. They share morphological similarities with the villous adenomas of the gastrointestinal tract. Only two case series and around 20 scattered case reports of villous adenoma in the urinary tract have been published in English literature [2]. Villous adenomas have however not been reported at the vesicoureteric junction. These lesions usually occur in the elderly males from 53 to 93 years, with an average age of 69.6 years [2]. Villous adenomas can present with haematuria, irritating symptoms and occasionally with mucusuria [3]. Our patient was a 50-year-old lady who came to seek medical attention for pain in right flank and fever with chills due to pyonephrosis of right kidney.
As regards the aetiology, villous adenomas are believed to arise from the parts of cloacal rests which persists after embryogenesis in the adult urinary bladder and urachus, and which can develop into an epithelial neoplasm [4]. During embryogenesis, the distal colorectum and the bladder both develop from the cloaca. The urorectal septum develops within the cloaca and partitions it into rectum and anal canal dorsally and lower genitourinary tract ventrally [4]. This explains why villous adenomas of urinary tract and gastrointestinal tract are morphologically and cytogenetically similar. An alternative theory suggests that villous adenoma is the product of a sequence of chronic irritation-metaplasia-dysplasia-carcinoma. Presence of neutral mucins, acidic sulphomucins and sialomucins within the villous adenoma and in cystitis glandularis and a similar genetic makeup between villous adenoma and the dysplastic regions of flat metaplastic mucosa favours this theory [5,6].
Villous adenomas have been reported to coexist or be associated with or show transformation into malignant tumours like adenocarcinoma in situ, infiltrating adenocarcinomas and urothelial carcinomas [3]. No recurrences are seen in the pure villous adenomas.
The histopathology of pure villous adenoma is quite diagnostic and is characterised by fronds lined by benign pseudostratified epithelium with nuclei polarised towards the basement membrane. Presence of coexisting urothelial carcinoma and adenocarcinoma should always be looked for since villous adenomas can coexist with and also undergo malignant transformation. The main differential diagnosis that can be considered for villous adenoma is papillary urothelial carcinoma with villo-glandular differentiation. No morphological features of urothelial carcinoma and no hint of any atypia were seen in our case. Immunohistochemistry for villous adenoma shows Cytokeratin 20 (CK20) (100%) positivity, while cytokeratin 7, carcinoembryonic antigen and epithelial membrane antigen can also show positivity [7]. In contrast to intestinal villous adenomas about 50% of urinary tract villous adenomas exhibit positive results for cytokeratin 7 [3]. In our case lesion showed strong CK20 positivity.
Isolated pure villous adenoma, though rare, has a good prognosis and cystoscopic excision is curative [1]. This patient had a nephrectomy done a month after the villous adenoma was excised, and the nephrectomy showed acute on chronic pyelonephritis with pyonephrosis and calculi. The patient is disease free and well currently, seven months after the excision of the adenoma.
Conclusion
Pure villous adenomas are difficult to diagnose without the help of histopathology. They cannot be differentiated on cystoscopy from the more sinister urothelial carcinomas. Histopathology also helps to diagnose villous adenomas which co-exist with malignancies or which may have undergone malignant transformation.
[1]. Sung W, Park BD, Lee S, Chang SG, Villous adenoma of the urinary bladderInt J Urol 2008 15(6):551-53. [Google Scholar]
[2]. Wang J, Manucha V, Villous adenoma of the urinary bladder: a brief review of the literatureArch Pathol Lab Med 2016 140(1):91-93. [Google Scholar]
[3]. Seibel JL, Prasad S, Weiss RE, Bancila E, Epstein JI, Villous adenoma of the urinary tract: a lesion frequently associated with malignancyHum Pathol 2002 33(2):236-41. [Google Scholar]
[4]. Wright HB, McFarlane DJ, Carcinoma of the urachusAm J Surg 1955 90:693-97. [Google Scholar]
[5]. Channer JL, Williams JL, Henry L, Villous adenoma of the bladderJ Clin Pathol 1993 46(5):450-52. [Google Scholar]
[6]. Adegboyega PA, Adesokan A, Tubulovillous adenoma of the urinary bladderMod Pathol 1999 12(7):735-38. [Google Scholar]
[7]. Cheng L, Montironi R, Bostwick DG, Villous adenoma of the urinarytract: a report of 23 cases, including 8 with coexistent adenocarcinomaAm J Surg Pathol 1999 23(7):764-71. [Google Scholar]